He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Doi:10.1016/s0006-3223(02)01787-0
Comorbidity is common among patients with major de-Medical Comorbidity pression, but in most instances it may be of little rele-vance. Nonetheless, it is a complex issue because of its
Clinical trials of antidepressants generally exclude patients
relation to treatment response, and few studies have
who have significant medical illness, yet depression with
attempted to address this. Most have examined comorbid-
medical comorbidity is the norm rather than the exception
ity after the fact in secondary analyses. In this article, I
among patients who are seen in most clinical settings. The
focus on whether comorbidity influences depression treat-
treatment of depression in medically ill patients is chal-
ment response among patients who are primarily diag-
lenging. Recognition, compliance, differential diagnosis,
nosed as suffering from major depression. At least three
side effects, and tolerance of drug regimens can compli-
comorbidities are believed to influence treatment re-
cate the treatment of depression among patients who are
sponse: medical, anxiety, and personality disorders.
medically ill. Before the introduction of selective seroto-
Whether studies find that these factors predict worseoutcomes in patients with major depression appears to
nin reuptake inhibitors (SSRIs), it was generally believed
depend on the nature and severity of the medical illness,
that medically ill depressed patients did not tolerate or
the study setting, and the study design. The best designed
respond well to antidepressant treatment.
studies reported the least effects of these factors on
reported that nortriptyline was contraindicated in
treatment outcome. Clinically, this suggests that these
90% of medically ill depressed patients. He also noted that
factors should not be seen as impediments to treatment.
80% of potentially eligible patients were unable to com-
Biol Psychiatry 2003;53:701–706 2003 Society of Bio-
plete a trial of nortriptyline. In a retrospective review
reported that only 40% of medically illdepressed patients responded to treatment and that 32%
Key Words: Comorbidity, medical, treatment, anxiety,
could not tolerate treatment. Both these studies were
conducted before the advent of SSRIs and led to anihilistic perception regarding the use of antidepressants in
Introduction
the medically ill. This perception may not be warranted.
A recent Cochrane report on the use of antidepressants
Comorbidity is common among patients with major in the medically ill addresses the issue of whether antide-
depression, but in most instances it may be of little
pressants are effective in this population
relevance. Nonetheless, it is a complex issue because of its
This review analyzed all relevant randomized trials
relation to treatment response, and few studies have
that compared any antidepressant drug with placebo or no
attempted to address this. Most available studies examined
treatment in patients diagnosed with depression and a
comorbidity after the fact in secondary analyses. In this
specified physical disorder. This review included 18 stud-
article, I focus on whether comorbidity influences depres-
ies, covering 838 patients with a range of medical condi-
sion treatment response among patients who are diagnosed
tions (cancer in two studies, diabetes in one, head injury in
primarily as suffering from major depression. It is impor-
one, heart disease in one, HIV in five, lung disease in one,
tant to keep in mind that depression secondary to other
multiple sclerosis in one, renal disease in one, stroke in
diseases may not have the same response pattern. At least
three, combined disorders in two). Six studies used SSRIs,
three comorbidities are believed to influence treatment
three used atypical antidepressants, and the reminder used
response: medical, anxiety, and personality disorders. I
tricyclic antidepressants (TCA). The key finding was that
briefly review the available information on whether the
patients treated with antidepressants were more likely to
presence of these three categories of comorbidity influ-
improve than those who were given placebo or no treat-
ence treatment response among patients with a primary
ment. The finding that about four patients would need to
be treated with antidepressants to produce one recoveryfrom depression that would not have occurred had they
From the Department of Psychiatry and Behavioral Sciences, Duke University
been given placebo or no treatment is similar to that seen
Medical Center, Durham, North Carolina.
Address reprint requests to Ranga R. Krishnan, M.D., Department of Psychiatry and
in trials of depressed patients without medical problems.
Behavioral Sciences, Duke University Medical Center, Box 3950, Durham NC
The other interesting finding was that antidepressants were
Received May 3, 2002; revised August 26, 2002; accepted October 2, 2002.
well tolerated by patients; about 10 patients would need to
be treated with antidepressants to produce one dropoutfrom treatment, which would not have occurred had theybeen given placebo. By inferencefrom this review, one can conclude that medical comor-bidity is not a major factor in treatment response.
is that they did not include both healthyand medically ill patients with depression. Thus, it cannotbe definitively stated that, under the same trial conditions,medical comorbidity does not influence treatment re-sponse. Steffens recently studied this issue in a naturalisticmanner Thirty-one elderly patientswith unipolar major depression (DSM-IV) who wereenrolled in Duke’s Mental Health Clinical Research Cen-
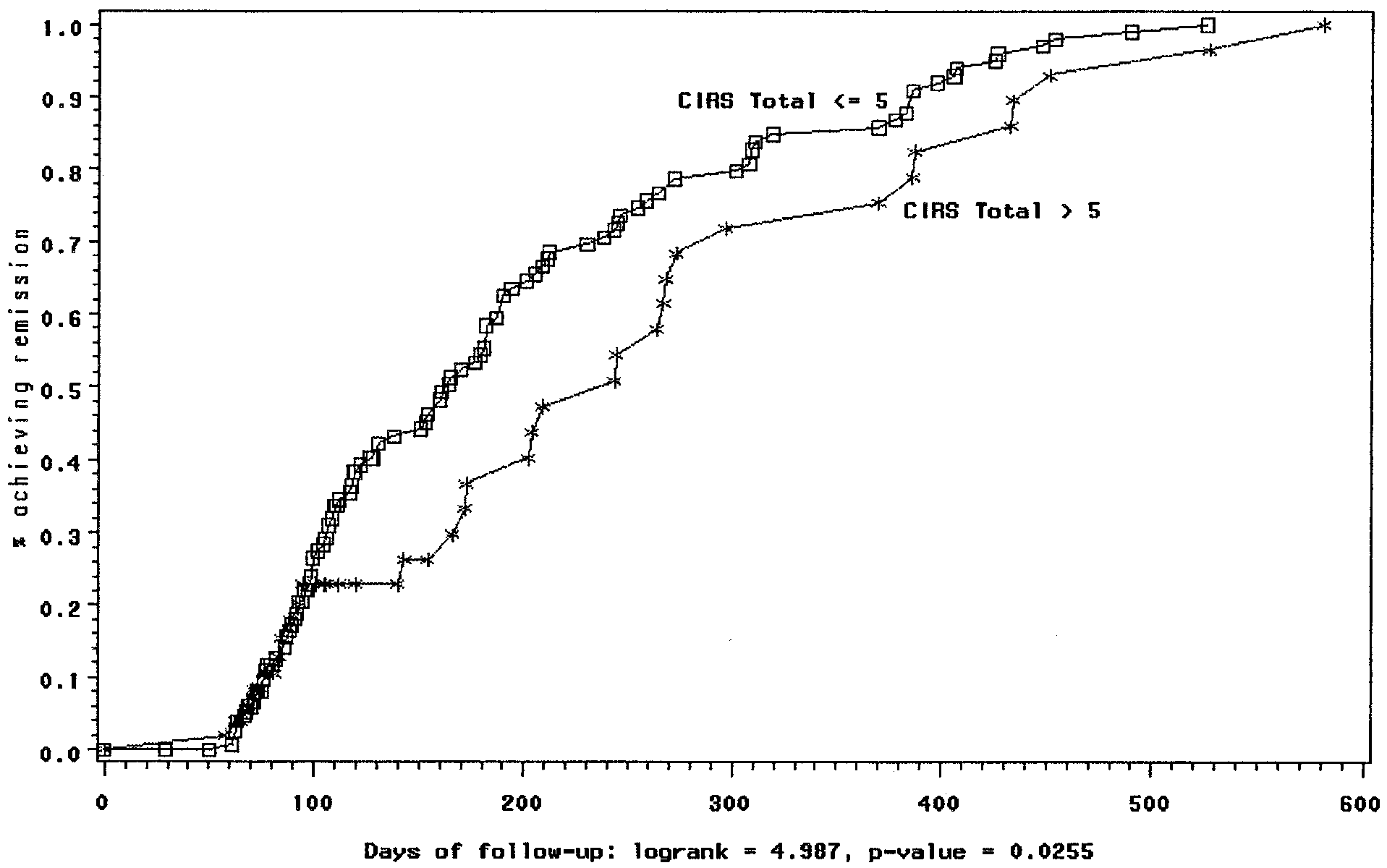
Figure 1. Cumulative remission for depressed patients starting
ter for the Study of Depression in Later Life were
prescribed bupropion SR or IR, alone or in combinationwith other antidepressant agents, for 12 weeks. Montgom-
disease and other forms of dementia, stroke, Parkinson’s
ery–Asberg Depression Rating Scale (MADRS;
disease, and multiple sclerosis); subjects with current or
recent histories of substance abuse were also excluded. At
Impression (CGI) severity scores were used to define
baseline, subjects received standardized clinical assess-
response. Seventy-four percent of the sample responded to
ments including the MADRS and Cumulative Illness
treatment. Fifty-three percent (16 of 30) achieved a partial
or complete remission of major depression at week 12.
viewer administered the Duke Depression Evaluation
Response rates did not differ between those with high
concluded that geriatric patients with high and low med-
instrument that includes the Centers for Epidemiologic
ical comorbidity responded well to bupropion and bupro-
portions of the National Institute of Mental Health Diag-
We recently evaluated the effect of sertraline in patients
nostic Interview Schedule (DIS). The interview consists of
with major depression and comorbid vascular disease
questions that screen for DSM-IV diagnoses including
major depression, bipolar disorder, generalized anxiety
three groups: 1) patients with a current diagnosis of
disorder, and panic disorder. Clinical assessments were
hypertension only, 2) patients with a current or past history
repeated every 3 months and when contact was clinically
of cardiovascular illness but no hypertension, and 3)
patients with no hypertension or comorbid vascular illness.
Subjects in the study were treated as clinically indi-
Sertraline treatment yielded similar levels of response in
cated, using antidepressant medications, electroconvulsive
all three groups (response criterion: CGI much or very
therapy (ECT), and individual and group cognitive– be-
much improved) at treatment end point on a completer
analysis (hypertension: 86%; vascular disease: 89%; no
vascular disease: 77%). Both our study and that of
The results of the study demonstrated that the cumula-
tive remission rate was slightly greater among patients
however, and the medical comorbidity evaluated was
without medical illness than among those with mild
restricted to vascular disease in our study. We therefore
medical illness (CIRS Ͼ 5; see Remission was
evaluated the role of medical factors in a large sample of
defined as MADRS score less than 8; when adjusted for
elderly patients who were treated using a staged approach.
age, however, this variable was not significant. In sum-
The sample consisted of 259 subjects enrolled in the
mary, the results of these three studies, in consonant to the
National Institute of Mental Health–sponsored Mental
Health Clinical Research Center for the Study of Depres-
medical comorbidity has only a modest and insignificant
sion in Later Life (Conte Center). The subjects were Ն 60
effect on antidepressant treatment response; however, this
years and met DSM-IV criteria for major depression at
may not be the case for other medical conditions and needs
baseline. Exclusions included other major psychiatric
to be further evaluated. Whether studies find that medical
illness (e.g., schizophrenia, schizoaffective disorder, bipo-
disorders predict worse outcome in patients with major
lar disorder) or major neurologic illness (e.g., Alzheimer’s
depression appears to depend on the nature and severity of
the medical illness, the study setting, and the study design.
described earlier, no difference in treatment response was
The best designed studies reported the least effect of
found among paroxetine, sertraline, and fluoxetine
medical illness on depression treatment outcome. Clini-
cally, this suggests that medical illness should not be seen
venlafaxine in patients with anxiety and depression. A
pooled analysis was conducted of six short-term trials ofvenlafaxine measuring anxiety in anxious-depressed pa-tients using the HAM-D, anxiety/somatization factor and
Anxiety Disorder
psychic anxiety item scores. Treatment with venlafaxine
Anxiety disorder is also common among patients with
resulted in a significant improvement in depression scores
in patients who were anxious at baseline compared with
quency of diagnostic comorbidity in major depressive
disorder (MDD). At the time of the evaluation, 64.1% of
Data from eight randomized, double-blind, placebo-
the patients met criteria for at least 1 of the 23 Axis I
controlled clinical trials comparing mirtazapine to placebo
disorders, and more than one third had two or more
in patients with high anxiety and depression were reported
disorders. Anxiety disorders were the most frequent co-
morbid disorders (56.8%), and social phobia was the most
demonstrated a statistically significant reduction in the
frequent individual disorder. Among depressed patients,
sum of anxiety and agitation compared with placebo-
the more severe the depression, the more likely the
treated patients. In general, the drug was effective in
presence of anxiety symptoms. It is assumed that anxiety
treating both anxiety and depression, and anxiety did not
symptoms affect treatment response. This has been eval-
uated in a number of studies. reported that
All these studies primarily classified patients on the
people with depression who were anxious responded
basis of the anxiety subscale of the HAM-D. They did not
poorly to amitriptyline compared with other depressed
specifically address the issue of whether the anxiety was
patients. Another study reported that neurotic symptoms
part of depression or as part of another anxiety disorder. In
general, these studies would have excluded patients with
The data with regard to the SSRIs appears to be
primary anxiety disorders. The data are modest in terms of
whether the presence of an anxiety disorder can influence
randomized, double-blind clinical trials comparing fluox-
etine with placebo or TCAs in patients with major depres-
response in patients with major depression and comorbid
sion. On the basis of the anxiety/somatization factor within
anxiety disorder who were treated with fluvoxamine. The
the 21-item Hamilton Rating Scale for Depression (HAM-
mean number of comorbid anxiety disorders per patient
D), patients were characterized as anxious (score Ն 7) or
was 2.1 Ϯ 1.1. Fluvoxamine was shown to be effective in
nonanxious (score Ͻ 7). Fluoxetine was significantly (p Յ
treating outpatients with major depression with comorbid
.05) more effective than placebo in treating both anxious
anxiety disorder. This study was limited by the small
and nonanxious major depression. Fluoxetine was also
number of subjects and by the fact that a number of studies
more effective than placebo in reducing the anxiety/
have not shown a clear antidepressant effect for fluvox-
The effect of anxiety on treatment response to sertraline
efficacy of venalfaxine on patients with concomitant
was evaluated in a study of chronic depression
generalized anxiety disorder and depression. Ninety-two
In this study, patients diagnosed with chronic
patients meeting DSM-IV criteria for MDD who also had
major or double depression were randomized to 12 weeks
comorbid generalized anxiety disorder were compared
of double-blind treatment with either sertraline or imipra-
with 276 noncomorbid patients. Patients received ven-
mine in a 2:1 ratio. A high-anxiety subgroup was opera-
lafaxine XR (75–225 mg/day), fluoxetine (20 – 60 mg/
tionally defined by a HAM-D anxiety/somatization factor
day), or placebo for 12 weeks. Onset of efficacy was
score Ն 7. Of the total sample, 209 were treated with
slower in comorbid than in noncomorbid patients. Re-
imipramine and 426 with sertraline. Thirty-six percent of
sponse, defined as Ͼ 50% decrease in symptom score on
the population met criteria for the high-anxiety subgroup.
the HAM-D, was achieved in 66% of the comorbid
Patients with significant concurrent anxiety symptoms
patients in the venlafaxine XR group at week 12. This
were more likely to respond by 12 weeks (66.4%) than
response was higher than that seen with fluoxetine (52%)
those without significant anxiety symptoms (54.2%).
There was no significant difference in response rates for
In contrast to these reports, a study in primary care
sertraline versus imipramine. In a comparison of SSRIs
patients reported that anxiety can predict persistence of
among patients with anxious depression classified as
depression at baseline, 43 had coexisting anxiety disorder
Table 1. Personality Disorder and Treatment Response
(38 with social phobia). The risk for persistent depression
at 12 months was 44% greater among those with coexist-ing anxiety; this may largely reflect the type of anxiety
disorder that coexists with major depression. A recent
more effective than desipramine for depression in the
context of obsessive– compulsive disorder. This is consis-
tent with data showing that SSRIs are more effective than
drugs that primarily work through a norepinephrine mech-
anism. Given that SSRIs are effective for posttraumatic
stress disorder, social phobia, obsessive– compulsive dis-order, panic disorder, and generalized anxiety disorder, itis not surprising that these drugs are effective in treatingdepression in the context of anxiety disorders. Nonethe-
medication treatment, three showed no difference, and two
less, randomized trials evaluating whether the response
showed worse outcome for patients with personality dis-
rate is altered by the presence of each of these anxiety
orders (one with desipramine and one with maprotoline;
The largest study (Hirshfield 1998), with more
The data with psychotherapy may be significantly
than 600 patients, used sertraline and showed no differ-
ence between patients with and without significant per-
higher levels of anxiety predicted poor response to treat-
sonality pathology. reported that cluster B
ment. Additional studies are needed to evaluate whether
factors affected treatment response, with patients with
treatment response is different with specific comorbid
high reward dependence responding better to clomipra-
anxiety disorder such as obsessive– compulsive disorder
mine than to desipramine. In his review of these studies,
Mulder’s appropriate conclusion is as follows: “Whetheror not personality pathology significantly worsens out-come in patients with major depression appears to depend
Personality Traits and Disorders
on study design, since the rate of personality pathology
Personality traits have long been considered important in
varies markedly depending on how it is measured. In
the treatment outcome of depression. The study of person-
addition, depressed patients with personality pathology
ality traits and disorders is complex, and a variety of
appear less likely to receive adequate treatment in uncon-
methods has been used, including dimensional measures,
trolled studies. Finally, studies rarely control for depres-
such as neuroticism and the Tridimensional Personality
sion characteristics (e.g., chronicity, severity) that may
Questionnaire (TPQ) (Newman et al 2000), and categori-
influence outcome and be related to personality pathology.
cal measures such as DSM-based personality disorder
Overall, the best designed studies reported the least effect
scales. recently evaluated these studies in
of personality pathology on depression treatment outcome.
an excellent review. To summarize the results based on his
Clinically, this suggests that comorbid personality pathol-
review, neuroticism generally predicted poor long-term
ogy should not be seen as an impediment to good
response. The studies of shorter duration care were more
equivocal, with most not showing a relationship to short-term outcome. Studies with the TPQ were done at a latertime point and were better designed. The TPQ measures
novelty seeking, which reflects differences in the behav-ioral activation system; harm avoidance, which reflects
Comorbidity as generally seen in the context of major
differences in the behavioral inhibition system; and reward
depression appears to be only a minor factor determining
dependence, which reflects differences in the behavioral
treatment response. Medical comorbidity has a modest and
maintenance system. The largest study, by Nelson and
insignificant effect on short-term treatment response to
Clonninger (1997), showed that reward dependence pre-
SSRIs and other, more recently introduced medications.
The nihilistic assumption that antidepressants are not
The categorical assessment studies were highly varied
effective based on early studies with TCAs is not war-
in that a variety of methods was used. Seven studies used
ranted. In fact, even in patients with significant medical
both a standardized assessment and standardized treatment
problems, antidepressants are effective. Severity of anxi-
(sertraline, TCAs, ECT). Of the five studies that used
ety symptoms does not appear to have a major differential
effect on somatic treatment response, especially for the
sive and major depressive disorders. Arch Gen Psychiatry
SSRIs and other newer antidepressants, although it may
for psychotherapy. Anxiety disorders are well treated with
Joyce PR, Mulder RT, Cloninger CR (1994): Temperament
SSRIs, and thus the findings that these drugs work well for
predicts clomipramine and desipramine response in major
depression in the context of anxiety disorders is not
depression. J Affect Disord 30:35– 46.
surprising. At least for comorbid generalized anxiety and
Koenig HG, Goli V, Shelp F, Kudler HS, Cohen HJ, Meador KG,
depression, the presence of comorbidity does not affect
Blazer DG (1989): Antidepressant use in elderly medicalinpatients: Lesions from an attempted clinical trial. J Gen
treatment response. Personality disorder also does not
appear to have a major effect on treatment response.
Krishnan KR, Doraiswamy PM, Clary CM (2001): Clinical and
Although intuitively it is likely that severe personality
treatment response characteristics of late-life depression as-
disorder is likely to reduce treatment response, this has yet
sociated with vascular disease: A pooled analysis of two
to be studied. Neuroticism appears to be a predictor of
multicenter trials with sertraline. Prog Neuropsychopharma-col Biol Psychiatry 25:347–361.
Landerman R, George LK, Campbell RT, Blazer DG (1989):
Alternative models of the stress buffering hypothesis. Am J
Aspects of this work were presented at the conference, “Difficult-to-
Community Psychol 17:626 –642.
Treat Depression,” held April 21–22, 2002 in San Francisco, California. The conference was sponsored by the Society of Biological Psychiatry
Linn BS, Linn MW, Gurel L (1968): Cumulative illness rating
through an unrestricted grant provided by Eli Lilly and Company.
scale. J Am Geriatr Soc 16:622–626.
Montgomery SA, Asberg M (1979): A new rating scale designed
to be sensitive to change. Br J Psychiatry 134:382–389. References
Mulder RT (2002): Personality pathology and treatment outcome
Bielski RJ, Friedel RO (1976): Prediction of tricyclic antidepres-
in major depression: A review. Am J Psychiatry 159:359 –
sant response: A critical review. Arch Gen Psychiatry
Nelson E, Cloninger CR (1997): Exploring the TPQ as a possible
Fava M, Bouffides E, Pava JA, McCarthy MK, Steingard RJ,
predictor of antidepressant response to nefzaodone in a large
Rosenbaum JF (1994): Personality disorder comorbidity with
multi-site study. J Affect Dis 44:197–200.
major depression and response to fluoxetine treatment. Psy-
Newman JR, Ewing SE, McColl RD, Borus JS, Nierenberg AA,
chother Psychosom 62:160 –167.
Pava J, Fava M (2000): Tridemensional Personality Question-
Fava M, Rosenbaum JF, Hoog SL, Tepner RG, Koop JB, Nilsson
naire and treatment response in major depressive disorder: a
ME (2000): Fluoxetine versus sertraline and paroxetine in
negative study. J Affect Dis 57:241–247.
major depression: Tolerability and efficacy in anxious depres-sion. Affect Disord 59:119 –126.
Paykel ES (1972): Depressive typologies and response to ami-
triptyline. Br J Psychiatry 120:147–156.
Fawcett J, Barkin RL (1998): A meta-analysis of eight random-
ized, double-blind, controlled clinical trials of mirtazapine for
Peselow ED, Fieve RR, DiFiglia C (1992): Personality traits and
the treatment of patients with major depression and symptoms
response to desipramine. J Affect Disord 24:209 –216.
of anxiety. J Clin Psychiatry 59:123–127.
Popkin MK, Callies AL, Mackenzie TB (1985): The outcome of
Feske U, Frank E, Kupfer DJ, Shear MK, Weaver E (1998):
antidepressant use in the medically ill. Arch Gen Psychiatry
Anxiety as a predictor of response to interpersonal psycho-
therapy for recurrent major depression: An exploratory inves-
Radloff LS (1977): The CES-D scale: A self-report depression
tigation. Depress Anxiety 8:135–141.
scale for research in the general population. Appl Psychol
Gaynes BN, Magruder KM, Burns BJ, Wagner HR, Yarnall KS,
Broadhead WE (1999): Does a coexisting anxiety disorderpredict persistance of depressive illness in primary care
Robins LN, Helzer JE, Croughan J, Ratcliff KS (1981): National
patients with major depression? Gen Hosp Psychiatry 21(3):
Institute of Mental Health Diagnostic Interview Schedule: Its
history, characteristics, and validity. Arch Gen Psychiatry38:381–389.
George LK, Blazer DG, Hughes DC, Fowler N (1989): Social
support and the outcome of major depression. Br J Psychiatry
Rudolph RL, Entsuah R, Chitra R (1998): A meta-analysis of the
effects of venlafaxine on anxiety associated with depression. J Clin Psychopharmacol 18:136 –144.
Gill D, Hatcher S (2000): Antidepressants for depression in
medical illness. Cochrane Database Syst Rev. (4):CD001312.
Russell JM, Koran LM, Rush J, Hirschfeld RM, Harrison W,
Hirschfeld RM, Russell JM, Delgado PL, Fawcett J, Friedman
Friedman ES, et al (2001): Effect of concurrent anxiety on
RA, Harrison WM, et al (1998): Predictors of response to
response to sertraline and imipramine in patients with chronic
acute treatment of chronic and double depression with sertra-
depression. Depress Anxiety 13:18 –27.
line or imipramine. J Clin Psychiatry 59:669 – 675.
Sato T, Sakado K, Sato S (1993): Is there any specific personality
Hoehn-Saric R, Ninan P, Black DW, Stahl S, Greist JH, Lydiard
disorder or personality disorder cluster that worsens the
B, et al (2000): Multicenter double-blind comparison of
short-term treatment outcome of major depression? Acta
sertraline and desipramine for concurrent obsessive-compul-
Psychiatr Scand 88:342–349.
Silverstone PH, Salinas E (2001): Efficacy of venlafaxine extended
Steffens DC, McQuoid DR, Krishnan KRR (2002): The Duke
release in patients with major depressive disorder and comorbid
generalized anxiety disorder. J Clin Psychiatry 62:523–529.
(STAGED) approach. Psychopharm Bull 36:58 –68.
Sonawalla SB, Spillmann MK, Kolsky AR, Alpert JE, Nieren-
Tollefson GD, Holman SL, Sayler ME, Potvin JH (1994):
berg AA, Rosenbaum JF, Fava M (1999): Efficacy of fluvox-
Fluoxetine, placebo, and tricyclic antidepressants in major
amine in the treatment of major depression with comorbid
depression with and without anxious features. J Clin Psychi-
anxiety disorders. J Clin Psychiatry 60(9):580 –583.
Steffens DC, Doraiswamy PM, McQuoid DR (2001): Bupropion
Zimmerman M, Chelminski I, McDermut W (2002): Major
SR in the naturalistic treatment of elderly patients with major
depressive disorder and Axis I diagnostic comorbidity. J Clin
depression. Int J Geriatr Psychiatry 16:862–865.
J_ID: Z7V Customer A_ID: 06-0418 Cadmus Art: CCI 21093 Date: 5-JANUARY-07Catheterization and Cardiovascular Interventions 69:000–000 (2007)Late Stent Thrombosis: Considerations and PracticalAdvice for the Use of Drug-Eluting Stents:A Report From the Society for Cardiovascular Angiographyand Interventions Drug-eluting Stent Task ForceJohn McB. Hodgson,1 * MD, FSCAI, Gregg W. Stone,2 MD, FS
Natural disaster and Rural Planning The Association of Rural Planning, Japan Head of the symposium organizing committee Scope and Objective: The natural environmental structure of Asia-Pacific Rim and Monsoon Asian reveals vulnerable induced by environmental condition. Additional factors are rapid land cover change and urbanization in the lowlands or river deltas with large expanding
 be treated with antidepressants to produce one dropoutfrom treatment, which would not have occurred had theybeen given placebo. By inferencefrom this review, one can conclude that medical comor-bidity is not a major factor in treatment response.
be treated with antidepressants to produce one dropoutfrom treatment, which would not have occurred had theybeen given placebo. By inferencefrom this review, one can conclude that medical comor-bidity is not a major factor in treatment response.