He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Theinformedpatient.in
Companion diagnostics and personalized medicine: A review of molecular diagnostic applications
Mathew W. Moore1, Deepti Babu2, and Philip D. Cotter1,* ResearchDx, Irvine, California, USA. 2Department of Medical Genetics, University of Alberta,
ABSTRACT
well established [1, 2]. The advantages of approaching medicine in this way are theoretically
Personalized medicine is the customization of
treatment based on a patient’s hereditary or
clear; personalized medicine has the potential to
somatic genetics and holds the promise of more efficiently, effectively, and safely direct
revolutionizing healthcare. Companion diagnostics,
health care than traditional non-targeted approaches.
many of which are molecular genetics assays, are
While the rate of progress has clearly increased, there are still significant technical and regulatory
critical tools in the implementation of personalized
medicine. Information derived from these tests
hurdles to overcome. Several guidance documents
provides for customizing specific therapies based from regulatory organizations worldwide have
on the genetics of the disease. While the benefits
attempted to address these challenges, and no
are clear, the path to a successful companion doubt more will be presented in the near future
diagnostic has required a forging of new alliances
between drug and diagnostic developers, clinical
Companion diagnostics are increasingly relied
laboratories, physicians, pathologists, and healthcare upon to ensure the effective, safe development
providers. Molecular genetic companion diagnostic
and use of a personalized therapeutic. Multiple
assays are becoming more relevant and important
liaisons and partnerships between key stakeholders
in an environment of increased regulatory guidance
are needed in this complex, dynamic process.
in their development and application. Here, we
Many successful companion diagnostics are
review key molecular genetics companion diagnostic genetic tests - particularly molecular diagnostics -
tests and their applications in personalized medicine.
and this speaks to their high impact and relevance
KEYWORDS: personalized medicine, genetic, Personalized medicine and the “new” genomics
“Personalized medicine” is a phrase first coined in
INTRODUCTION
the 1990s, although the concept pre-dated this
The concept of personalized medicine, whereby [4, 5]. Achieved successfully, personalized medicine disease diagnosis, treatment and prevention are
harnesses power from innate biological information
customized to one’s genetic composition, is now
to direct appropriate therapies for appropriate
patients - a goal that maximizes key components
of effectiveness, efficiency, and safety.
*Address correspondence to: Dr. Philip D. Cotter,
ResearchDx, 13766 Alton Parkway, Suite 147,
Independent of the Human Genome Project,
personalized medicine efforts initially began with
a consortium of the world’s largest pharmaceutical
companies and scientists, created to identify Early strategic partnerships are necessary to create
natural genetic differences between people [4].
personalized therapeutics. Few pharmaceutical
The goal was to correlate informative genetic companies have depth of experience in the biomarkers with disease symptoms, or serious diagnostics arena. Partnerships can address side effects to certain medications. Drug experimental design, assay discovery, assay developers then hoped to develop more effective,
validation, marketing and commercialization [3].
safer drugs to target these patient populations.
However, some of these partnerships are not part
of current pharmaceutical company outsourcing
More recently, the interest in personalized
practices. In addition, early alliances are difficult
medicine has increased substantially; based on
because the value of the drug and its diagnostic
PubMed searches on the term ‘personalized
are difficult to predict [3]. These and other factors
medicine’, a 2011 publication found that the
bring about several business challenges.
number of scientific publications on the subject
has shown an exponential growth in the period
Commercially, there are several challenges for a
from 1999 to 2010 [6]. Kongkaew et al. [7]
companion diagnostic. The total market for the
estimated that more than 5% of hospital therapeutic needs to be large enough to not only admissions are associated with adverse reactions
justify the development cost of the therapeutic
to prescribed drugs. Many of these are due to
itself, but also now the cost of development for
individual genetic differences that render one
the associated companion diagnostic. In addition,
hypersensitive to the drug, or unable to one has to market the value of both the therapeutic
and the diagnostic. A companion diagnostic has
the potential to reduce the market size for a
Challenges in the drug development process
therapeutic by limiting the patient population.
Responses from the larger pharmaceutical and Similarly, in an extreme case the companion
biotechnology companies to create personalized
diagnostic may leave the physician without a
therapeutics have been lower than expected, based
viable therapeutic treatment. These issues can
on interest level. Success rates in bringing these
make pharmaceutical companies less commercially
drugs to market have also been low. A number of
motivated to pursue a personalized therapeutic.
scientific, strategic, commercial, and regulatory
Regulatory factors can also bring challenges,
factors have been attributed to this [9].
as there are inefficiencies in the current drug
Jorgensen et al. [6] argued that the initial “one
development process. The co-submission of a
drug for one disease” model does not fit the
therapeutic and diagnostic complicates the
clinical reality of heterogeneous disease regulatory submission process and can lead to mechanisms at the molecular level. As a result,
some diseases have not been as amenable to Historically, there were few regulatory guidance
personalized medicine, as was initially postulated.
Scientifically, it has also been more difficult to
diagnostic co-development. More recently,
identify and validate biomarkers in as timely a
regulatory agencies have responded with guidance
fashion than the industry initially expected. While
documents, attempting to inform best practices,
the drug development and regulatory process is
and to provide clarity and consistency in assay
well known and understood, the development of a
successful biomarker requires an understanding of
several success factors including biomarker
Regulatory responses about companion
availability, robust technical assay validation, the
diagnostics
importance of demonstrating clinical utility, and
the ability to bring an investment-positive Regulatory agencies are quickly recognizing that
commercial value proposition to the table [3]. companion diagnostics can be the key to a safe, This is extremely difficult to find without successful personalized therapeutic. In draft partnering with several organizations, introducing
guidance from July 2011, the FDA indicated that,
several logistical challenges to the process.
“in most circumstances, if use of an in vitro
Genetic tests as companion diagnostics 25 companion diagnostic device (IVD companion the colon, lung, breast and other sites [1]. These
diagnostic device) is essential for the safe and
companion diagnostics typically identify somatic
effective use of a therapeutic product, (it and its) mutations identified in tumor cells, which help
therapeutic product should be approved or cleared
direct use of an appropriate therapeutic (Table 1).
contemporaneously by FDA for the use indicated
in the therapeutic product labeling” [10]. The Recent successful genetic companion diagnostic
guidance also stated that, “the results of the IVD
tests in oncology
companion diagnostic device will be essential for
Crizotinib and non-small cell lung cancer
the safe and effective use of the therapeutic
Recently, rearrangements of the anaplastic
product, and its use will be stipulated in the
lymphoma kinase (ALK) gene were reported in
labeling of the therapeutic product.” Because the
non-small cell lung cancer (NSCLC) [16, 17].
IVD companion diagnostic was identified as Within three years, studies of ALK inhibition
essential for this purpose, it was noted that, “with
yielding dramatic response rates in patients with
some exceptions FDA does not believe it may
advanced NSCLC containing ALKrearrangements
approve a novel therapeutic product or new
were reported [16, 18, 19]. In pretreated patients
therapeutic product indication for use with an IVD
that generally have a 10% response rate to
companion diagnostic if the IVD companion conventional chemotherapy, treatment with the
diagnostic is not approved or cleared for that
oral ALK inhibitor crizotinib (Xalkori®) yielded
indication” [10]. Guidelines for the development
an overall response rate of 55% and an estimated
of IVDs also exist in the European Union (EU)
six-month, progression-free survival rate of 72%
Regulatory guidances put an increased focus and
Significantly, the mechanism of resistance was
relevance on the development of companion
associated with ALK kinase domain mutations,
diagnostics, many of which are genetic tests. substantiating that ALK was indeed the genetic
Gene-based and molecular diagnostics testing is
target of the personalized therapy [16]. This also
growing at a 30-50% rate, and it has been
reinforced that appropriate clinical application of
estimated that as many as 1,500 genes and 5,000
ALK-targeted therapy was absolutely dependent
proteins may be candidates for new molecular test
upon a companion diagnostic to identify patients
targets [12, 13]. It has also been recommended
most likely to respond. The FDA has since
that companion diagnostics be used at an early
approved the drug, and requires use of its
stage in the drug development process [9]. From
companion diagnostic; this is indicated in product
a financial perspective, molecular diagnostics
within the USA alone was valued at approximately $2.7 billion in 2006, and was expected to reach
Vemurafenib and metastatic malignant
$5 billion by 2010 (AGR 15%) [14]. Oncology
melanoma
molecular diagnostics was the fastest growing
The B-Raf proto-oncogene serine/threonine-
sector at that time and was predicted to increase
protein kinase (BRAF) gene is critical in the
by 30% each year, tripling from its 2005 level of
development of melanoma [20, 21]. Melanoma
$315 million to more than $1.35 billion by 2010
tumor cells with BRAF mutations contain
distinctive characteristics, such as unique
morphological variants, an age at diagnosis often
Personalized medicine in the oncology sector
before 55 years, and others [21]. A multi-centric
There has been significant progress for study reported that the treatment of metastatic
companion diagnostics and personalized medicine melanomas carrying the V600E mutation in
in the oncology sector. For example, the use of
BRAF with a selective small molecule inhibitor
pre-symptomatic genetic testing and “targeted PLX4032 (vemurafenib) resulted in complete or therapies” tailored to genetic profiles of tumors is
partial regression of disease in most patients
part of a recommended evaluation for cancers of
[20, 22]. From clinical trial studies, patients with
Drug manufac FDA approve Required companion diagnostic Genetic biomarker
Genetic tests as companion diagnostics 27 BRAF V600E mutation-positive melanoma drug metabolism. Metabolism in the liver by
receiving vemurafenib (Zelboraf™) showed
cytochrome P450s represents the most common
improved rates of overall and progression-free route of drug breakdown. Fast- and slow- survival, as compared to those receiving metabolizing variants due to mutations in these conventional therapy. This highlighted the enzymes can lead to under- and over-dosing of
importance of a molecular disease model focusing
drugs [8, 28]. The FDA approved Roche’s
on specific biomarkers, identified by companion AmpliChip™ microarray-based assay to identify
diagnostics, as bona fide targets that could benefit
melanoma patients [21]. The FDA subsequently
approved the drug and requires use of the
Known to mediate the metabolism of almost 25%
companion diagnostic prior to its administration;
of drugs, adverse events with nearly 30 drugs are
known to be related to drug accumulation in
patients carrying variants in these two enzymes
Key companion diagnostics outside the oncology sector
Recently, findings were published on the prediction
Genetic biomarkers identify risk for
of dose selection for warfarin after correlation
life-threatening drug side effects
Companion diagnostics for hereditary mutations algorithm [8, 30]. Under- or over-dosing with
are also becoming more widespread (Table 2). warfarin is the worldwide leading cause of Heterozygosity for the human leukocyte antigen
hospitalization related to adverse events. Variants
HLA-B*1502 allele, found almost exclusively in
in CYP2D9 and VKORC1 are known to influence
individuals from some parts of Asia, placed one the biologic breakdown of warfarin. Study results
at increased risk of life-threatening reactions have shown that the prediction of dose selection to carbamazepine, a commonly prescribed anti-
with a pharmacogenetic algorithm correlated well
convulsant in those geographical regions [25]. with empirically determined maintenance doses.
Once the risk for these serious reactions in those
In fact, this outperformed clinical prediction and
with the HLA-B*1502 allele became known, the standard dose estimates. This was particularly true FDA issued an alert, indicating that if an in the outlier population; patients with common individual tests positive for the allele … variants of the metabolizing enzymes fell within
“carbamazepine should not be started unless the
the range of standard dosing [8, 30]. The FDA has
expected benefit clearly outweighs the increased
been updating drug labels to include such genetic
risk of serious skin reactions.” (http://www. information where compelling data exist [8]. fda.gov.login.ezproxy.library.ualberta.ca/Drugs/D
New alliances are needed to ensure successful
rugSafety/PostmarketDrugSafetyInformationforPa
companion diagnostics
tientsandProviders/ucm124718.html). The FDA
then recommended an HLA-B*1502 companion
diagnostic to be performed prior to prescribing
diagnostic is complex, and is best achieved
carbamazepine to those from at-risk populations.
through a closely coordinated interaction between
A 2011 letter to the New England Journal of
diagnostic manufacturers, drug companies and
Medicine augmented this warning by stating, “Given
regulatory agencies [11]. More specifically, this
the availability of other elective therapeutic requires alliances between drug and diagnostic choices, it may be prudent to advise HLA-B*1502
developers, clinical laboratories, physicians,
carriers to avoid not only carbamazepine but also
pathologists, healthcare providers, and others
other structurally related anticonvulsants, such as
phenytoin, oxcarbazepine, and possibly lamotrigine.”
Although companion diagnostics have been
developed and approved in some therapeutic
Drug metabolism variances due to hereditary
areas, the regulatory process itself is still evolving.
mutations
Each companion diagnostic case is unique and
Other successful companion diagnostics are requires early interactions and planning to ensure
associated with hereditary mutations that affect
diagnostic
allele are at high risk for experiencing a
(s) Companion Indication Drug Manufacturer
Genetic tests as companion diagnostics 29
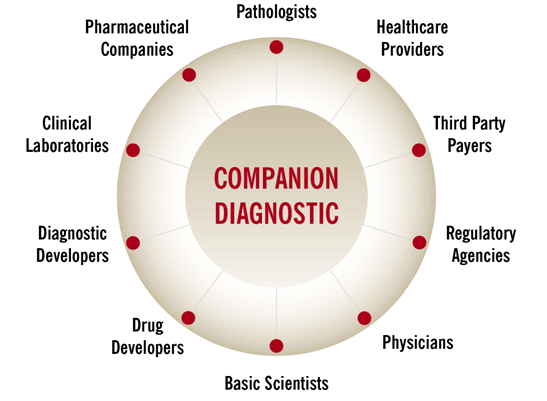
Figure 1. Necessary alliances to develop a successful companion diagnostic. CONCLUSION REFERENCES
The field of molecular diagnostics has advanced 1. Offit, K. 2011, Hum. Genet., 130, 3. rapidly since the first widespread introduction in
the early 1980s, and has exhibited continual
technological development. Thirty years into the
age of molecular diagnostics, the stunning pace of
advancement has shown no signs of abating,
with the next generation of technologies rapidly
Jorgensen, J. T. 2009, Oncologist, 14, 557.
becoming the method of choice for drug 6. Jorgensen, J. T. 2011, Drug Discov Today,
developers looking to include a companion
diagnostic into their drug development cycle.
Kongkaew, C., Noyce, P. R., and Ashcroft,
While drug development companies are becoming
D. M. 2008, Ann. Pharmacother, 42, 1017.
increasingly receptive to adding a diagnostic to
Bates, S. 2010, Drug Discov. Today, 15, 115.
their drug development cycle, many large 9. Papadopoulos, N., Kinzler, K. W., and
instructions are challenged by the implementation.
Current development relies heavily on in-house
technology, intellectual property, and expertise.
10. Services, U. S. D. o. H. a. H. 2011. Draft
However, development of a companion diagnostic
requires a complex and symbiotic collaboration
Administration Staff - In Vitro Companion
between public and private enterprise, research
institutions, diagnostics, drug development,
clinicians, patients and regulatory authorities. No
in vitro companion diagnostic devices,
one organization currently has the capabilities to
combine all of the required pieces, and only such
11. Nikolcheva, T., Jager, S., Bush, T. A., and
partnerships have the financial, scientific and
Vargas, G. 2011, Expert Rev. Mol. Diagn.,
technical capabilities necessary to complete this
12. Ross, J. S. 2011, Biomark Med., 5, 277.
13. Ross, J. S. and Ginsburg, G. S. 2002, Drug
20. Smalley, K. S. 2010, Curr. Opin. Investig.
14. Sannes, L. 2007, Molecular Diagnostics: A 21. de Souza, C. F., Morais, A. S., and
Rapidly Shifting Commercial and Technology
15. Administration, U. S. F. a. D. 2011, Table of
22. Flaherty, K. T., Puzanov, I., Kim, K. B.,
Pharmacogenomic Biomarkers in Drug Labels.
Ribas, A., McArthur, G. A., Sosman, J. A.,
16. Gerber, D. E. and Minna, J. D. 2010, Cancer
O'Dwyer, P. J., Lee, R. J., Grippo, J. F.,
17. Soda, M., Choi, Y. L., Enomoto, M.,
Takada, S., Yamashita, Y., Ishikawa, S.,
Fujiwara, S., Watanabe, H., Kurashina, K.,
Ishikawa, Y., Aburatani, H., Niki, T., 24. U. S. Food and Drug Administration
25. Chung, W. H., Hung, S. I., Hong, H. S.,
18. Choi, Y. L., Soda, M., Yamashita, Y., Ueno,
T., Takashima, J., Nakajima, T., Yatabe, Y.,
Wu, J. Y., and Chen, Y. T. 2004, Nature,
Ishikawa, Y., Kimura, H., Mitsudomi, T.,
26. Liao, W. P., Shi, Y. W., and Min, F. L.
Tanio, Y., and Mano, H. 2010, N. Engl. J.
27. Phillips, E. J. and Mallal, S. A. 2011, N.
19. Kwak, E. L., Bang, Y. J., Camidge, D. R.,
Shaw, A. T., Solomon, B., Maki, R. G., Ou,
28. Phillips, K. A., Veenstra, D. L., Oren, E.,
S. H., Dezube, B. J., Janne, P. A., Costa, D.
B., Varella-Garcia, M., Kim, W. H., Lynch,
T. J., Fidias, P., Stubbs, H., Engelman, J. A.,
29. Jain, K. K. 2005, Mol. Diagn., 9, 119.
Sequist, L. V., Tan, W., Gandhi, L., Mino-
30. Klein, T. E., Altman, R. B., Eriksson, N.,
Kenudson, M., Wei, G. C., Shreeve, S. M.,
Ratain, M. J., Settleman, J., Christensen, J.
G., Haber, D. A., Wilner, K., Salgia, R.,
Shapiro, G. I., Clark, J. W., and Iafrate, A. J.
Pressemeddelelse vedrørende koncert i Nordjysk Sangselskab søndag den 6. marts 2011. Søndag den 6. marts kl. 14, i hjertet af Aalborg Operafestival, inviterer Nordjysk Sangselskab til en koncert, hvor de store følelser er på spil. I brudfladen mellem romantik og senromantik maler komponisterne med store penselstrøg. I selskab med Schubert, Schumann, Strauss, Wolf og Berg skal vi møde
• Temperatur ↓ • Strahlung ↑ • Luftdruck ↓ LERTWARTEAUSBILDUNG FÜR KLETTERN-ALPIN • Sauerstoffteildruck ↓ • Luftdruck in Tallage (0 m) 760 mmHg (1013 hPa) Atemluft → Sauerstoffpartialdruck p O = 160 mmHg (213 hPa)• pro 100 Hm Abfall des Luftdrucks um ca. 1 %→ in ca. 5500 m p O = 80 mmHg (106 hPa) Normoxie • zusätzliche geographische und klimatisch
 Genetic tests as companion diagnostics 29
Figure 1. Necessary alliances to develop a successful companion diagnostic.
Genetic tests as companion diagnostics 29
Figure 1. Necessary alliances to develop a successful companion diagnostic.