He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Endoscopic.co.za
Crohn's Disease
Crohn's disease is a condition where there is inflammation in the gut. The
disease flares-up from time to time. Symptoms vary, depending on the part
of the gut affected. Medication can often ease symptoms when they flare-
up. Surgery to remove sections of the gut is needed to treat some flare-ups.
Medication taken each day may prevent symptoms from flaring-up. What is Crohn's disease?
Crohn's disease is a condition that causes inflammation of the wall of the gut. Any part of the gut
can be affected. This can lead to various symptoms (detailed below). Crohn's disease is named
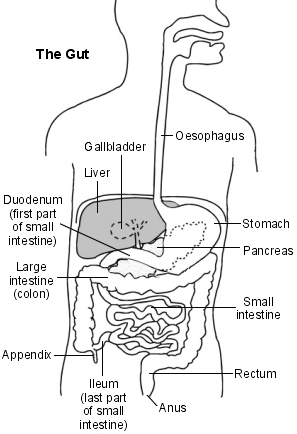
after Dr Crohn, the person who first described the disease in the 1930's. Understanding the gut
The gut (gastrointestinal tract) is the long tube that starts at the mouth and ends at the anus.
Food passes down the oesophagus (gullet), into the stomach, and then into the small
The small intestine has three sections - the
intestine is where food is digested and absorbed into the bloodstream. The structure
of the gut then changes to become the large
intestine (colon and rectum, sometimes called
The colon absorbs water, and contains food
that has not been digested, such as fibre. This is passed into the last part of the large
intestine, where it is stored as faeces. Faeces
(motions or stools) are then passed out of the
Who gets Crohn's disease?
About 1 in 1500 people have Crohn's disease.
It can develop at any age but most commonly
starts between the ages of 15 and 40. It affects
Which part of the gut is affected in Crohn's disease?
In Crohn's disease, one or more patches of inflammation develop in parts of the gut. Any part of the gut can be affected, but the most common site is the last part of the small intestine (the ileum).
The ileum is affected in about half of cases. Other parts of the small intestine and the colon are
also commonly affected. The mouth, gullet and stomach are affected much less commonly.
A patch of inflammation may be small, or spread quite a distance along part of the gut. Several
patches of inflammation may develop along the gut, with normal sections of gut in between. What causes Crohn's disease?
The cause is not known. Although not strictly an inherited disease, it tends to run in some families.
About 1 in 10 people with Crohn's disease have a close relative who also has it. This means there
may be some genetic factor. However, other factors such as a bacterium or virus (germ) may be involved. One theory is that a germ may trigger the immune system to cause inflammation in parts
of the gut in people who are genetically prone to develop the disease. Crohn's disease has
become more common in recent years, but the reason for this is not known. It is more common
than average in smokers and in women who use the combined oral contraceptive pill. How does Crohn's disease progress?
Crohn's disease is a chronic, relapsing condition. Chronic means that it is ongoing. Relapsing
means that there are times when symptoms flare-up (relapse), and times when there are few or no
symptoms (remission). The severity of symptoms, and how frequently they occur, varies from
person to person. The first episode (flare-up) of symptoms is often the worst. What are the symptoms of Crohn's disease?
Symptoms are due to inflammation in the wall of the affected parts of the gut. When the disease flares up, the inflammation may cause one or more of the following.
Pain. The site of the pain depends on which part of the gut is affected. The last part of the
small intestine (ileum) is the commonest site. Therefore, a common area of pain is the lower
right side of the abdomen. When Crohn's disease first develops it is sometimes mistaken for
appendicitis. The severity of pain can vary from person to person. Also, a sudden change or worsening of pain may indicate a complication (see below).
Ulcers. An ulcer is a raw area of the lining of the gut which may bleed. You may see blood
when you pass stools (motions or faeces).
Diarrhoea. This varies from mild to severe. The diarrhoea may be mixed with mucus, pus or
blood. An urgency to get to the toilet is common. A feeling of wanting to go to the toilet but
with nothing to pass is also common (tenesmus).
Generally feeling unwell with loss of appetite, weight loss, fever, and tiredness. Anaemia may occur if you lose a lot of blood. Mouth ulcers are common. Anal fissures may occur. These are painful 'cracks' in the skin of the anus. Skin tags (small
fleshy wart-like lumps) may also appear around the anus.
The symptoms can vary and depend on which part(s) of the gut are affected. For example:
you may not have diarrhoea if the disease is just in the small intestine. a persistent pain in the abdomen without any other symptoms may be due to a small patch
of Crohn's disease in the small intestine.
a severe flare-up can make you generally very ill. if large parts of the gut are affected, you may not absorb food well, and you may become
deficient in vitamins and other nutrients. Other symptoms
Other parts of the body are affected in some people in addition to the gut. These include:
inflammation and pain of some joints (arthritis); skin rashes; inflammation of the eye (uveitis); liver inflammation. These problems can cause various symptoms.
It is not clear why these other problems occur. The immune system may trigger inflammation in other parts of the body when there is inflammation in the gut. These other problems tend to go
when the gut symptoms settle, but not always. What are the possible complications of Crohn's disease?
Complications may occur, particularly if flare-ups are frequent or severe. These include the following which usually need treatment with surgery.
Stricture. This is a narrowing of part of the gut. It is due to scar tissue that may form in the
wall of an inflamed part of the gut. A stricture can cause difficulty in food passing through (a
'blockage'). This leads to pain and vomiting.
Perforation. This is a small hole that forms in the wall of the gut. The contents of the gut can
then leak out and cause infection or an abscess inside the abdomen. This can be serious
Fistula. This is when the inflammation causes a channel to form between two parts of the
gut. For example, a fistula may form between a part of the small intestine with part of the colon. Fistulas can also form between part of the gut and other organs, such as the bladder
or uterus (womb). The contents of the gut may then leak into these other organs.
Cancer. People with Crohn's disease have a small increased risk of developing cancer of
the intestines (bowel cancer) compared to the risk of the general population.
How is Crohn's disease diagnosed?
Depending on where the symptoms arise from, various tests may be done to confirm the
diagnosis, and determine how much of the gut is affected. For example, if you have symptoms
coming from the colon, then a doctor may look inside the colon using a special telescope (a short
sigmoidoscope or a longer flexible colonoscope. Separate leaflets describe these tests in detail). The typical appearance of the inside lining of the colon suggests Crohn's disease. Biopsies (small
samples) of the lining of the gut are usually taken. These are looked at under a microscope. The
typical pattern of the cells may confirm the diagnosis.
If you have symptoms coming from the upper part of the gut, then a doctor may suggest an
endoscopy. This is where a thin, flexible telescope is passed down the oesophagus into the
stomach. This allows a doctor or nurse to look inside.
A special X-ray of the large intestine (barium enema) or small intestine (barium meal) may be
advised. Barium coats the lining of the gut and shows up as white on X-ray films. Typical patterns on the films show which parts of the gut are affected.
More sophisticated tests and scans may be needed if the diagnosis is in doubt, or if complications are suspected. Also, blood tests are helpful from time to time to check for anaemia and other
What are the treatments for Crohn's disease? Treatment when symptoms flare-up
The common treatment to control symptoms when Crohn's disease first develops is either a steroid or a 5-aminosalicylate medicine. Both of these types of medicine reduce inflammation, but work in
different ways. They can be taken as tablets. They can also be taken as enemas if only the rectum
or last part of the colon is affected. Medication is taken for a few weeks until symptoms clear. A
course of medication is then usually taken each time symptoms flare-up.
A course of steroids (corticosteroids) such as prednisolone usually eases symptoms. In
about 7 in 10 cases, symptoms are much improved within four weeks of starting steroids. The dose is reduced gradually, and then stopped once symptoms ease. A course of steroids
for a few weeks is normally safe. Steroids are not usually continued once a flare-up has
settled. This is because side-effects may develop if steroids are taken for a long time (several months or more). The aim is to treat any flare-ups, but to keep the total amount of
steroid treatment over the years as low as possible.
5-sminosalicylate medicines include sulfasalazine, mesalazine, ofsalazine, and
balsalazide. They are an alternative to steroids, and often work well for mild or moderate
flare-ups. They do not work in all cases. Some people need to switch to steroid medication if
a 5-aminosalicylate medicine is not working, or if the flare-up is severe.
Other treatments. Some people do not respond well to steroid or 5-aminosalicylate
medication. Other treatments may then be considered.
Other 'second line' medicines may be advised. These include certain antibiotics,
immunosuppressive medicines such as methotrexate, and antibody therapy (infliximab). The success of these varies and a specialist may advise one or more to
find the best medicine or combination of medicines.
Dietary treatment. A very strict, special 'elemental' diet has been found to help in
some cases. A flare-up can settle within four weeks in about 2 in 3 cases. After this, a
normal diet is gradually re-started. It is not clear why this treatment works. It may have
some effect of 'resting' the gut. This may be an alternative for some people when
medication has not worked so well, or has caused bad side-effects.
Surgery to remove a severely affected section of gut may be needed if other
treatments do not work. The gut is cut above and below the affected part which is
removed. The two ends are then joined up. Surgery is also usually needed to treat
complications such as fistulas, strictures, and abscesses. Treatment between flare-ups
Once an initial episode of symptoms has cleared, you may be advised to take a medicine each day to prevent further episodes (flare-ups) of symptoms.
5-aminosalicylate medicines are used to prevent flare-ups of symptoms. A lower
'maintenance dose' than the dose used to treat a flare-up is usual. One can be taken
indefinitely. Most people have little trouble taking one of these medicines. Some people
develop side-effects such as abdominal pains, feeling sick, headaches, or rashes. If one medicine causes side-effects, switching to an alternative may be fine as side-effects can
Other medicines may be advised if a 5-aminosalicylate medicine does not work, or causes
difficult side-effects. For example, azathioprine or 6-mercaptopurine are alternatives, and some studies suggest that these may be better at preventing flare-ups than 5-
aminosalicylate medicines. Methotrexate is another alternative that is sometimes used.
However, medicines to prevent flare-ups do not work in all cases. Also, it may not be worthwhile
taking regular medication if flare-ups are not frequent, and respond well to treatment when they
occur. Your doctor will advise about the pros and cons of long-term medication. General measures
For smokers, stopping smoking reduces the number of flare-ups in some cases. Iron tablets may be prescribed if you develop anaemia. Vitamins and other nutrients may be needed if a large part of the gut is affected and food is
Anti-diarrhoeal medicines may be needed during flare-ups. Antibiotics are often needed during a flare-up. Painkillers may be needed for a while during flare-ups. Hospital admission for intravenous fluids (drip) and intensive treatment may be needed if
In some people a 'trigger' may possibly cause symptoms to flare-up. For example, milk products,
food preservatives, a reaction to certain medicines such as aspirin or other anti-inflammatory
medicines, or antibiotics. Some people find that avoiding triggers is beneficial. However, it is
difficult to prove whether such triggers are really to blame, and in most cases no change in diet or
lifestyle is advised. A well balanced healthy diet is usually best between flare-ups.
Newer medicines
Treatment for Crohn's disease is an evolving field. Various new medicines are under investigation and are likely to change the treatment strategies and options over the next ten years or so.
What is the outlook (prognosis)?
The outlook is variable. It depends on which part(s) of the gut are affected, and how often and how severe the flare-ups are.
About 3 in 20 people with Crohn's disease have frequent and/or severe flare-ups. A few people with Crohn's disease have just one or two flare-ups in their life, but for most of their life have no
symptoms. Most people with Crohn's disease fall somewhere in between, have flare-ups from time
to time, but can have long spells without symptoms. Sometimes a severe flare-up is life-threatening and some people die as a result of a serious complication such as a perforated gut.
About 8 in 10 people with Crohn's disease require surgery at some stage in their life for a
complication. In about half of people with Crohn's disease, surgery is needed within the first 10 years of developing the disease. The most common reason for surgery is to relieve a stricture that
has formed. Some people need several operations in their lifetime. If you develop Crohn's disease
as a young adult, on average you can expect to have 2-4 operations in your lifetime. However, you can usually expect a good quality of life for most of the time.
What is inflammatory bowel disease?
When doctors talk of 'inflammatory bowel disease' they usually mean people who either have
Crohn's disease or ulcerative colitis. Both of these conditions can cause inflammation of the colon
and rectum (large bowel or large intestine) with similar symptoms such as bloody diarrhoea, etc. Although these conditions are similar, and treatments are similar, there are differences. For
example, the inflammation of ulcerative colitis tends to be just in the inner lining of the gut,
whereas the inflammation of Crohn's disease can spread through the whole wall of the gut. Also,
ulcerative colitis only affects the colon and rectum whereas Crohn's disease can affect any part of the gut. There is a separate leaflet that gives more detail about ulcerative colitis.
However, about 1 in 20 patients with 'inflammatory bowel disease' affecting the colon cannot be classified as either Crohn's disease or ulcerative colitis because they have some features of both
conditions. This is sometimes called indeterminate colitis. Further information NACC - National Association for Colitis and Crohn's Disease
4 Beaumont House, Sutton Road, St Albans, Herts, AL1 5HHTel: 0845 130 2233 Web: www.nacc.org.uk
Crohn's in Childhood Research Association
Parkgate House, 356 West Barnes Lane, Motspur Park, Surrey KT3 6NBTel: 020 8949 6209 Web: www.cicra.org
EMIS and PIP 2005 Updated: November 2005
Comprehensive patient resources are available at www.patient.co.uk
Marc GIRARD Mathématicien de formation, le Dr Girard est devenu médecin tout en menant des recherches sur la modélisation mathématique en biologie. Après un passage aussi bref que mouvementé comme salarié d’une grande firme pharmaceutique, il a développé, en France, la première activité libérale de conseil en pharmacovigilance (étude des effets secondaires des médicaments) et e
Contemporary legal institutions TRADE RELATED ASPECTS OF INTELLECTUAL PROPERTY RIGHTS, ISSUES FOR DEVELOPING Professor CHARLES F. HICKMAN University of Alabama in Huntsville The Trade Related Aspects of Intellectual Property Rights (TRIPS) agreement was adopted as Annex 1C of the Agreement Establishing the World Trade Organization in 1994. The adoption of TRIPS was large
 Crohn's Disease
Crohn's Disease