He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Willowpharma.com.au
Ceftazidime SXP Product Information NAME OF THE MEDICINE Proprietary names: Non proprietary names: Ceftazidime (as pentahydrate) powder for injection 1 g
Ceftazidime (as pentahydrate) powder for injection 2 g
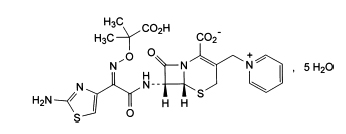
Chemical name: (6R,7R)-7-[[(Z)-2-(2-aminothiazol-4-yl)-2-[(1-carboxy-1-methylethoxy)imino]acetyl]amino]-
8-oxo-3-[(1-pyridinio)methyl]-5-thia-1-azabicyclo-[4.2.0]oct-2-ene-2-carboxylate pentahydrate Molecular formula: C22H22N6O7S2.5H2O Molecular weight: 636.6 Structure: The chemical structure of ceftazidime pentahydrate is: CAS Number: 78439-06-2 DESCRIPTION Ceftazidime is a cephalosporin antibiotic for use by injection only. It is a white or almost white crystalline
powder in vials containing ceftazidime as pentahydrate, with sodium carbonate anhydrous. On the addition of
water for injections, Ceftazidime SXP injection dissolves with effervescence to produce a solution for injection. Ceftazidime SXP injection contains approximately 52 mg (2.3 mEq) of sodium per g of ceftazidime. Ceftazidime
pentahydrate 116 mg is equivalent to ceftazidime anhydrous 100 mg. For laboratory tests associated with ceftazidime administration, ceftazidime pentahydrate should be used. PHARMACOLOGY Actions: Antibiotic Microbiology: Ceftazidime is bactericidal in action, exerting its effect on target cell wall proteins and causing
inhibition of cell wall synthesis. It is stable to most beta-lactamases produced by Gram positive and Gram
negative organisms and consequently is active against many ampicillin and cephalothin resistant strains (but
not methicillin resistant strains). Ceftazidime has been shown to have in vitro activity against the following
organisms. Gram negative organisms.Pseudomonas aeruginosa, Pseudomonas sp. (other), Klebsiella pneumoniae, Klebsiella sp. (other), Proteus mirabilis, P. vulgaris, Morganella morganii (formerly P. morganii), P. rettgeri,
Providencia sp., Escherichia coli, Enterobacter sp., Citrobacter sp., Serratia sp., Acinetobacter sp., Neisseria gonorrhoeae, N. meningitidis, Haemophilus influenzae (including ampicillin resistant strains). Gram positive organisms.Staphylococcus aureus (methicillin sensitive strains), Staph. epidermidis
(methicillin sensitive strains), Micrococcus sp., Streptococcus pyogenes, Streptococcus group B, Strep. pneumoniae, Streptococcus sp. (excluding Strep. faecalis). Ceftazidime is not active in vitro against methicillin
resistant Staphylococci, Streptococcus faecalis and many other Enterococci, Listeria monocytogenes,
Campylobacter sp. or Clostridium difficile. In vitro, the activities of ceftazidime and aminoglycoside antibiotics in combination have been shown to be
at least additive; there is evidence of synergy in some strains tested. This property may be important in the
treatment of febrile neutropenic patients. Susceptibility tests: Disc Susceptibility Test Dilution or diffusion techniques- either quantitative (MIC) or breakpoint, should be used following a regularly
updated, recognised and standardised method (eg Clinical and Laboratory Standards Institute [CLSI formerly
NCCLS]). Standardised susceptibility test procedures require the use of laboratory control microorganisms to
control the technical aspects of the laboratory procedures. A report of “Susceptible” indicates that the pathogen is likely to be inhibited if the antimicrobial compound in
the blood reaches the concentrations usually achievable. A report of “Intermediate” indicates that the result should be considered equivocal, and if the microorganism is
not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies
possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where
high dosage of drug can be used. This category also provides a buffer zone, which prevents small-uncontrolled
technical factors from causing major discrepancies in interpretation. A report of “Resistant” indicates that the pathogen is not likely to be inhibited if the antimicrobial compound in
the blood reaches the concentrations usually achievable; other therapy should be selected. Note: The prevalence of resistance may vary geographically for selected species and local information on
resistance is desirable, particularly when treating severe infections. Pharmacokinetics: Absorption of ceftazidime after oral administration is negligible, therefore Ceftazidime SXP
is intended for parenteral use only. In humans, after an intravenous bolus injection of 500 mg, 1 g and 2 g or single intramuscular administration
of 500 mg and 1 g, the mean peak serum levels obtained are shown in the tables below. Mean peak serum concentrations of Ceftazidime following IV administration Ceftazidime IV dose Serum concentrations (mg/L) 5 minutes
Mean peak serum concentrations of Ceftazidime following IM administration Ceftazidime IM dose Serum concentrations (mg/L)
The serum half-life in adults with normal renal function is about 1.8 hours (1.2 to 2.9 hours). This may be
prolonged to 20 to 35 hours in anuric patients. In neonates, the serum half-life of ceftazidime can be three to
four times greater than that measured in adults. The serum protein binding of ceftazidime is low at about 10%. Ceftazidime is not metabolised in the body and is excreted unchanged in the active form into the urine by
glomerular filtration. In the presence of normal renal function approximately 80 to 90% of the dose is recovered
in the urine within 24 hours. Less than 1% is excreted via the bile. The mean maximum concentrations of ceftazidime in bone, heart, bile, sputum, aqueous humour and synovial,
pleural and peritoneal fluids were in excess of the in vitro minimum inhibitory levels for susceptible organisms
(see Susceptibility tests). Transplacental transfer of the antibiotic readily occurs. Ceftazidime penetrates the
intact blood-brain barrier poorly and low levels are achieved in the cerebrospinal fluid (CSF). The pharmacokinetics of ceftazidime are similar whether it is administered by a single or by repeat dosage. Concurrent oral administration of probenecid did not affect the serum levels or urinary recoveries of
ceftazidime. The pharmacokinetics of ceftazidime were not affected when administered intramuscularly with
0.5% lignocaine INDICATIONS Treatment of single and mixed infections caused by susceptible aerobic organisms with suspected or
documented resistance to other antimicrobials, but not to ceftazidime; as an alternative to aminoglycosides
in pseudomonal infection in patients in whom aminoglycoside toxicity is a cause for concern and other
antipseudomonal antibiotics cannot be used. Indications include the following:
• Severe infections in general. For example: septicaemia (including neonatal sepsis), bacteraemia; in
patients in intensive care units with specific problems, e.g. infected burns.
• Respiratory tract. For example: pneumonia, bronchopneumonia, infected pleurisy, infected bronchiectasis • Severe ear, nose and throat infections. For example: otitis media, mastoiditis. • Urinary tract. For example: acute and chronic pyelonephritis, pyelitis, cystitis, urethritis (bacterial only);
infections associated with bladder and renal stones.
• Skin and soft tissue. For example: erysipelas, abscesses, cellulitis, infected burns and wounds, mastitis. • Gastrointestinal and abdominal. For example: intra-abdominal abscesses, enterocolitis. • Bone and joint. For example: osteitis, osteomyelitis, septic arthritis, infected bursitis. CONTRAINDICATIONS Hypersensitivity to cephalosporins or a major allergy to penicillin (anaphylaxis, angioneurotic oedema,
urticaria). Lignocaine should not be used as a diluent for intramuscular injection in patients who are hypersensitive to
lignocaine. PRECAUTIONS Anaphylactic reactions As with other beta-lactam antibiotics, before therapy with ceftazidime is instituted, careful inquiry should be
made for a history of hypersensitivity reactions to ceftazidime, cephalosporins, penicillins or other drugs.
Ceftazidime should be given only with special caution to patients with mild type I or immediate hypersensitivity
reactions to penicillin. If an allergic reaction to ceftazidime occurs, discontinue the drug. Serious
hypersensitivity reactions may require adrenaline, hydrocortisone, antihistamine or other emergency measures. Pseudomembranous colitis Antibiotic associated pseudomembranous colitis has been reported with many antibiotics including ceftazidime.
A toxin produced by Clostridium difficile appears to be the primary cause. The severity of the colitis may range
from mild to life threatening. It is important to consider this diagnosis in patients who develop diarrhoea
or colitis in association with antibiotic use (this may occur up to several weeks after cessation of antibiotic
therapy). Mild cases usually respond to drug discontinuation alone. However, in moderate to severe cases
appropriate therapy with a suitable oral antibacterial agent effective against Cl. difficile should be considered.
Fluids, electrolytes and protein replacement should be provided when indicated. Drugs that delay peristalsis, e.g. opiates and diphenoxylate with atropine (e.g. Lomotil), may prolong and/or
worsen the condition and should not be used. Cl. difficile infection rarely manifests as diarrhoea in neonates. Other Prescribing ceftazidime in the absence of a proven or strongly suspected bacterial infection or a prophylactic
indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-
resistant bacteria. Inducible type I beta-lactamase resistance has been noted with some organisms (e.g., Enterobacter spp.,
Pseudomonas spp., and Serratia spp.). As with other extended-spectrum beta-lactam antibiotics, resistance
can develop during therapy, leading to clinical failure in some cases. When treating infections caused by these
organisms, periodic susceptibility testing should be performed when clinically appropriate. If patients fail to
respond to monotherapy, an aminoglycoside or similar agent should be considered. Cephalosporins may be associated with a fall in prothrombin activity. Those at risk include patients with
renal and hepatic impairment, or poor nutritional state, as well as patients receiving a protracted course of
antimicrobial therapy. Prothrombin time should be monitored in patients at risk and exogenous vitamin K
administered as indicated. Ceftazidime should be prescribed with caution in individuals with a history of gastrointestinal disease,
particularly colitis. Distal necrosis can occur after inadvertent intra-arterial administration of ceftazidime. Peak concentrations of ceftazidime in the CSF are considerably lower than those in the plasma. Its use in the
treatment of infections of the central nervous system, e.g. meningitis, brain abscess, is not advised at present. Vials of Ceftazidime SXP injection are supplied with carbon dioxide as a protective gas. A positive pressure
is produced on reconstitution due to the release of further carbon dioxide. See Dosage and Administration for
recommended techniques of reconstitution. Impaired renal function. Ceftazidime has shown some evidence of renal toxicity in animals. Clinical studies
have shown only transient elevations in serum urea and serum creatinine. It is excreted almost entirely by
glomerular filtration and its half-life is prolonged in patients with impaired renal function. In such patients,
dosage adjustment may be required in order to avoid the clinical consequences of elevated antibiotic levels.
Neurological sequelae have occasionally been reported when the dose has not been reduced appropriately (see
Dosage and Administration). Impaired hepatic function. Transient rises in hepatic enzymes have been noted in some patients given
ceftazidime, so careful monitoring of hepatic function is advised when any dysfunction exists. Repeated use
of lignocaine hydrochloride as a diluent for intramuscular use should be avoided in patients with severe liver
disease or decreased hepatic blood flow, due to the possibility of lignocaine toxicity resulting from decreased
metabolism and consequent accumulation. Use in pregnancy. (Category B1) The safety of ceftazidime in pregnancy has not been established, although
animal studies have not produced evidence of embryopathic or teratogenic effects attributable to ceftazidime.
Therefore, it may be administered during known or suspected pregnancy only if, in the opinion of the treating
doctor, the expected benefits outweigh the possible risks. Use in lactation. Ceftazidime is excreted in human breast milk in low concentrations. Therefore, it is not
recommended for breastfeeding mothers unless the expected benefits to the mother greatly outweigh any
potential risk to the infant. Use in children. Ceftazidime is effective in the treatment of neonatal infections caused by susceptible
organisms. INTERACTIONS: Interactions with other medicines Aminoglycoside antibiotics and/or diuretics: Nephrotoxicity has been reported following concomitant
administration of cephalosporins with aminoglycoside antibiotics or potent diuretics such as furosemide.
Renal function should be carefully monitored, especially if higher dosages of the aminoglycosides are
to be administered or if therapy is prolonged, because of the potential nephrotoxicity and ototoxicity of
aminoglycosidic antibiotics. Nephrotoxicity and ototoxicity were not noted when ceftazidime was given alone
in clinical trials. Oral Contraceptives: In common with other antibiotics, ceftazidime may affect the gut flora, leading to lower
oestrogen reabsorption and reduced efficacy of combined oral contraceptives. Chloramphenicol has been shown to be antagonistic to beta-lactam antibiotics, including ceftazidime, based on
in vitro studies and time kill curves with enteric gram-negative bacilli. Due to possibility of antagonism in vivo,
particularly when bactericidal activity is desired, this drug combination should be avoided. Drug/Laboratory Test Interactions The administration of ceftazidime may result in a false-positive reaction for glucose in the urine when using
CLINITEST® tablets, Benedict’s solution, or Fehling’s solution. It is recommended that glucose tests based on
enzymatic glucose oxidase reactions (such as CLINISTIX®)be used. ADVERSE EFFECTS Clinical trial experience has shown that ceftazidime is generally well tolerated. Adverse reactions are infrequent
and include the following. Local. Phlebitis or thrombophlebitis with intravenous administration; pain and/or inflammation after
intramuscular injection. Hypersensitivity. Maculopapular or urticarial rash, fever, pruritus; very rarely angioedema and anaphylaxis
(including bronchospasm and hypotension), erythema multiforme, Stevens-Johnson syndrome and toxic
epidermal necrolysis. Gastrointestinal. Diarrhoea, nausea, vomiting, abdominal pain and very rarely oral thrush or colitis.
Pseudomembranous colitis has been reported. Central nervous system. Headache, dizziness, paraesthesia and bad taste. There have been reports of
neurological sequelae including tremor, myoclonia, convulsions, encephalopathy and coma occurring in
patients with renal impairment in whom the dose of ceftazidime has not been appropriately reduced. Genitourinary. Candidiasis, vaginitis. Renal. Transient elevations of blood urea, serum urea and/or serum creatinine have been observed
occasionally. Hepatic. Elevations in one or more of the hepatic enzymes, AST, ALT, LDH, GGT and alkaline phosphatase, may
occur. Haematological. Eosinophilia, positive Coombs’ test, thrombocytosis; very rarely, transient leucopenia,
haemolytic anaemia, neutropenia, thrombocytopenia and lymphocytosis have been seen. Other. Hot flushes, superficial desquamation around injection site. DOSAGE AND ADMINISTRATION Note. Vials of Ceftazidime SXP injection are supplied with carbon dioxide as a protective gas. A positive
pressure is produced on reconstitution due to the release of further carbon dioxide. Ceftazidime is to be used by the parenteral route, the dosage depending upon the severity, sensitivity and type
of infection, and the age, weight and renal function of the patient. Ceftazidime SXP is for single use in one patient only. Adults. The adult dosage range for ceftazidime is 1 to 6 g daily, for instance, 500 mg, 1 g or 2 g given every
twelve or eight hours by intravenous or intramuscular injection. In urinary tract infections and in many less
serious infections, 500 mg or 1 g every twelve hours is usually adequate. In the majority of infections, 1 g
every eight hours or 2 g every twelve hours should be given. In very severe infections, 2 g every eight or twelve
hours should be administered. Individual doses exceeding 1 g should be administered intravenously. Children. Over 12 months. The usual dosage range for children aged over 12 months is 25 to 100 mg/kg/day
(up to a maximum of 6 g/day), given as two or three divided doses. The maximum daily dosage (6 g) may be
given to children with very serious infections, e.g. those who are immunocompromised or who suffer from
cystic fibrosis. Neonates, infants up to 12 months. 25 to 100 mg/kg/day in two divided doses. In neonates the serum half-life
of ceftazidime can be three to four times greater than that measured in adults. Use in the elderly. In view of the reduced clearance of ceftazidime in elderly patients, the daily dosage should
be adjusted according to renal function. Impaired renal function. Adults. Ceftazidime is excreted by the kidneys almost exclusively by glomerular
filtration. Therefore, in patients with impaired renal function it is recommended that the dosage of ceftazidime
should be reduced to compensate for its slower excretion, except in mild impairment, i.e. glomerular filtration
rate (GFR) greater than 50 mL/minute. In patients with suspected renal insufficiency, an initial loading dose of
ceftazidime 1 g may be given. An estimate of GFR should be made to determine the appropriate maintenance
dose. Recommended maintenance doses are shown in Table 1. Table 1: Recommended maintenance doses of ceftazidime in renal insufficiency Creatinine clearance Approx. serum Recommended unit Frequency of dosing (mL/min) creatinine* dose of ceftazidime (g) (micromol/L)
*These values are guidelines and may not accurately predict renal function in all patients, especially in the
elderly in whom the serum creatinine concentration may overestimate renal function.
In patients with severe infections who would normally receive ceftazidime 6 g daily were it not for renal
insufficiency, the unit dose given in the table above may be increased by 50% or the dosing frequency
increased appropriately. In such patients it is recommended that ceftazidime serum levels should be monitored
and trough levels should not exceed 40 mg/L. When only serum creatinine is available, the following formula
(Cockcroft’s equation) may be used to estimate creatinine clearance. The serum creatinine should represent a
steady state of renal function. Calculation of creatinine clearance (mL/minute) Men:
Bodyweight (kg) x (140 – age in years) x 0.0885
Women: Multiplication of the result of the above equation by 0.85 Children. In children the creatinine clearance should be adjusted for body surface area or lean body mass and
the dosing frequency reduced in cases of renal insufficiency as for adults. The serum half-life of ceftazidime
during haemodialysis is approximately three hours. The appropriate maintenance dose of ceftazidime should
be repeated following each haemodialysis period. Continuous ambulatory peritoneal dialysis (CAPD) removed
approximately 10% of the antibiotic when the dwell time was four to six hours. Administration. Ceftazidime may be given intravenously or by deep intramuscular injection into a large muscle
mass such as the upper outer quadrant of the gluteus maximus or lateral part of the thigh. Reconstitution. Ceftazidime SXP may be constituted with water for injections or, for intramuscular injection,
with 0.5% lignocaine. See Table 2 for additive volumes and solution concentrations. Table 2: Preparation of solution Vial size/route Amount of diluent to be added Approximate concentration
* Note: addition should be in 2 stages (see text)
All sizes of vials of Ceftazidime SXP injection are supplied with carbon dioxide as a protective gas. A positive
pressure is produced on reconstitution due to the release of further carbon dioxide. For ease of use, it is
recommended that the following techniques of reconstitution are adopted. 1 g intramuscular/ intravenous and 2 g intravenous bolus vials. Insert syringe needle through vial closure
and inject recommended volume of diluent. Remove the syringe needle. Shake to dissolve; carbon dioxide is
released and a clear solution obtained in about one to two minutes.
Invert the vial. With the syringe plunger fully depressed, insert the needle through vial closure and withdraw
the total volume of solution into the syringe (the pressure in the vial may aid withdrawal). Ensure that the
needle remains within the solution and does not enter the headspace. The withdrawn solution may contain
small bubbles of carbon dioxide; they may be disregarded. 2 g intravenous infusion vial. This vial may be reconstituted for short intravenous infusion (e.g. up to 30
minutes) as follows. Insert syringe needle through the vial closure and inject 10 mL of diluent. Remove the
Shake to dissolve; carbon dioxide is released and a clear solution obtained in about one to two minutes.
Insert a gas relief needle through vial closure to relieve internal pressure and, with gas relief in position, add a
further 40 mL of diluent. Remove the gas relief needle and syringe needle; shake the vial and set up for infusion
use in the normal way. Note. To preserve product sterility, it is important that a gas relief needle is not inserted through the vial
closure before the product has dissolved.
These solutions may be given directly into the vein or introduced into the tubing of a giving set if the patient is
receiving parenteral fluids. Solutions of Ceftazidime SXP injection reconstituted in water for injections may be stored for up to two hours
below 25°C or for 24 hours under refrigeration (2 to 8°C). Do not freeze. Some increase in the colour of prepared solutions of Ceftazidime SXP for injection may occur on storage. It is,
however, advisable to use the reconstituted product as soon as possible. Ceftazidime is compatible with the intravenous fluids shown below. Solutions at concentrations between 1 mg/
mL and 40 mg/mL in these infusion fluids may be stored for up to two hours below 25°C or for 24 hours under
refrigeration (2 to 8°C): 0.9% Sodium Chloride, Ringer Sodium Lactate solution, 5% Dextrose, Dextran 40 10%
in 0.9% Sodium Chloride, Dextran 70 6% in 0.9% Sodium Chloride. Sodium bicarbonate injection is not recommended as a diluent. Ceftazidime injection may be stored for up to two hours below 25°C or for 24 hours under refrigeration (2 to
8°C) at concentrations between 0.05 mg/mL and 0.25 mg/mL in Intraperitoneal Dialysis solution. Ceftazidime injection may be stored for up to two hours below 25°C or for 24 hours under refrigeration (2 to
8°C) when admixed at 4 mg/mL with potassium chloride 10 mEq/L or 40 mEq/L in 0.9% Sodium Chloride, or
heparin (10 and 50 units/mL) in 0.9% sodium chloride. Ceftazidime and aminoglycosides should not be mixed in the same giving set or syringe. Precipitation has been reported when vancomycin has been added to ceftazidime in solution. Therefore, it
would be prudent to flush giving sets and intravenous lines between the administration of these two agents. Protect from light. Solutions should be clear and may range from colourless to yellow depending on concentration, diluent and
storage conditions used. Within the stated recommendations, product potency is not adversely affected by
such colour variations. OVERDOSAGE Symptoms. Overdosage can lead to neurological sequelae including encephalopathy, convulsions and coma. Treatment. Ceftazidime can be removed by haemodialysis. Contact the Poisons Information Centre on 131126 for advice on management. PRESENTATION AND STORAGE CONDITIONS Vial (powder for reconstitution), 1 g (for IM or IV use): 5’s; 2 g (for IV use): 5’s. Store below 25°C. Protect from light. Shelf life: 2 years. NAME AND ADDRESS OF SPONSOR Southern Cross Pharma Pty Ltd 56 Illabunda Drive Malua Bay, NSW, 2536 POISON SCHEDULE S4 DATE OF TGA APPROVAL 14/10/2008
All Correspondence this week responds to the expansion of diagnostic categories and Barbara Sahakian and Sharon Morein- the invention of new pathological conditions Zamir’s Commentary ‘Professor’s little helper’ — sometimes to cover cases that in earlier ( Nature 450, 1157–1159; 2007) and the times would have been regarded as within related discussion at http://
La tecnologia migliora la qualita’ della vita. Sveglia radiocontrollata che proietta l’ora sul muro; Colazione preparata con il microonde, e poi via in auto verso una nuova giornata lavorativa. L’autoradio, ci mette al corrente delle ultime novita’ dal mondo. Il badge personale permette l’accesso al parcheggio riservato ai dipendenti. In ufficio, il P.C. ci saluta con una dolce melodia.
 Ceftazidime SXP
Ceftazidime SXP