He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Therapiepraktijkavo.nl
Long-term Improvement in Functional DyspepsiaUsing Hypnotherapy
EMMA LOUISE CALVERT,* LESLEY ANNE HOUGHTON,* PATRICIA COOPER,* JULIE MORRIS,‡and PETER JAMES WHORWELL**Department of Medicine and ‡Department of Medical Statistics, Education and Research Centre, Wythenshawe Hospital,Southmoor Road, Manchester, United Kingdom
Functional dyspepsia (FD) and irritable bowel syn-
drome (IBS) account for more than 1⁄2 of the gastro-
enterologist’s workload1 and are also the most commongastrointestinal problems seen in primary care settings.2
Background & Aims: We have shown hypnotherapy (HT)
Although FD and IBS share some clinical features, they
to be effective in irritable bowel syndrome, with long-
can be distinguished symptomatically into 2 distinct
term improvements in symptomatology andquality of
entities.3 There is also probably some overlap in their
life (QOL). This study aimed to assess the efficacy of HT
underlying pathophysiology, with abnormalities of both
in functional dyspepsia (FD). Methods: A total of 126 FDpatients were randomized to HT, supportive therapy plus
motility4 and visceral sensitivity5,6 likely contributory.
placebo medication, or medical treatment for 16 weeks.
The most recently accepted definition of FD (Rome II)
Percentage change in symptomatology from baseline
is recurrent (at least 12 weeks/year) epigastric pain with
was assessedafter the 16-week treatment phase (short-
no evidence of organic disease and associated upper ab-
term) andafter 56 weeks (long-term) with 26 HT, 24
dominal bloating, early satiety, nausea, vomiting, and
supportive therapy, and29 medical treatment patients
feelings of fullness.3 It has been traditional to divide FD
completing all phases of the study. QOL was measured
into reflux-like, ulcer-like, dysmotility-like, and nonspe-
as a secondary outcome. Results: Short-term symptom
cific dyspepsia,7 although the clinical utility of this
scores improvedmore in the HT group (median, 59%)
classification has been questioned.1 With respect to treat-
than in the supportive (41%; P ؍ 0.01) or medical
ment trials, there is little evidence that subgrouping is
treatment (33%; P ؍ 0.057) groups. HT also benefited
helpful,3 although patients with reflux symptoms are
QOL (42%) comparedwith either supportive therapy
(10% [P < 0.001]) or medical treatment (11% [P <
FD is extremely common, affecting up to 25% of the
0.001]). Long-term, HT significantly improvedsymptoms
population.3,7,9 Unfortunately, there are even fewer ef-
(73%) comparedwith supportive therapy (34% [P <
fective medications for this condition than for IBS, and
0.02]) or medical treatment (43% [P < 0.01]). QOL
those that are used, such as proton pump inhibitors and
improvedsignificantly more with HT (44%) than with
prokinetics, are expensive. This condition is very costly
medical treatment (20% [P < 0.001]). QOL did improve
in both economic and social terms, as a result of these
in the supportive therapy (43%) group, but 5 of these
patients consulting frequently7 and taking time off
patients commenced taking antidepressants during fol-
work.9 The costs related to FD have recently been esti-
low-up. A total of 90% of the patients in the medical
mated to exceed $1.2 billion per year in the United
treatment group and82% of the patients in the support-
ive therapy group commenced medication during follow-
We have previously shown that hypnotherapy (HT) is
up, whereas none in the HT group did so (P < 0.001). Those in the HT group visitedtheir general practitioner
extremely effective in treating IBS, leading to long-term
or gastroenterologist significantly less (median, 1) than
improvement of symptoms and quality of life,10–12 and
did those in the supportive therapy (median, 4) andmedical treatment (median, 4) groups during follow-up
Abbreviations used in this paper: FD, functional dyspepsia; HAD,
(P < 0.001). Conclusions: HT is highly effective in the
hospital anxiety anddepression; HT, hypnotherapy; IBS, irritable bowel
long-term management of FD. Furthermore, the dra-
2002 by the American Gastroenterological Association
matic reduction in medication use and consultation rate
this has been confirmed by other investigators.13,14 HT is
commonly considered a purely psychotherapeutic inter-
The study was of a randomized (stratified for gender),
vention; not as well appreciated is the fact that it can also
controlled, parallel design in which patients were randomly
modify processes not usually considered as being under
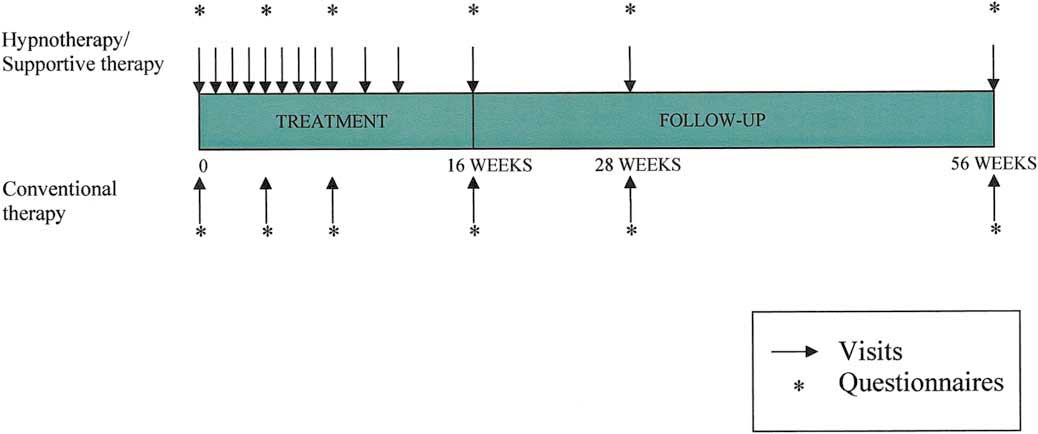
assigned to 1 of 3 groups. Patients underwent a 16-week
conscious control.15,16 HT has also been demonstrated to
treatment phase of HT, supportive therapy plus placebo med-
have the capacity to normalize visceral sensitivity and
ication or medical treatment with a histamine-2 antagonist
modulate motility in the gastrointestinal system.17,18
(ranitidine 150 mg twice daily), followed by a 40-week fol-
The aim of this study was to assess the efficacy of HT
low-up phase during which no further study interventions
compared with supportive therapy coupled with placebo
were undertaken. The active ranitidine, supplied by Glaxo-
medication or with medical management in the short-
Wellcome (United Kingdom), was in the form of a white
and long-term treatment of FD. Particular attention was
tablet that did not resemble either the over-the-counter orprescription versions of the drug. The treatment phase con-
given to controlling for time spent with patients.
sisted of 12, 30-minute visits for patients receiving HT orsupportive therapy and only 4 visits, to dispense medication,
for the patients randomized to medical treatment (Figure 1). Patients were assessed at baseline (week 0) and at weeks 4, 8,
16, 28, and 56 by an independent blind assessor, who was
All patients attending the endoscopy unit at the Uni-
unaware of the treatment randomization. Patients were specif-
versity Hospital of South Manchester with dyspeptic symp-
ically instructed about the importance of the assessor remain-
toms and a negative endoscopy were considered for the study,
ing blind to treatment and were told to avoid mentioning their
and those fulfilling the Rome I19 criteria for FD were recruited.
treatment modality to the assessor and subsequently, during
Patients were excluded if they had predominant gastroesoph-
ageal reflux-like symptoms, had a history of peptic ulcer
Symptom scores were measured using a variation of a vali-
disease, or were regularly using nonsteroidal anti-inflamma-
dated symptom scoring system22 developed in our department
tory drugs. All patients with a history of abdominal surgery,
for use in IBS. Quality-of-life (QOL) scores were assessed using
with the exception of appendectomy, cholecystectomy, or hys-
a QOL instrument validated in affective disorder,23 modified
terectomy more than 1 year previously, were also excluded.
for use in functional bowel disorders11 and subsequently used
Patients with Helicobacter pylori infection were also excluded,
in a number of HT studies, in which it has proven to be
because the role of this organism in the pathogenesis of func-
sensitive to changes over time.12,24,25 Patients’anxiety and
tional dyspepsia is still somewhat controversial.20,21 Patients
depression levels were also assessed using the hospital anxiety
with concomitant symptoms consistent with IBS were not
and depression (HAD) scale26 at the start and end of the
excluded, provided that their FD symptoms were more pre-
treatment phase only. Furthermore, the economic impact of
dominant. The study was approved by the local ethics com-
FD for the year preceding treatment and throughout the study
mittee, and all patients gave written informed consent.
was assessed by recording the number of consultations with a
Figure 1. Study protocol. Reprinted with permission from Department of Medical Illustration, Withington Hospital, Manchester, England.
general practitioner or physician in the outpatient department,
number of clinical procedures, work absences, and inpatient
It was calculated that 17 subjects in each group were
stays. Medication use was also recorded, and prescribing was
needed to achieve an 80% power to detect a significant differ-
left entirely to the discretion of the patients’primary care
ence in percentage improvement of 40% between the HT and
physicians or consultants, who were not involved in the study
control groups using a 2-sample t test, assuming that the data
and were kept blind to the treatment modality.
followed a normal distribution with a common standard de-viation of 40. However, skewness of the data with non-normal
distribution was anticipated. Thus a sample size of 25–30 in
HT was provided by a qualified therapist as described
each group was considered appropriate to adjust for the non-
in detail elsewhere.27 Briefly, the patients were given a tutorial
normality of the data and to compare HT with each of the 2
that included basic pathophysiologic concepts of FD and how
control groups. Assessment of the long-term efficacy of HT
HT might be used to treat the condition. Hypnosis was then
was considered a particularly important part of the study that
induced using eye fixation and closure, followed by progressive
could be compromised if dropouts reduced the size of any of
muscular relaxation and standard deepening procedures. Sug-
the treatment groups before this phase was established. There-
gestions of disease improvement were made using both tactile
fore, in the event of an unequal dropout rate, the contingency
and imagery techniques. The patient was asked to place a hand
for a process of uneven randomization was adopted, to ensure
on the abdomen and imagine a reduction of all symptoms.
that similar numbers entered the follow-up phase.
Suggestions of positive changes in motor activity, sensitivity,
The analysis was performed on an intent-to-treat basis for
and secretion of acid and mucus were also introduced. All of
both the short- and long-term phases of the study, with the
these concepts of improvement were reinforced by any appro-
last available data for an individual carried forward as an
priate visualization processes with which the patient felt com-
endpoint. Symptom and QOL data followed a non-normal
distribution; hence, nonparametric summary statistics (medi-ans and interquartile ranges) were used to describe the data.
Short-term and long-term changes between groups using per-
centage change scores from baseline were assessed usingKruskal–Wallis tests, followed by Mann–Whitney U tests
This involved an experienced clinical research assistant
with Bonferroni’s correction for multiple group comparisons. P
providing general supportive advice about FD and listening to
values unadjusted for multiple outcome comparisons are pre-
patients’concerns about the condition. No specific psychologic
sented. However, as an acknowledgement of the problem of
intervention was undertaken, and sessions lasted exactly the
multiple comparisons, only P values Ͻ 0.01 were taken to
same length of time as those devoted to hypnotherapy. Placebo
provide reasonable evidence of a difference between groups
ranitidine (GlaxoWellcome) was prescribed on a twice-daily
with respect to individual secondary outcome measures. Com-
basis for the duration of the treatment phase and was in the
parisons of medication use between groups during the fol-
form of a white tablet that did not resemble either the pre-
low-up phase were assessed using 2 tests.
scription or the over-the-counter form of this medication. Patients were told that they might be receiving either a
placebo or an active form of a drug that might help their
Recruitment of patients and their flow through
condition, was entirely safe, and was not being tested in a
each stage of the study, as recommended by the CON-
SORT statement,28 are illustrated in Figure 2. A total of149 patients were eligible for the study, of which 23
(15%) declined to participate, leaving 126 patients. Of
All symptom (pain severity and frequency, nausea,
these 126 patients, 32 were randomized to receive HT;
poor appetite, early satiety, bloating, and belching) and QOL
48, to supportive therapy; and 46, to medical treatment.
(psychological and physical well-being, mood, locus of control,
In these groups, 27, 32, and 34 patients, respectively,
social relationships, work, hobbies, and finances) measures
completed the treatment phase. During the acute phase,
were assessed using visual analogue scales of 0 –10 cm (10 cm
8 (6%) patients (3 in the HT group, 2 in the medical
being maximum), from which the percentage of the changes
group, and 2 in the supportive group) withdrew before
from baseline to the end of both the treatment (short-term)
receiving any treatment, 6 (5%) because of the time
and follow-up (long-term) phases were obtained. The primaryoutcome measure was the percentage change from baseline of
commitment, and 2 (2%) for other reasons. Another 23
the total score derived from the individual symptom measures
(18%) patients (0 from the HT group, 13 from the
at the end of the short- and long-term phases. QOL was
supportive group, and 10 from the medical group) with-
considered a secondary outcome measure, as were the individ-
drew from the acute phase because the treatment was not
ual symptom scores and data on health care–seeking behavior
working (P Ͻ 0.001 hypnotherapy vs. medical and sup-
portive). Because of the high dropout rates in the 2
Figure 2. Study flow diagram. Reprinted with permission fromDepartment of Medical Illus-tration, Withington Hospital,Manchester, England.
control groups and to maintain equal numbers of pa-
group. To control for any variations in scores, percentage
tients entering the follow-up phase of the study, more
change rather than actual score was used for statistical
patients were randomized to receive the control thera-
comparisons. Table 2 gives the actual scores obtained for
pies. Fourteen (11%) patients were lost during the fol-
total symptoms and QOL at baseline, the end of treat-
Table 1 summarizes the initial total symptom and
Figure 3 shows a comparison of the primary out-
QOL scores and their individual components for each
come measure (total symptom score) for the 3 groups at
Table 1. Patient Symptom and Quality of Life Scores Before Entering Into the Study
NOTE. Expressed as median (interquartile range). Reprinted with permission from Department of Medical Illustration, Withington Hospital, Manchester, England.
all time points during the course of the study. As can be
significantly improved following HT compared with the
seen, a highly significant improvement in symptoms
occurred in the HT patients compared with the other 2groups by the end of the short-term phase, and this was
Figure 5 shows a comparison of the total QOL
Short-Term. Figure 4 illustrates the percentage
scores for the 3 groups at all time points during the
improvement in all symptoms at the end of the short-
course of the study. QOL significantly improved in the
term phase. HT improved total symptom scores [per-
HT group compared with the other 2 groups in the
centage improvement, median (IQR) 59% (26%– 85%)]
short-term. However, in the long-term, although HT
more than either supportive [40.7% (10%–59%); P ϭ
significantly improved QOL compared with medical
0.057] or medical [33% (Ϫ27% to Ϫ47.8%); P ϭ 0.01]
treatment, the supportive group did exhibit a slow im-
therapy. Significant differences favoring HT for the in-
provement over time. A likely explanation for the unex-
pected improvement in QOL in the supportive group
Long-term. At the end of the follow-up phase,
was that 5 patients in this group (compared with none in
patients receiving HT were significantly improved for
the other control group) began taking antidepressants
the primary outcome measure [73% (26%–96%)] com-
during the follow-up phase, as shown in Table 3, which
pared with either of the other 2 control groups [support-
led to an improvement of this parameter.
ive, 34% (Ϫ24%–71%), P Ͻ 0.02; medical, 43%
Short-term. Figure 6 illustrates the percentage
(15%–57%), P Ͻ 0.01]. In addition, all of the individual
improvement in all components of QOL at the end of the
symptoms with the sole exception of nausea remained
short-term phase. As can be seen, this was significantly
Table 2. Scores for Total Symptoms and Quality of Life at Baseline and the End of the Short- and Long-Term Phases
NOTE. Expressed as median (interquartile range). Reprinted with permission from Department of Medical Illustration, Withington Hospital,Manchester, England.
Figure 3. Symptom change throughout the study. Reprinted with
Figure 5. QOL change throughout the study. Reprinted with permis-
permission from Department of Medical Illustration, Withington Hos-
sion from Department of Medical Illustration, Withington Hospital,
improved by HT [42% (31%– 69%)] compared with
supportive, 3.6 (2.8 – 4.7); medical, 3.6 (2.5– 4.5); total
both the medical [11% (Ϫ9%– 46.6%) P Ͻ 0.001] and
QOL score: HT, 5.1 (4.6 – 6.5); supportive, 5.1 (4.7–
supportive [10% (Ϫ10%–21.2%); P Ͻ 0.001] groups.
Significant differences favoring HT for the individualscores were also observed.
Long-term. At the end of the follow-up phase,
The initial median HAD (anxiety) scores were at
QOL improved significantly with HT [44% (24%– 69%)]
the upper limits of the normal range (score Յ9 is nor-
compared with the medical [20% (10%–26%); P Ͻ
mal), whereas those for depression were well within
0.01] but not with the supportive group [43% (9%–
normal limits (score Յ9 is normal). Patients in both the
60%)], for reasons already explained.
HT and supportive groups experienced a significant re-duction in anxiety during the treatment phase of the
study (anxiety score expressed as median [IQR]: HT pre,
There were no significant differences between the
8.5 [4.5–11.5], post, 5 [4.5–7], P ϭ 0.03; supportive
initial symptom and QOL scores in any of the treatment
pre, 10 [8 –11], post, 7 [4 –9], P ϭ 0.02). Anxiety was
groups for those patients who completed the treatment
not significantly changed after medical treatment (pre, 8
phase [total symptom score: HT, 3.3 (2.3–5.1); support-
[3.3–10.8]; post, 6.5 [4 –9]). However, there were no
ive, 4.4 (3.4 –5.9); medical, 3.8 (2.9 –5); total QOL
significant differences in anxiety reduction during the
score: HT, 5.3 (4.6 – 6.1); supportive, 5.3 (4.2– 6.9);
treatment phase between the 3 groups.
medical, 6.1 (5.4 –7.3)] compared with those whodropped out [total symptom score: HT, 3.9 (3–5.4);
Table 3 provides data on medication use and
consultation behavior during the 40-week follow-up
Figure 4. Symptom change during the short-term phase. Reprinted
Figure 6. QOL change during the short-term phase. Reprinted with
with permission from Department of Medical Illustration, Withington
permission from Department of Medical Illustration, Withington Hos-
Table 3. Medication Use and Consultation Rate of Patients
term basis, even though they are of questionable efficacy.
Furthermore, medically treated patients continue to con-
sult much more than those managed with HT.
Interestingly, there were significantly more dropouts
due to treatment failure in the 2 control groups than in
the HT group (P Ͻ 0.001). The symptom severity of the
dropouts was no worse than those remaining in the trial,
suggesting that these were true treatment failures rather
than being more severe. For HT to be an economically
feasible treatment of any condition, it must be effective
in the long-term without the need for continuing ses-
sions, irrespective of any short-term gains. Thus it was
essential that sufficient patients be recruited to each arm
for the follow-up phase of the study; this was achieved by
replacing dropouts. This policy inevitably resulted in
recruitment of patients more likely to respond to controltherapies and therefore biased the trial against HT for
NOTE. Expressed as median (interquartile range).
both the long- and short-term phases. Thus the results
*P Ͻ .001 vs. hypnotherapy. Reprinted with permission from Department of Medical Illustration,
achieved for HT are even more encouraging.
Withington Hospital, Manchester, England.
There is a strong need for good quality-controlled
trials in the area of “complementary” therapy (although
phase. As can be seen, 82% of patients in the supportive
some claim that these are impossible to undertake).
group and 90% of patients in the medical group resorted
Identifying suitable comparator groups presents some
to some form of medication, compared with 0 in the HT
problems, and we felt it appropriate to have 2 control
group (P Ͻ 0.001 HT vs. medical and supportive). The
arms. The medical group provided an estimate of the
number of general practitioner or physician consultations
standard response rate to medical treatment. The sup-
was also significantly lower after HT than after either
portive group controlled for the time spent with the
medical or supportive treatment during follow-up.
patient during HT, the necessity for which was con-firmed by the reduced anxiety levels in the 2 groups
receiving more attention. Those receiving supportivetreatment were also given a placebo tablet, which served
This study clearly demonstrates that HT is more
effective than medical treatment or supportive therapy
3 functions: (1) to control for medication given to the
plus placebo medication in both the short- and long-
medically treated group, (2) to maximize response to
term management of FD. HT not only improves all
treatment to the greatest extent possible, and (3) as a
aspects of symptomatology and QOL, but also has con-
result of needing further supplies of medication at each
siderable economic advantages. Of particular interest is
visit, ensuring they returned for sessions.
the striking difference in the medication needs of the 3
The mode of action of HT remains speculative but
groups. None of the patients receiving HT resumed any
probably involves a number of different factors. There is
form of drug therapy, whereas 90% of patients in the
undoubtedly a positive response to the increased atten-
medical group and 82% of patients in the supportive
tion, but this should have been adequately controlled for
group felt it necessary to begin some form of treatment.
by the inclusion of a group receiving supportive therapy.
Five patients who received supportive therapy also began
Moreover, it is likely that the general relaxation associ-
taking antidepressants during follow-up; this contrib-
ated with hypnosis provides a nonspecific psychothera-
uted to the somewhat surprising improvement in QOL
peutic response reducing anxiety. However, it should be
observed in this group. A standard course of HT requires
noted that although anxiety declined during HT, there
up to 12 sessions and thus at face value appears rather
was no correlation with symptom improvement (r ϭ
expensive in the short-term. However, this fails to take
0.220, P ϭ 0.185), suggesting that the beneficial effect
into account the fact that once treated, a patient seldom
cannot be attributed to anxiety reduction alone. The
needs any further intervention—in sharp contrast to the
observation that HT can influence gastrointestinal phys-
conventional treatment of FD, in which expensive drugs
iologic function17,18 might suggest that the improve-
(e.g., proton pump inhibitors) are often used on a long-
ment observed in FD may result from some modification
of gastric motility, gastric accommodation, or visceral
syndrome with hypnotherapy. Appl Psychophysiol Biofeedback
sensitivity. It is of interest that although HT has been
14. Vidakovic-Vukic M. Hypnotherapy in the treatment of irritable
shown to modify gastric acid secretion,15 its effects on
bowel syndrome: methods and results in Amsterdam. Scand J
other parameters of gastric physiology have not yet been
Gastroenterol 1999; (suppl 230):49 –51.
assessed, although studies of this nature are now under-
15. Stacher G, Berner P, Naske R, Schuster P, Bauer P, Starker H,
Schulz D. Effect of hypnotic suggestion of relaxation on basal and
betazole-stimulated gastric acid secretion. Gastroenterology
These results, taken in conjunction with those ob-
tained for IBS,10,11–14,24,25 confirm the efficacy of HT in
16. Black S, Humphrey JH, Niven JSF. Inhibition of the Mantoux
reaction by direct suggestion under hypnosis. Br Med J 1963;I:
a group of functional disorders that are especially diffi-
cult to treat. They also warrant the evaluation of this
17. Prior A, Colgan SM, Whorwell PJ. Changes in rectal sensitivity
form of treatment in other functional problems not nec-
after hypnotherapy in patients with irritable bowel syndrome. Gut
essarily confined to the gastrointestinal tract.
18. Whorwell PJ, Houghton LA, Taylor E, Maxton DG. Physiological
effects of emotion: assessment via hypnosis. Lancet 1992;2:
19. Colin-Jones D. The management of dyspepsia. Scand J Gastro-
1. Drossman DA, Li A, Andruzzi E, Temple RD, Talley NJ, Thompson
WG, Whitehead WE, Janssens J, Funch-Jensen P, Corazziari E,
20. Talley NJ, Janssens J, Laurilsen K, Racz I, Bolling-Sterneuald E.
Richter JE, Koch GG. U.S. householder survey of functional gas-
Eradication of Helicobacter pylori in functional dyspepsia: a ran-
trointestinal disorders: prevalence, sociodemography and health
domised double-blind placebo-controlled trial with 12-months fol-
impact. Dig Dis Sci 1993;38:1569 –1580.
2. Bommelaer G, Rouch M, Dapoigny M, Pais D, Loisy P, Gualino M,
21. Blum AL, Talley NJ, O’Morain C, VanZanten SV, Labenz J, Stolte
Tournut R. Epidemiology of intestinal function disorders in appar-
M, Louw JA, Stubberod A, Theodors A, Sundin M, Bolling-Ster-
ently healthy people. Gastroenterol Clin Biol 1986;10:7–12.
neuald E, Junghard O. Lack of effect of treating Helicobacter
3. Talley NJ, Stanghelllini V, Heading RC, Koch KL, Malagelada JR,
pylori infection in patients with non-ulcer dyspepsia. N Engl J Med
Tygat GNJ. Functional gastroduodenal disorders. In: Drossman
DA, Corazziari E, Talley NJ, Grant Thompson W, Whitehead WE,
22. Francis CY, Morris J, Whorwell PJ. The irritable bowel severity
eds. Rome II: The functional gastrointestinal disorders. 2nd ed.
scoring system: a simple method of monitoring irritable bowel
McLean, VA: Degnon Associates, 2000.
syndrome and its progress. Aliment Pharmacol Ther 1997;11:
4. Camilleri M, Phillips SF. Disorders of small intestinal motility.
Gastroenterol Clin North Am 1989;18:405– 424.
23. Dunbar GC, Stoker MJ, Hodges TCP, Beaumont G. The develop-
5. Ness TJ, Metcalf AM, Gebhart GF. A psychophysical study in
ment of SBQOL: a unique scale for measuring quality of life. Br J
humans using colonic distension as a noxious visceral stimulus.
24. Gonsalkorale WM, Cruickshanks P, Whelan V, Miller V, Randles J,
6. Mearin F, Cucala M, Azpiroz F, Malagelada JA. The origin of
Cooper P, Whorwell PJ. Improvement in symptoms with hypno-
symptoms on the brain-gut axis in functional dyspepsia. Gastro-
therapy is associated with cognitive change (abstr). Gastroenter-
7. Jones RH, Lydeard ST, Hobbs FDR, Kenkre JE, Williams EI, Jones
25. Gonsalkorale WM, Miller V, Afzal A, Whorwell PJ. Hypnotherapy
SJ, Repper JA, Caldow JL, Dunwoodie WM, Bottomley JM. Dys-
for irritable bowel syndrome: improvement is long-lasting and
pepsia in England and Scotland. Gut 1990;31:401– 405.
reduces health care costs (abstr). Gastroenterology 2002;122:
8. Talley NJ, Silverstein M, Agreus L, Nyren O, Sonnenberg A, Holt-
man G. AGA technical review: evaluation of dyspepsia. Gastroen-
26. Zigmond AS, Snaith RP. The hospital anxiety and depression
scale. Acta Psychiatr Scand 1983;67:361–370.
9. Kurata JH. Gastritis/nonulcer dyspepsia. In: Everhart JE, ed.
27. Whorwell PJ. Hypnosis and the gastrointestinal system. Br J Hosp
Digestive disease in the U.S.: epidemiology and impact. Wash-
ington, DC: National Institutes of Health, National Institute of
28. Begg C, Eastwood S, Horton R, Moher D, Olkin I, Pitkin R, Rennie
Diabetes, Digestive and Kidney Diseases Publication 94-1447,
D, Shulz KF, Simel D, Stroop DF. Improving the quality of report-
ing of randomised controlled trials. The CONSORT statement.
10. Whorwell PJ, Prior A, Farragher EB, 1984. Controlled trial of
hypnotherapy in the treatment of severe refractory irritable bowelsyndrome. Lancet 1984;2:1232–1234.
11. Houghton LA, Heyman DJ, Whorwell PJ. Symptomatology, quality
ReceivedMay 3, 2002. AcceptedAugust 27, 2002.
of life and economic features of irritable bowel syndrome—the
Address requests for reprints to: Peter J. Whorwell, M.D., Depart-
effect of hypnotherapy. Aliment Pharmacol Ther 1996;10:91–95.
ment of Medicine, Education and Research Centre, Wythenshawe
12. Gonsalkorale WM, Houghton LA, Whorwell PJ. Hypnotherapy for
Hospital, Southmoor Road, Manchester M23 9LT, United Kingdom.
irritable bowel syndrome: a large-scale audit of a clinical service
e-mail: [email protected]; fax: (44) 161-434-5194.
with examination of factors influencing responsiveness. Am J
Supportedby a grant from the Wellcome Trust.
The authors thank Professor M. J. S. Langman for helpful criticism
13. Galvolski TE, Blanchard EB. The treatment of irritable bowel
during the preparation of this manuscript.
Analogpräparate und Leitsubstanzen Herbstsymposium der korporativen Mitglieder der DGIM 18. Oktober 2007, Wiesbaden Bertram Häussler IGES Institut IGES Institut für Gesundheits- und Sozialforschung GmbHWichmannstr. 5 · D-10787 Berlin · Germany +49 30 230 80 9-0 ¬ +49 30 230 80 9-11 www.iges.de Übersicht Zur Methode von Fricke und Klaus IGES-Studie zur Evaluation
Schulmedizin und Alternativmedizin – Die Sicht der Schulmedizin Prof. Dr. Rudolf Joss, Luzern „Natural-born killers“ – so titelte kürzlich die angesehene Zeitschrift Nature Medicine einen Beitrag über Phytotherapie. Steve Bechler, ein Baseball-Spieler der Baltimore Orioles hatte mit Hilfe sogenannter „herbal supplements“, also mit pflanzlichen Nahrungsmittelzusätzen vers
 this has been confirmed by other investigators.13,14 HT is
commonly considered a purely psychotherapeutic inter-
The study was of a randomized (stratified for gender),
vention; not as well appreciated is the fact that it can also
controlled, parallel design in which patients were randomly
modify processes not usually considered as being under
assigned to 1 of 3 groups. Patients underwent a 16-week
conscious control.15,16 HT has also been demonstrated to
treatment phase of HT, supportive therapy plus placebo med-
have the capacity to normalize visceral sensitivity and
ication or medical treatment with a histamine-2 antagonist
modulate motility in the gastrointestinal system.17,18
(ranitidine 150 mg twice daily), followed by a 40-week fol-
The aim of this study was to assess the efficacy of HT
low-up phase during which no further study interventions
compared with supportive therapy coupled with placebo
were undertaken. The active ranitidine, supplied by Glaxo-
medication or with medical management in the short-
Wellcome (United Kingdom), was in the form of a white
and long-term treatment of FD. Particular attention was
tablet that did not resemble either the over-the-counter orprescription versions of the drug. The treatment phase con-
given to controlling for time spent with patients.
this has been confirmed by other investigators.13,14 HT is
commonly considered a purely psychotherapeutic inter-
The study was of a randomized (stratified for gender),
vention; not as well appreciated is the fact that it can also
controlled, parallel design in which patients were randomly
modify processes not usually considered as being under
assigned to 1 of 3 groups. Patients underwent a 16-week
conscious control.15,16 HT has also been demonstrated to
treatment phase of HT, supportive therapy plus placebo med-
have the capacity to normalize visceral sensitivity and
ication or medical treatment with a histamine-2 antagonist
modulate motility in the gastrointestinal system.17,18
(ranitidine 150 mg twice daily), followed by a 40-week fol-
The aim of this study was to assess the efficacy of HT
low-up phase during which no further study interventions
compared with supportive therapy coupled with placebo
were undertaken. The active ranitidine, supplied by Glaxo-
medication or with medical management in the short-
Wellcome (United Kingdom), was in the form of a white
and long-term treatment of FD. Particular attention was
tablet that did not resemble either the over-the-counter orprescription versions of the drug. The treatment phase con-
given to controlling for time spent with patients.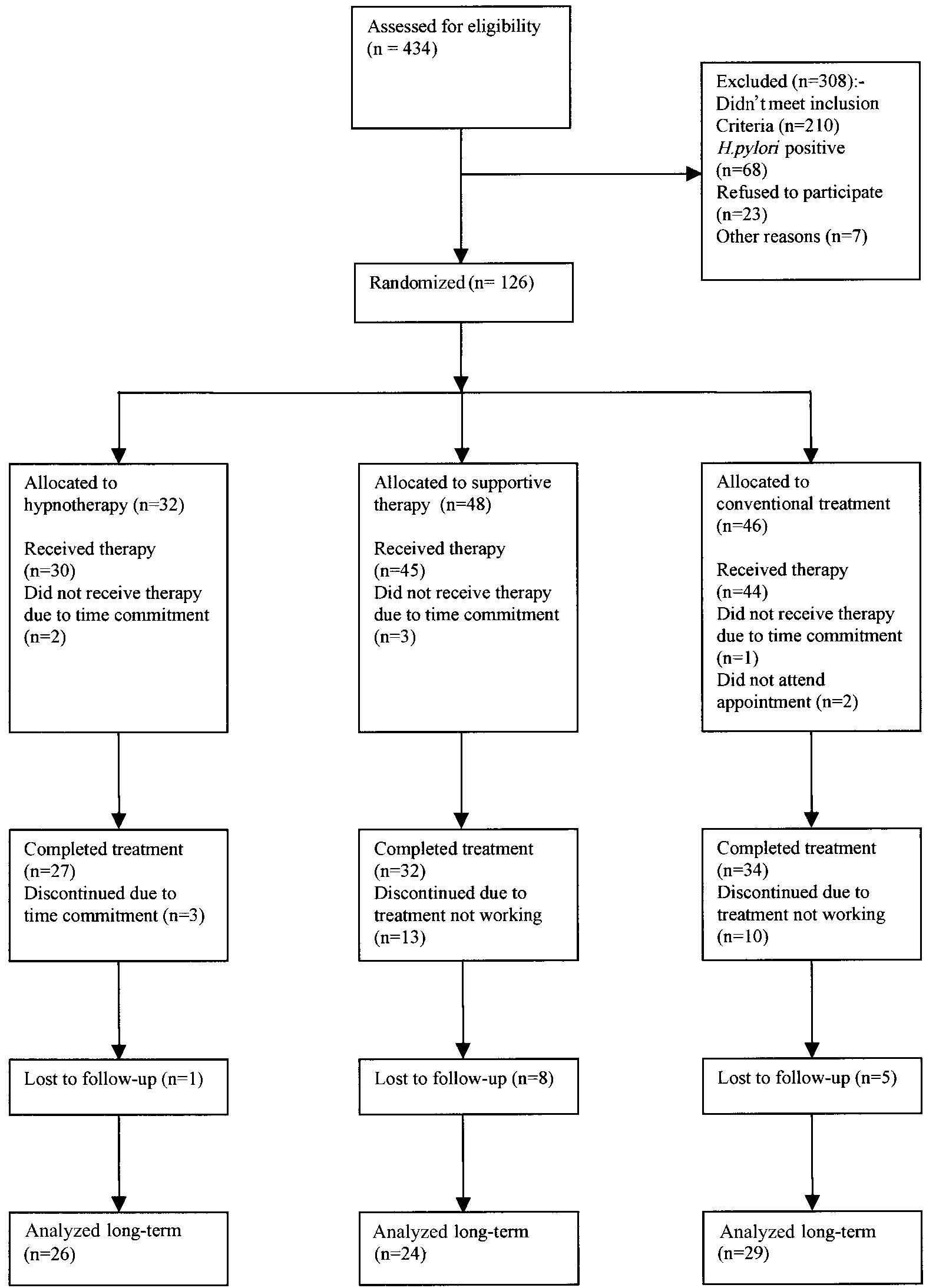 Figure 2. Study flow diagram.
Figure 2. Study flow diagram.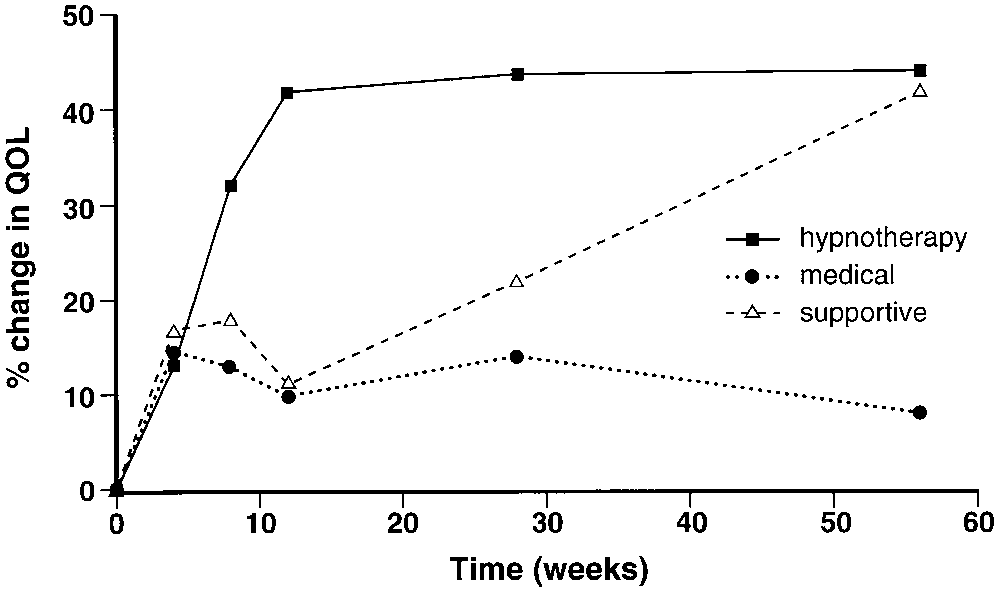
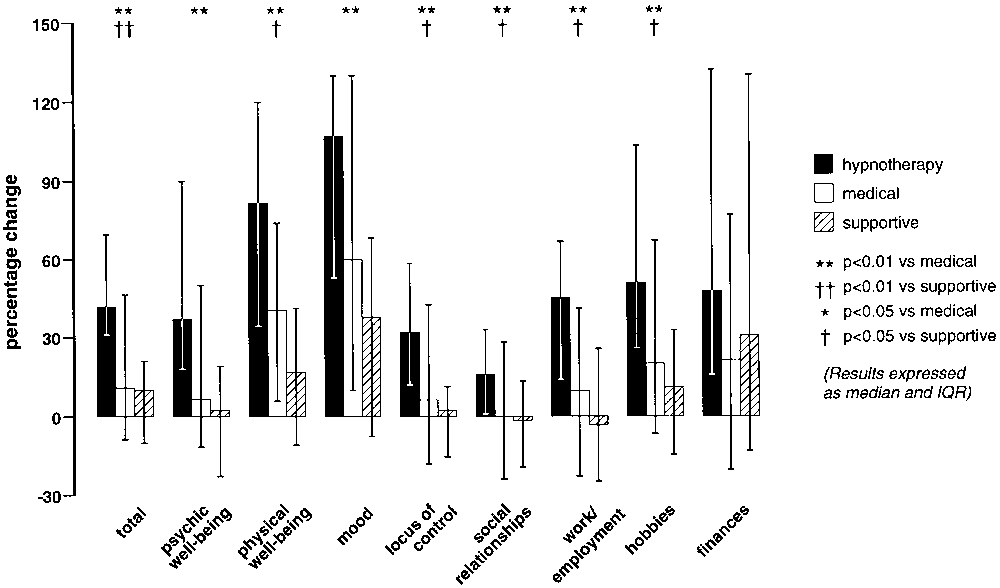
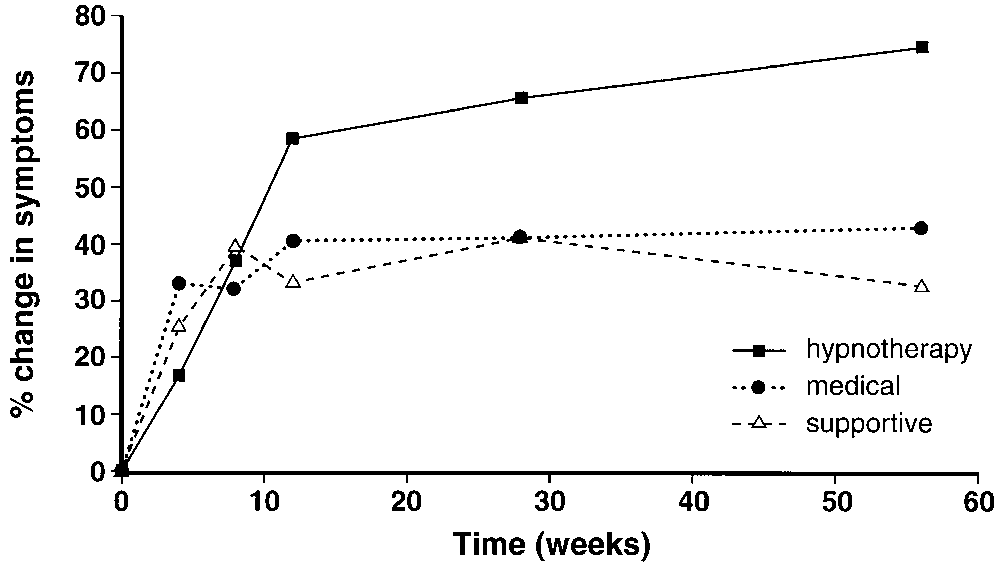
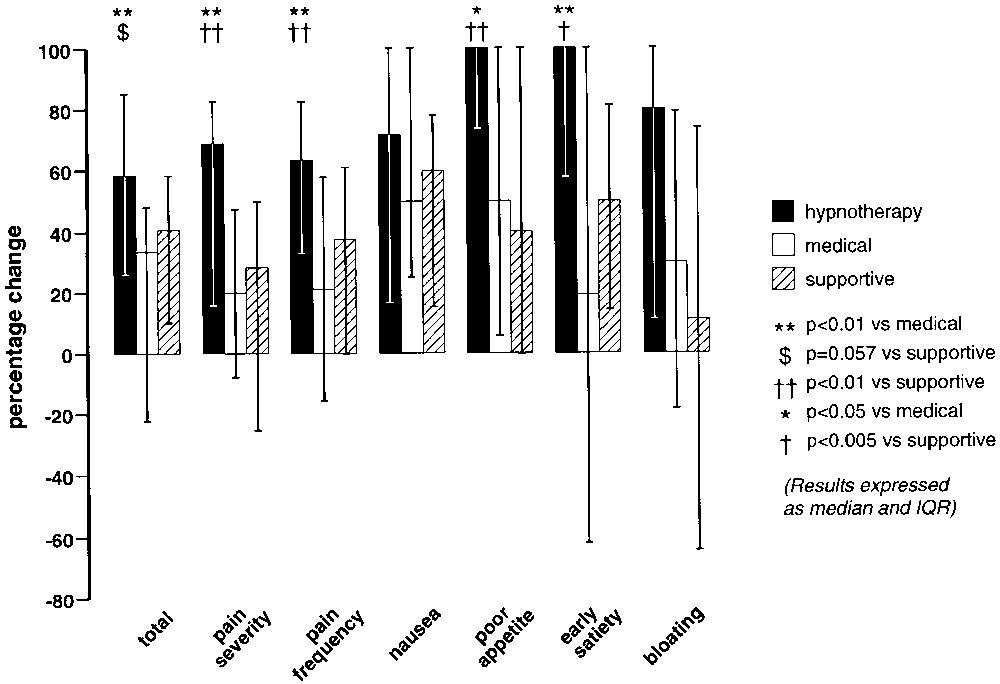 Figure 3. Symptom change throughout the study. Reprinted with
Figure 5. QOL change throughout the study. Reprinted with permis-
permission from Department of Medical Illustration, Withington Hos-
sion from Department of Medical Illustration, Withington Hospital,
improved by HT [42% (31%– 69%)] compared with
supportive, 3.6 (2.8 – 4.7); medical, 3.6 (2.5– 4.5); total
both the medical [11% (Ϫ9%– 46.6%) P Ͻ 0.001] and
QOL score: HT, 5.1 (4.6 – 6.5); supportive, 5.1 (4.7–
supportive [10% (Ϫ10%–21.2%); P Ͻ 0.001] groups.
Figure 3. Symptom change throughout the study. Reprinted with
Figure 5. QOL change throughout the study. Reprinted with permis-
permission from Department of Medical Illustration, Withington Hos-
sion from Department of Medical Illustration, Withington Hospital,
improved by HT [42% (31%– 69%)] compared with
supportive, 3.6 (2.8 – 4.7); medical, 3.6 (2.5– 4.5); total
both the medical [11% (Ϫ9%– 46.6%) P Ͻ 0.001] and
QOL score: HT, 5.1 (4.6 – 6.5); supportive, 5.1 (4.7–
supportive [10% (Ϫ10%–21.2%); P Ͻ 0.001] groups.