He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Dr-mardani.ir
ORIGINAL ARTICLE
Acta Orthop Traumatol Turc 2012;46(5):346-352
Efficacy of sonographically guided intra-flexoral sheath corticosteroid injection in the treatment of trigger thumb Mohsen MARDANI-KIVI1, Farivar Abdullahzadeh LAHIJI2, Ali Babaei JANDAGHI3, Khashayar SAHEB-EKHTIARI4, Keyvan HASHEMI-MOTLAGH4 1Department of Orthopedics, Guilan University of Medical Sciences, Rasht, Iran;2Department of Orthopedics, Shahid Beheshti University of Medical Sciences, Tehran, Iran;3Department of Radiology, Guilan University of Medical Sciences, Rasht, Iran;4Orthopedics Research Center, Guilan University of Medical Sciences, Rasht, IranObjective: The aim of this study was to determine the efficacy of sonographically guided intra-flexo- ral sheath corticosteroid injection in the treatment of trigger thumb. Methods: This study included 112 trigger thumbs of 104 patients (7 males, 97 females; mean age: 52.11 years) studied prospectively from 2009 to 2011. All patients experienced pain, tenderness, dis- comfort and/or triggering with flexion/extension of the thumb and palpable nodules at the level of the A1 pulley. Ultrasonographically guided corticosteroid injection was performed on all affected thumbs. Thumb improvement was evaluated using the Quinnell grading system and patients were followed up for one year. Results: All 112 thumbs received one ultrasonographically guided corticosteroid injection. Fifteen thumbs (13.4%) needed re-injection and/or surgery during their one year follow-up. Eight (53.3%) of these 15 cases, had a pre-treatment Quinnell Grade of 4, six (40%) thumbs were Grade 3 and one (6.7%) was Grade 2. Twelve were re-injected, two underwent surgery without re-injection and one underwent surgery after showing no improvement following re-injection. There was a significant reduction in the post-injection Quinnell grade (p<0.0001). One year after the initial injection, 108 thumbs (96.4%) were completely symptom-free. Conclusion: Sonographically guided intra-flexoral sheath corticosteroid injection is an effective method in the treatment of trigger thumb and reduces the need for surgery. Key words: Corticosteroid injection; tenosynovitis; therapeutic; trigger thumb; ultrasound.
Trigger finger/thumb is one of the most prevalent
rigidity, a click, difficulty in opening the flexed finger
causes of hand disability and is a common cause of
and pain caused by inflammation and progressive
referral to orthopedic clinics.[1-3] It is more common
hypertrophy of the finger or thumb flexor tendon
among women,[1,3-6] with the thumb having the highest
sheath at the level of the A1 pulley.[8-13] The first line of
involvement.[1,6,7] Symptoms include snapping, locking,
treatment are conservative methods, such as finger
Correspondence: Mohsen Mardani-Kivi, MD. Guilan University of Medical Sciences, Namjoo Avenue, Rasht, Iran, PO Box: 4193713191.
Tel: +98-131 - 323 98 42 e-mail: [email protected]Submitted: December 3, 2011 Accepted: April 4, 2012 2012 Turkish Association of Orthopaedics and Traumatology
Mardani-Kivi et al. Efficacy of ultrasound-guided intra-flexoral sheath corticosteroid injection in trigger thumb
rests with or without the use of a splint and a local cor-
ease, carpal tunnel syndrome and Dupuytren’s con-
ticosteroid injection.[1,14-16] Surgical treatments are inva-
tracture, involvement of other fingers, clinical doubt as
sive and have potential complications. Although good
to the true nature of the symptoms or any history of
results with surgical treatment are possible in children
local corticosteroid injection were excluded.
over one year of age,[17] surgery is only indicated if non-
Additionally, patients undergoing ultrasound-guided
surgical treatments fails in adults.[7,14,18]
intra-flexoral sheath injection treatment in the first
Intra-flexoral corticosteroid injection is the most
three months were excluded. One hundred and twelve
common non-surgical treatment with a reported suc-
thumbs of 104 patients (7 men, 97 women; mean age:
cess rate between 38 and 93% for the treatment of trig-
52.11±7.63 years; range: 26 to 69 years) were included
ger thumb.[1,6,19,20] Recently, studies have questioned the
accuracy and precision of intra-sheath blind corticos-
The affected side was right in 64 patients, left in 32
teroid injection and its effect on the treatment success
and bilateral in 8. Trigger thumb was seen in the dom-
rate.[1] A recent study explored the intra-sheath delivery
inant hand in 89 of 112 thumbs (79.5%) and in the
of corticosteroids using a blind injection of methylene
non-dominant hand in 23 (20.5%). Patients were grad-
blue and corticosteroid into the sheath before open
ed according to Quinnell’s grading classification
surgery in the treatment of trigger thumb. They
(Table 1). Of the 104 patients, 28 (26.9%) had con-
observed that the contrast medium was successfully
comitant medical conditions (Table 2). Symptoms
injected into the flexoral sheath in only half of the
were present for less than six months (<6 months
blind injections and was clinically manifested as an
group) in 107 thumbs (95.5%) and more than 6
increase in the duration of symptoms in this sub-group
months (>6 month group) in 5 thumbs (4.5%).
of patients.[21] In addition, reports have been issuedabout hazardous consequences of blind injection ofcorticosteroids.[22,23] Lee et al. performed a study com-
paring 20 ultrasound-guided injections and 20 blindinjections and reported successful intra-sheath injec-
Grade Explanation
tion in 70% of the group with ultrasound-guided injec-
Without trigger state, uneven finger movement or slight
tions and only in 15% in the group receiving blind
injections.[24] Therefore, the aim of this study was to
Trigger state, finger snapping that is corrected actively
study the therapeutic outcomes and complications of
Trigger state, finger snapping that is corrected passively
ultrasound-guided intra-flexoral sheath injection.
Patients and methods This descriptive, prospective study reviewed all
Previous studies have showed increased success rates
patients referred to our orthopedic clinic for trigger
with the insertion of a 25-gauge needle in a proximal to
thumb between March 2009 and March 2011.
distal direction at an angle of 30-45° angle from the volar
Inclusion criteria were pain and tenderness at the posi-
side into the anatomic position of the A1 pulley.[4,21,25] We
tion of A1 pulley, pain and discomfort when flexing
performed the same procedure using 1 ml of 40 mg/ml
and extending the finger, nodule palpation, presence of
methyl prednisolone acetate and 0.5 ml of 2% lidocaine
a clicking sound at the time of flexion or extension of
hydrochloride in all patients. All examinations, diagno-
the thumb, snapping or locking of finger, and the exis-
sis, injections, investigation of therapeutic outcomes and
tence of a trigger state. Patients with any kind of con-
re-injections or operations, if needed, were performed
comitant local tenosynovitis such as De Quervain’s dis-
by the corresponding author. Ultrasound guidance was
The frequency of concomitant medical conditions in the population of the patients of this study. Frequency in persons synchronous Number of having concomitant Frequency in patients* medical conditions all patients
*One patient was simultaneously afflicted with diabetes mellitus and rheumatoid arthritis and one patient had diabetes mellitus andhypothyroid simultaneously.
Setting the probe to find the tendon in axial view. [Color
Rotating the probe to find the tendon in longitudinal view.
figure can be viewed in the online issue, which is available
[Color figure can be viewed in the online issue, which is
performed using a 14 MHz linear probe (Ultrasonix,
needle was inserted into the space between the A1 pul-
Touch model, ver. 5.5.4). First, the tendon was detect-
ley and flexor pollicis longus at a 30 to 45° angle ori-
ed through an axial scan of the proximal phalanx (Fig.
ented proximal to distal and the solution injected (Fig.
2) and the probe was rotated until a fibrillary echo pat-
4). Distension of the tendon sheath and the resultant
tern was visualized and adjusted in the screen center.
fluid wave inside from the finger tip to the injection
Next, the probe was moved proximally to the first MCP
site were confirmed during the injection process (Figs.
joint and the first annular pulley appeared (Fig. 3). The
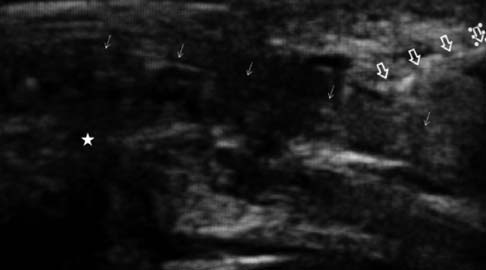
Inserting the needle at 30-45° angle.
Longitudinal view of needle's entrance (Hollow arrows:
[Color figure can be viewed in the online issue, which is
needle, solid arrows: tendon, star: the first metacarpopha-
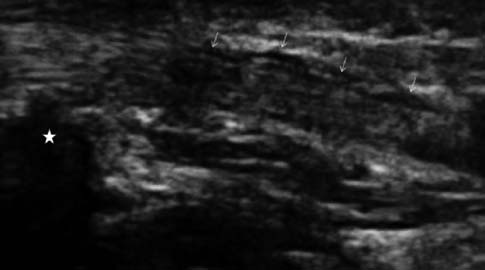
Longitudinal view of tendon after corticosteroid injection
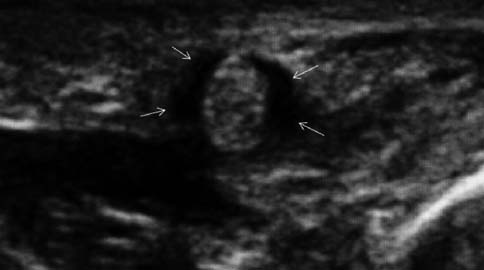
Axial view of the tendon after corticosteroid injection
(Arrows: confluence of liquid inside sheath around tendon,
(Arrows: fluid collection inside sheath around tendon).
star: the first metacarpophalangeal joint).
Mardani-Kivi et al. Efficacy of ultrasound-guided intra-flexoral sheath corticosteroid injection in trigger thumb
Frequency
Patients were followed-up at 3 and 6 weeks, 3 and 6
ences of qualitative parameters between groups. To
months and 1 year after the first injection. Of the orig-
analyze the trend of Quinnell’s grade changes, repeat-
inal 117 patients, 13 were excluded from the study
ed measure analysis test through Mauchley’s test of
because of failed follow-up. The Quinnell’s criterion
sphericity was employed, and to evaluate the value of
was applied to evaluate improvements during follow-
these changes, analysis of variance (ANOVA) was per-
up. Patients were observed for 6 weeks and further
formed. In all statistical tests, the p value was set at
treatment (re-injection or surgery) was suggested to
patients and performed depending on patient prefer-ence. In addition, patients who were still symptomatic
after 2 injections became candidates for open surgery.
Symptoms were completely ameliorated after one
Collected data was saved separately into two thera-
injection in 86.6% of thumbs. These patients had no
peutic groups and was statistically analyzed using SPSS
relapse. At the one year follow-up, 15 thumbs (13.4%)
software package for Windows v.19.0 (SPSS Inc.,
needed reinjection and/or surgery. Of these 15
Chicago, IL, USA). After summarizing the characteris-
thumbs, 12 (80%) were re-injected, 2 (13.3%) under-
tics of both groups with descriptive statistics, response
went surgery without re-injection, and one (6.7%) was
variables were evaluated according to the
re-injected and underwent subsequent surgery. No
Kolmogorov-Smirnov test and it was shown that none
thumb was injected more than two times. Of the 13
had a normal distribution. The Mann-Whitney U test
reinjection cases, only one case (7.7%) needed surgery.
was used in order to compare these variables of both
After one year (6th visit), 109 thumbs (97.3%) were
groups and the chi-squared test to compare the differ-
symptom-free and only one thumb was at Quinnell’s
Frequency distribution and the mean of Quinnell's grade of fingers in performed visits. Mean±SD Turn of visit Number (%) Number (%) Number (%) Number (%) Number (%) Quinnell’s grade (Mean) Quinnell’s grade (Mean)
Quinnell's grade in two groups of less and more than 6months.
Grade 1. Due to this patient’s unwillingness, reinjec-
of sonographic guidance. The inaccuracy associated
with blind injection appears to be responsible for the
Quinnell’s grading for thumbs from the first to
decrease in success rates seen in intra-sheath delivery
sixth visits is shown in Table 3. Statistical analysis
revealed that the trend and value of variations of
The relationship between the existence of one or
Quinnell’s grade are statistically significant for all
more concomitant medical conditions and the efficacy
thumbs (p<0.0001) (Fig. 8). In addition, trend and
of corticosteroid injection has also been scruti-
value of variations of Quinnell’s grade was statistically
nized.[6,14,19,27-29] Many authors, including Blythe and Ross,
significant between the over and under 6 month symp-
regarded trigger thumb as a part of what they called
tom groups (p<0.0001) (Fig. 9). There was no signifi-
“diabetic hand syndrome”.[28] Since there were a limited
cant difference in trend and value of variations of the
number of patients with both hypothyroidism (6.7%)
Quinnell’s grade between diabetic and non-diabetic
and rheumatoid arthritis (2.9%) in this study, we chose
patients (p=0.85 and p=0.63, respectively). Quinnell’sgrades of these two groups are given in Fig. 10. Complications were not seen in any patient.
Discussion
The effect of corticosteroid injections in the treatmentof stenosing tenosynovitis is a contentious issue in
orthopedics. Despite studies for more than a quartercentury, the role of corticosteroid injections into the
flexor tendon’s sheath and the importance of intra-sheath delivery in the treatment of trigger finger and
thumb has been questioned.[1,19,21,26] In the present study,
Quinnell’s grade (Mean)
109 of 112 thumbs (97.3%) were completely symptom-
free one year post-injection. This rate is higher than
the reported success rates of 38 to 93% in previousstudies.[1,16,19,20] Those studies with a varying range of
success rates relied on blind injection for the corticos-
teroid delivery, while those with higher success rates,
Fig. 10. Quinnell's grade in two groups of diabetic and non-diabet-
including the present study, were attained with the aid
Mardani-Kivi et al. Efficacy of ultrasound-guided intra-flexoral sheath corticosteroid injection in trigger thumb
to discuss diabetic patients, as it is very common in our
3. Flatt AE. Notta’s nodules and trigger digits. Proc (Bayl Univ
patient population. In several previous studies,[2,19,29] dia-
betic patients showed less therapeutic response than
4. Creighton JJ Jr, Idler RS, Strickland JW. Trigger finger and
non-diabetic individuals and required surgical treatment
5. Ger E, Kupcha P, Ger D. The management of trigger
more often. In a study of 54 diabetic patients with 121
thumb in children. J Hand Surg Am 1991;16:944-7.
trigger thumbs over a 3 year follow-up, Griggs et al.[27]
6. Moore JS. Flexor tendon entrapment of the digits (trigger
reported that symptoms were completely ameliorated in
finger and trigger thumb). J Occup Environ Med 2000;42:
34 fingers (28%) after the first injection, and this num-
ber increased by an additional 27 fingers (22%) after the
7. Lange-Riess D, Schuh R, Hönle W, Schuh A. Long-term
second and third injections. Sixty fingers (50%)
results of surgical release of trigger finger and trigger thumb
improved slightly and required surgery to release the A1
in adults. Arch Orthop Trauma Surg 2009;129:1617-9.
pulley. In the present study, although a higher percent-
8. Newport ML, Lane LB, Stuchin SA. Treatment of trigger
age of diabetic thumbs opposed to non-diabetic thumbs
finger by steroid injection. J Hand Surg Am 1990;15:748-50.
(30.8% and 18.2%, respectively) required reinjection,
9. Sampson SP, Badalamente MA, Hurst LC, Seidman J.
Pathobiology of the human A1 pulley in trigger finger. J Hand
this difference was not statistically significant (p=0.28).
This indicates that diabetic patients benefit from ultra-
10. Doyle JR. Anatomy of the finger flexor tendon sheath and
sound-guided intra-flexoral injection as much as non-
pulley system: a current review. J Hand Surg Am 1989;14:
Limitations of sonographically guided intra-flexo-
11. Hume EL, Hutchinson DT, Jaeger SA, Hunter JM.
ral injection are the limited availability of sonography
Biomechanics of pulley reconstruction. J Hand Surg Am1991;16:722-30.
and the need for skillful radiologists for ultrasound
12. Moutet F. Flexor tendon pulley system: anatomy, pathology,
guidance, which cause significantly more costs com-
treatment. [Article in French] Chir Main 2003;22:1-12.
pared to the blind method. However, the reduction in
13. Bayat A, Shaaban H, Giakas G, Lees VC. The pulley system
the need for surgery and the remarkable increase in the
of the thumb: anatomic and biomechanical study. J Hand
speed and rate of symptom amelioration results in a
reduction in health care costs and the financial burden
14. Makkouk AH, Oetgen ME, Swigart CR, Dodds SD. Trigger
finger: etiology, evaluation, and treatment. Curr Rev Muscu-
This study was conducted on the thumb only. With
15. Colbourn J, Heath N, Manary S, Pacifico D. Effectiveness of
the exception of a limited number of case studies,[2]
splinting for the treatment of trigger finger. J Hand Ther
most studies have been conducted on trigger fingers
(thumbs and fingers) and the fact that this study is lim-
16. Maneerit J, Sriworakun C, Budhraja N, Nagavajara PN.
ited to the thumb makes it difficult to compare and
Trigger thumb: results of a prospective randomised study of
generalize its results to other fingers. On the other
percutaneous release with steroid injection versus steroid
hand, the present study included a large sample volume
injection alone. J Hand Surg Br 2003;28:586-9.
of thumbs that is rare. Further studies that consider the
17. Sevencan A, Inan U, Köse N, Omero¤lu H, Seber S.
efficacy of the same method in other fingers with a
Percutaneous release for trigger thumb in children: improve-ments of the technique and results of 31 thumbs. J Pediatr
larger volume of samples are recommended.
In conclusion, sonographically guided corticos-
18. Cebesoy O, Kose KC, Baltaci ET, Isik M. Percutaneous
teroid injection into the sheath of the flexor tendon of
release of the trigger thumb: is it safe, cheap and effective?
the thumb appears to be a highly useful in the treat-
ment of trigger thumb and decreases the need for sur-
19. Nimigan AS, Ross DC, Gan BS. Steroid injections in the
gery, especially in patients who with a symptom dura-
management of trigger fingers. Am J Phys Med Rehabil
20. Lambert M, Morton RJ, Sloan JP. Controlled study of the
Conflicts of Interest: No conflicts declared.
use of local steroid injection in the treatment of trigger fin-ger and thumb. J Hand Surg Br 1992;17:69-70. References
21. Kamhin M, Engel J, Heim M. The fate of injected trigger
1. Akhtar S, Bradley MJ, Quinton DN, Burke FD. Management
and referral for trigger finger/thumb. BMJ 2005;331:30-3.
22. Fitzgerald BT, Hofmeister EP, Fan RA, Thompson MA.
2. Howitt S, Wong J, Zabukovec S. The conservative treatment
Delayed flexor digitorum superficialis and profundus rup-
of Trigger Thumb using Graston Techniques and Active
tures in a trigger finger after a steroid injection: a case
Release Techniques. J Can Chiropr Assoc 2006;50:249-54.
report. J Hand Surg Am 2005;30:479-82.
23. Park J, Dumanian GA. Shower emboli and digital necrosis
26. Taras JS, Raphael JS, Pan WT, Movagharnia F, Sotereanos
after a single corticosteroid injection for trigger thumb: case
DG. Corticosteroid injections for trigger digits: is intrasheath
report. J Hand Surg Am 2009;34:313-6.
injection necessary? J Hand Surg Am 1998;23:717-22.
24. Lee DH, Han SB, Park JW, Lee SH, Kim KW, Jeong WK.
27. Griggs SM, Weiss AP, Lane LB, Schwenker C, Akelman E,
Sonographically guided tendon sheath injections are more
Sachar K. Treatment of trigger finger in patients with dia-
accurate than blind injections: implications for trigger finger
betes mellitus. J Hand Surg Am 1995;20:787-9.
treatment. J Ultrasound Med 2011;30:197-203.
28. Blythe MJ, Ross DJ. Diabetes and trigger finger. J Hand
25. Zare-zadeh A, Samavarchi Tehrani M, Noorian V, Padidar
B. Efficacy of local corticosteroid injection in trigger finger
29. Arkkila PE, Gautier JF. Musculoskeletal disorders in dia-
treatment. [Article in Persian] Journal of Arak University of
betes mellitus: an update. Best Pract Res Clin Rheumatol
REGLAMENTO DE INSCRIPCIONES DEL REGISTRO DE PREDIOS SECCIÓN I DISPOSICIONES GENERALES Artículo 1°.- Contenido del Reglamento El presente Reglamento regula los requisitos para la inscripción de los diferentes actos o derechos en el Registro de Predios, las formalidades de los documentos que dan mérito a las inscripciones, el contenido de los asientos registrales y los proc
Sulla strada – Rassegna stampa 06 luglio 2011 PRIMO PIANO Incidenti stradali: UE, meno morti nel 2010, -6% in Italia 05.07.2011 - Scende il numero degli incidenti stradali mortali in Europa: nel 2010, secondo gli ultimi dati pubblicati oggi dalla Commissione Ue, la riduzione complessiva e' stata dell'11% ma l'andamento varia molto da Stato a Stato. In particolare, il rapporto fra mort

 ORIGINAL ARTICLE
ORIGINAL ARTICLE


 Setting the probe to find the tendon in axial view. [Color
Rotating the probe to find the tendon in longitudinal view.
Setting the probe to find the tendon in axial view. [Color
Rotating the probe to find the tendon in longitudinal view.