He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
091197 a controlled trial of two nucleoside analogues
C o py r ig h t , 1 9 9 7, by t h e Ma s s a c h u s e t t s Me d i c a l S o c i e t y
V O L U M E 3 3 7 N U M B E R 1 1
A CONTROLLED TRIAL OF TWO NUCLEOSIDE ANALOGUES PLUS INDINAVIR
IN PERSONS WITH HUMAN IMMUNODEFICIENCY VIRUS INFECTION
AND CD4 CELL COUNTS OF 200 PER CUBIC MILLIMETER OR LESS
SCOTT M. HAMMER, M.D., KATHLEEN E. SQUIRES, M.D., MICHAEL D. HUGHES, PH.D., JANET M. GRIMES, M.S.,
LISA M. DEMETER, M.D., JUDITH S. CURRIER, M.D., JOSEPH J. ERON, JR., M.D., JUDITH E. FEINBERG, M.D.,
HENRY H. BALFOUR, JR., M.D., LAWRENCE R. DEYTON, M.D., JEFFREY A. CHODAKEWITZ, M.D.,
AND MARGARET A. FISCHL, M.D., FOR THE AIDS CLINICAL TRIALS GROUP 320 STUDY TEAM*
ABSTRACT
ROGRESS in the field of antiretroviral ther-
apy for human immunodeficiency virus type
protease inhibitor to two nucleoside analogues to
1 (HIV-1) infection has brought the end of
treat human immunodeficiency virus type 1 (HIV-1)
the zidovudine-monotherapy era,1-3 an im-
infection are not clear. We compared treatment with
proved understanding of the pathogenesis of HIV-1
the protease inhibitor indinavir in addition to zidovu-
disease,4-9 demonstrations of the prognostic impor-
dine and lamivudine with treatment with the two nu-
tance of plasma HIV-1 RNA quantification,10-17 and
cleosides alone in HIV-infected adults previously treat-
the availability of increasingly potent therapeutic
agents. Much of this progress is linked to the intro-
duction of the HIV-protease inhibitors, drugs that
treated with lamivudine or protease inhibitors werestratified according to CD4 cell count (50 or fewer vs.
inhibit the processing of Gag and Gag–Pol polypro-
51 to 200 cells per cubic millimeter) and randomly
tein precursors and thus prevent the maturation of
assigned to one of two daily regimens: 600 mg of zi-
virions.18-20 Trials of HIV-protease inhibitors have
dovudine and 300 mg of lamivudine, or that regimen
shown beneficial effects on CD4 cell counts and plas-
with 2400 mg of indinavir. Stavudine could be sub-
ma HIV-1 RNA concentrations to a degree not pre-
stituted for zidovudine. The primary end point was
viously described with approved reverse-transcriptase
the time to the development of the acquired immu-
inhibitors.21-26 The most notable findings have in-
volved three-drug combinations that include a po-
tent HIV-protease inhibitor and two nucleoside an-
progressed to AIDS or death was lower with indina-vir, zidovudine (or stavudine), and lamivudine (6 per-cent) than with zidovudine (or stavudine) and lami-vudine alone (11 percent; estimated hazard ratio,0.50; 95 percent confidence interval, 0.33 to 0.76;
From Harvard Medical School, Boston (S.M.H.); the University of Ala-
Pϭ0.001). Mortality in the two groups was 1.4 per-
bama at Birmingham, Birmingham (K.E.S.); the London School of Hy-
cent and 3.1 percent, respectively (estimated hazard
giene and Tropical Medicine, London (M.D.H.); Harvard School of Public
ratio, 0.43; 95 percent confidence interval, 0.19 to
Health, Boston (M.D.H., J.M.G.); the University of Rochester, Rochester,
0.99; Pϭ0.04). The effects of treatment were similar
N.Y. (L.M.D.); the University of Southern California, Los Angeles (J.S.C.);the University of North Carolina, Chapel Hill (J.J.E.); the University of
in both CD4 cell strata. The responses of CD4 cells
Cincinnati, Cincinnati (J.E.F.); the University of Minnesota, Minneapolis
and plasma HIV-1 RNA paralleled the clinical results.
(H.H.B.); the Division of AIDS, National Institute of Allergy and Infec-
tious Diseases, Bethesda, Md. (L.R.D.); Merck and Co., West Point, Pa. (J.A.C.); and the University of Miami, Miami (M.A.F.). Address reprint re-
and lamivudine as compared with zidovudine and
quests to Dr. Hammer at the Division of Infectious Diseases, Beth Israel
lamivudine alone significantly slows the progression
Deaconess Medical Center, 1 Deaconess Rd., Boston, MA 02215.
of HIV-1 disease in patients with 200 CD4 cells or
Other authors were John P. Phair, M.D. (Northwestern University), Wil-
fewer per cubic millimeter and prior exposure to zi-
liam Spreen, Pharm.D. (Glaxo–Wellcome), Louise Pedneault, M.D. (Bris-tol-Myers Squibb), Bach-Yen Nguyen, M.D. (Merck), and Jon C. Cook,
dovudine. (N Engl J Med 1997;337:725-33.)
B.Sc. (AIDS Clinical Trials Group Operations Center).
1997, Massachusetts Medical Society.
*The institutions and investigators participating in the AIDS Clinical
Trials Group 320 Study are listed in the Appendix.
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
alogues. Specifically, when patients previously ex-
phylaxis for other opportunistic infections was permitted, al-
posed to zidovudine who had either 50 to 400 or
though the use of rifabutin was prohibited.
50 or fewer CD4 cells per cubic millimeter were
Patients who had verified AIDS-defining events were offered
open-label indinavir therapy with the approval of the study chairs
treated with indinavir, zidovudine, and lamivudine,
and without having their initial treatment assignments revealed.
plasma HIV-1 RNA concentrations were suppressed
All potential AIDS-defining events were reviewed in a blinded
to less than 500 copies per milliliter in 85 percent
fashion by the study chair; only those that met the criteria defined
and 65 percent of patients, respectively.24,25 These
in the study protocol were included in the analysis.
findings have raised the important question of the
Monitoring and Enrollment
clinical efficacy and safety of a three-drug regimen
The patients were followed at weeks 4, 8, and 16 and every
containing indinavir. We addressed that issue in this
eight weeks thereafter with a clinical assessment and routine lab-
oratory monitoring. CD4 cell counts were determined twice atbase line and at weeks 4, 8, 24, and 40. Enrollment began in Jan-
uary 1996. The study was reviewed twice by a data and safetymonitoring board. At the second such review, on February 18,
Study Design and Patients
1997, the comparison of the groups based on data on the patients
The AIDS Clinical Trials Group 320 Study was a randomized,
randomized by January 27, 1997, showed a significant difference
double-blind, placebo-controlled trial that compared the three-
between groups that met the prespecified guideline for stopping
drug regimen of indinavir (Crixivan), open-label zidovudine
the study. At that time, the board recommended that the accru-
(Retrovir) or stavudine (Zerit), and lamivudine (Epivir) with the
al of patients be terminated and the study closed.
two-drug regimen of zidovudine (or stavudine) and lamivudine
Plasma HIV-1 RNA concentrations were determined retro-
in HIV-infected patients who had no more than 200 CD4 cells
spectively in appropriately stored specimens from 190 randomly
per cubic millimeter and at least three months of prior zidovudine
selected patients. These concentrations were measured twice at
therapy. The randomization was stratified according to the CD4
base line and at weeks 4, 8, 24, and 40 (Roche Amplicor HIV-1
cell count obtained at the time of screening (50 or fewer cells per
cubic millimeter as compared with 51 to 200 cells per cubic mil-limeter). The study was designed to enroll 1750 patients, with 40
Statistical Analysis
percent of them in the stratum with 50 or fewer CD4 cells per
The times to events were compared between treatment groups
cubic millimeter. The primary outcome measure in the assess-
by Kaplan–Meier estimates, log-rank tests, and proportional-haz-
ment of efficacy was the development of a new acquired immu-
ards models stratified according to the CD4 cell count obtained
nodeficiency syndrome (AIDS)–defining event (except when the
at the time of screening (50 or fewer vs. 51 to 200 cells per cubic
AIDS-defining event was the development of Pneumocystis carinii
millimeter).30 Changes in CD4 cell counts over time were com-
pneumonia, in which case both new and recurrent events were ac-
pared in a mixed-effects regression model.31 An analysis of covar-
cepted as outcome measures) or death; in the assessment of safe-
iance adjusted for the screening CD4 cell count and the AIDS
ty, the outcome measure was the occurrence of adverse events
Clinical Trials Unit was used to compare changes in the CD4 cell
(signs, symptoms, or laboratory abnormalities) defined as severe
count and the HIV-1 RNA concentration at each measurement.32
or worse according to the grading scheme of the AIDS Clinical
With regard to changes in HIV-1 RNA, this calculation used a
Trials Group.27 The secondary outcome measures studied were
regression for censored data: concentrations below the limit of
death and changes in CD4 cell counts and plasma HIV-1 RNA
quantification, 500 copies per milliliter, were censored.33 Analyses
of all the variables pertaining to efficacy were performed on an
The patients, recruited from 33 AIDS Clinical Trials Units and
intention-to-treat basis that included data on all patients random-
7 National Hemophilia Foundation sites in the United States and
ized and all available follow-up data (including that obtained after
Puerto Rico (see the Appendix), had to be more than 16 years
the discontinuation of the study treatment). In the analyses of ad-
old and had to have laboratory documentation of HIV-1 infec-
verse events, the treatments were compared by a chi-square test;
tion, a CD4 cell count of 200 per cubic millimeter or less within
the follow-up data were censored either when a patient began re-
the 60 days before entry into the study, at least 3 months of prior
ceiving open-label indinavir or 56 days after the permanent dis-
zidovudine treatment, no more than 1 week of prior lamivudine
continuation of the study treatment, whichever came first, and
treatment, no prior treatment with protease inhibitors, a Karnof-
were restricted to patients for whom the study treatment was dis-
sky performance score of at least 70, and acceptable laboratory
pensed. All reported P values are two-sided. P values, estimates of
values. The study was approved by the institutional review boards
differences between treatments, and 95 percent confidence inter-
of the participating institutions, and all the patients gave written
vals are unadjusted for the repeated interim analyses.
The patients received open-label zidovudine (200 mg three
times daily) and lamivudine (150 mg two times daily) and wererandomly assigned to receive indinavir (800 mg) or matching pla-
Accrual and Characteristics of the Patients
cebo every eight hours. In the first version of the protocol, onlypatients who could tolerate zidovudine and who had had at least
There were 1156 patients randomized between
6 months of prior zidovudine therapy were enrolled, and the sub-
January 29, 1996, and January 27, 1997. Of these,
stitution of stavudine for zidovudine was permitted in the event
439 (38 percent) had 50 CD4 cells or fewer per cu-
of drug-associated toxicity at any point after randomization or if
bic millimeter and 717 (62 percent) had 51 to 200
clinical progression of HIV-1 disease occurred that did not fulfill
CD4 cells per cubic millimeter. The base-line char-
the criteria for a protocol-defined AIDS event at or beyond 24weeks of study. The dose of stavudine was 40 mg two times daily
acteristics of the study patients (Table 1) were well
(or 30 mg two times daily for patients weighing less than 60 kg).
A protocol modification in October 1996 reduced the requiredprior exposure to zidovudine to at least three months and permit-
Duration of Follow-up and Study Treatment
ted patients who could not tolerate zidovudine to enter the studywith stavudine substituted for zidovudine at the time of random-
The median duration of follow-up was 38 weeks.
ization. Prophylaxis for P. carinii pneumonia was mandated. Pro-
Five percent of the patients were lost to follow-up;
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T WO N U C L E O S I D E A N A LO G U E S P LU S I N D I N AV I R I N P E R S O N S W I T H H I V I N F E C T I O N TABLE 1. BASE-LINE CHARACTERISTICS OF THE PATIENTS ACCORDING TO
CD4 CELL COUNT AT THE TIME OF SCREENING.*
ALL PATIENTS CHARACTERISTIC (N؍1156) CD4 COUNT PER CUBIC MILLIMETER
alone or in combination — median (25th, 75th percentile)
*Plus–minus values are means ϮSD. Because of rounding, not all columns total 100 percent. †Values shown are the means of two measurements obtained at least one day apart. Values obtained
at screening, which had to be р200 cells per cubic millimeter, were not included in this calculation.
‡HIV-1 RNA was measured in a randomly selected cohort of 190 patients (75 patients with 50
CD4 cells or fewer per cubic millimeter and 115 patients with 51 to 200 CD4 cells per cubic milli-meter).
the duration of follow-up and the percentage of pa-
tration (on the basis of determinations made outside
tients lost to follow-up were similar in both treat-
ment groups and both CD4-cell strata.
Ten patients did not have any study treatment. Of
Progression of Disease
the remaining 1146 patients, 227 (20 percent) dis-
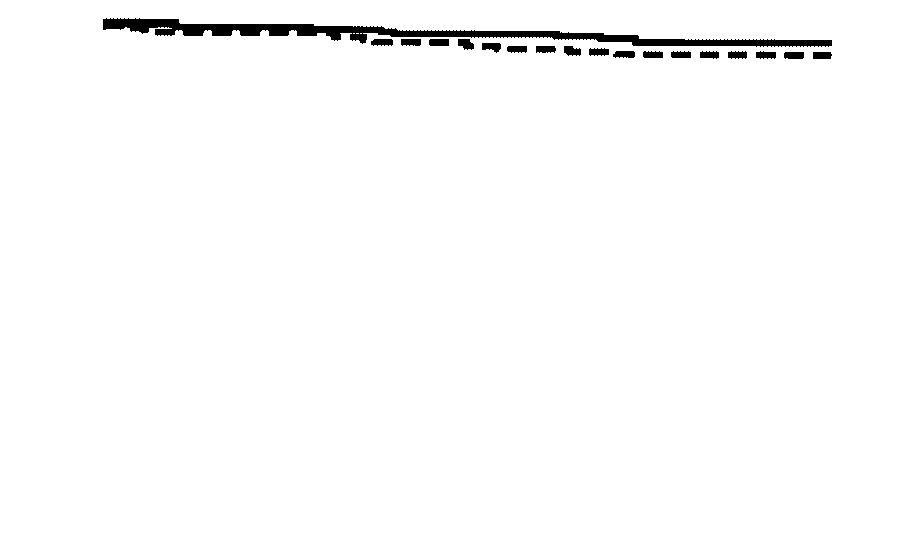
Ninety-six patients (8 percent) had AIDS-defining
continued the study treatment prematurely, more
events or died (Table 2). Sixty-three patients (11
than seven days before reaching a study end point.
percent) assigned to zidovudine (or stavudine) and
The proportion who discontinued the study treat-
lamivudine had disease progression, as compared
ment was higher in the group receiving zidovudine
with 33 patients (6 percent) assigned to indinavir, zi-
(or stavudine) and lamivudine (28 percent) than in
dovudine (or stavudine), and lamivudine (Pϭ0.001;
the group receiving indinavir, zidovudine (or stavu-
estimated hazard ratio, 0.50; 95 percent confidence
dine), and lamivudine (12 percent, PϽ0.001). In
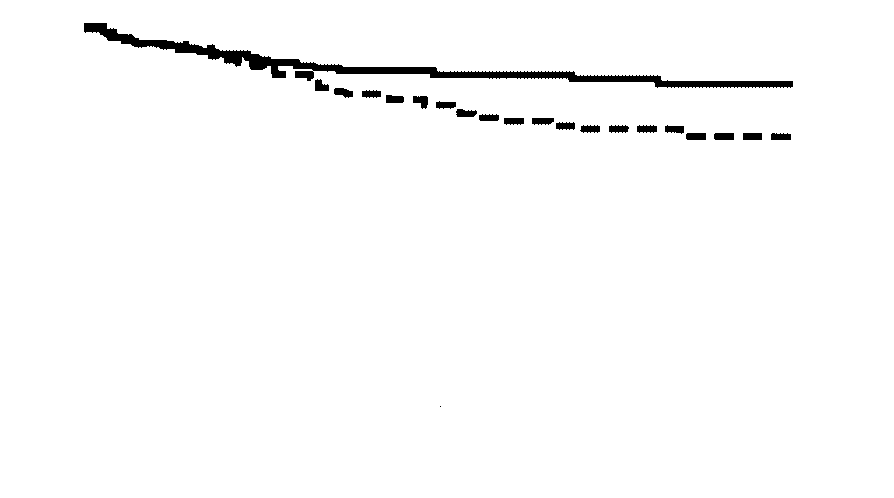
interval, 0.33 to 0.76) (Fig. 1A). There was no sig-
the stratum with 50 CD4 cells or fewer per cubic
nificant difference in the relative effects of the two
millimeter, the proportions of patients discontinuing
treatments between the patients with 50 CD4 cells
the study treatment in the two groups were 32 per-
or fewer per cubic millimeter and the patients with
cent and 16 percent, respectively (PϽ0.001), and
51 to 200 CD4 cells per cubic millimeter. Forty-four
in the stratum with 51 to 200 CD4 cells per cubic
patients in the former stratum (20 percent) had
millimeter, these proportions were 26 percent and
AIDS-defining events or died in the group assigned
9 percent (PϽ0.001). Only 4 percent of patients
to zidovudine (or stavudine) and lamivudine, as
(10 of 227) discontinued the study treatment pre-
compared with 23 patients (11 percent) in the
maturely because of protocol-defined adverse events:
group assigned to indinavir, zidovudine (or stavu-
4 patients assigned to zidovudine (or stavudine) and
dine), and lamivudine (Pϭ0.005; estimated hazard
lamivudine and 6 patients assigned to indinavir, zi-
ratio, 0.49; 95 percent confidence interval, 0.30 to
dovudine (or stavudine), and lamivudine. Among the
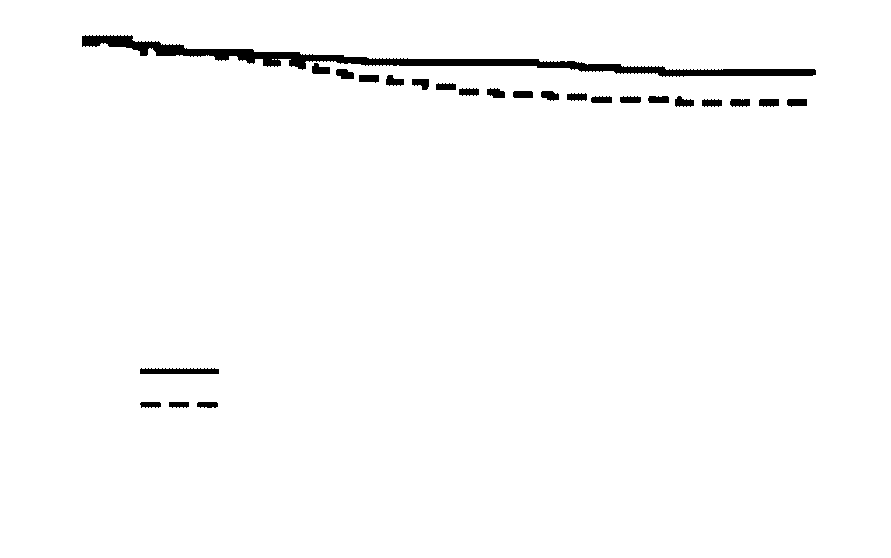
0.82) (Fig. 1B). In the stratum with 51 to 200 CD4
premature discontinuations, 52 percent (117 of 227)
cells per cubic millimeter, 19 patients (5 percent)
were initiated by the patients, and for approximately
had AIDS-defining events or died in the group as-
half these patients the reasons given included a de-
signed to zidovudine (or stavudine) and lamivudine,
sire to seek open-label therapy with protease inhibi-
as compared with 10 patients (3 percent) in the
tors, concern about the plasma HIV-1 RNA concen-
group assigned to indinavir, zidovudine (or stavu-
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
TABLE 2. RATES OF DISEASE PROGRESSION ACCORDING TO CD4 CELL COUNT INDINAVIR, ZIDOVUDINE ZIDOVUDINE HAZARD RATIO (OR STAVUDINE), (OR STAVUDINE) (95% CONFIDENCE VARIABLE AND LAMIVUDINE AND LAMIVUDINE INTERVAL)* P VALUE†
*The reference group is the group receiving zidovudine (or stavudine) and lamivudine.
†Values were calculated by the log-rank test.
dine), and lamivudine (Pϭ0.08; estimated hazard
pared with 31 among the patients assigned to indin-
ratio, 0.51; 95 percent confidence interval, 0.24 to
avir, zidovudine (or stavudine), and lamivudine. The
most common events were infections with P. carinii,
Overall, 26 patients died (2.2 percent) (Table 2).
cytomegalovirus, and Mycobacterium avium com-
Eighteen patients (3.1 percent) died in the group as-
plex (constituting 25 percent, 20 percent, and 16
signed to zidovudine (or stavudine) and lamivudine,
as compared with eight (1.4 percent) in the groupassigned to indinavir, zidovudine (or stavudine), and
Changes in CD4 Cell Counts
lamivudine (Pϭ0.04; estimated hazard ratio, 0.43;
Increased CD4 cell counts that persisted above
95 percent confidence interval, 0.19 to 0.99). There
base-line values were seen in both treatment groups,
was no significant difference in the relative effects of
with superior responses in the group receiving indin-
the two treatments between the two strata. Among
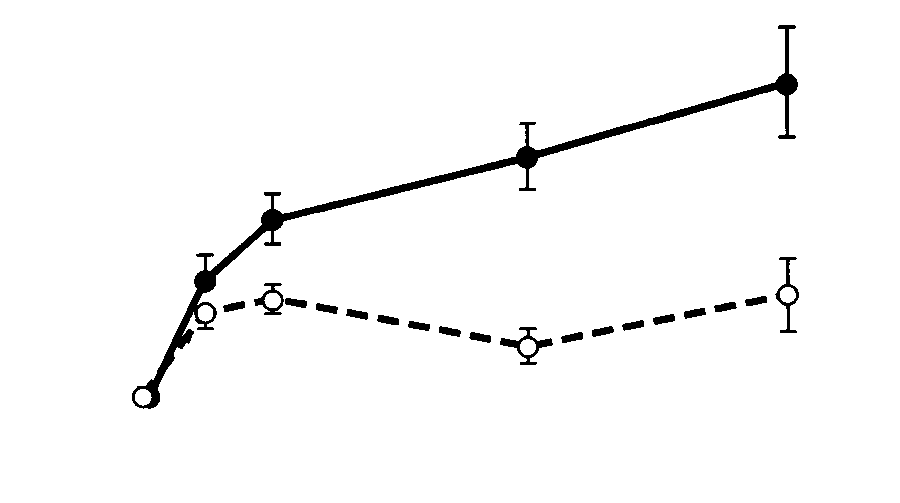
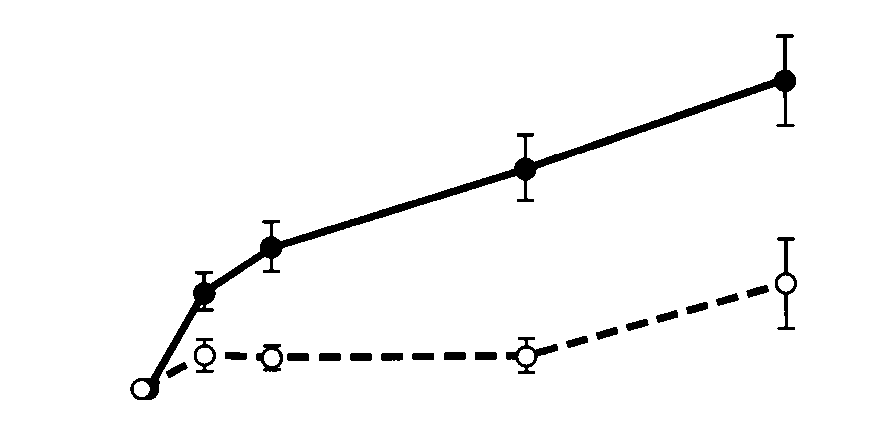
avir. At weeks 4, 8, 24, and 40, the mean CD4 cell
the patients with 50 CD4 cells or fewer per cubic
count in the patients assigned to zidovudine (or stav-
millimeter, 13 patients receiving only the two nucle-
udine) and lamivudine increased by 27, 30, 18, and
oside analogues died (5.9 percent), as compared
40 cells per cubic millimeter, respectively. The corre-
with 5 patients receiving all three drugs (2.3 percent;
sponding mean increases in the patients assigned to
Pϭ0.05; estimated hazard ratio, 0.37; 95 percent
indinavir, zidovudine (or stavudine), and lamivudine
confidence interval, 0.13 to 1.04). Among the pa-
were 46, 65, 91, and 121 cells per cubic millimeter
tients with 51 to 200 CD4 cells per cubic millimeter,
(Fig. 2A). Thus, the change at week 4 was greater by
five patients assigned to zidovudine (or stavudine)
19 cells per cubic millimeter (PϽ0.001) in the group
and lamivudine (1.4 percent) died, as compared with
that received indinavir, and the difference increased
three patients assigned to indinavir, zidovudine (or
with time (PϽ0.001), to 36, 73, and 82 cells per cu-
stavudine), and lamivudine (0.8 percent).
bic millimeter at weeks 8, 24, and 40, respectively.
A total of 109 of the 1156 patients (9.4 percent)
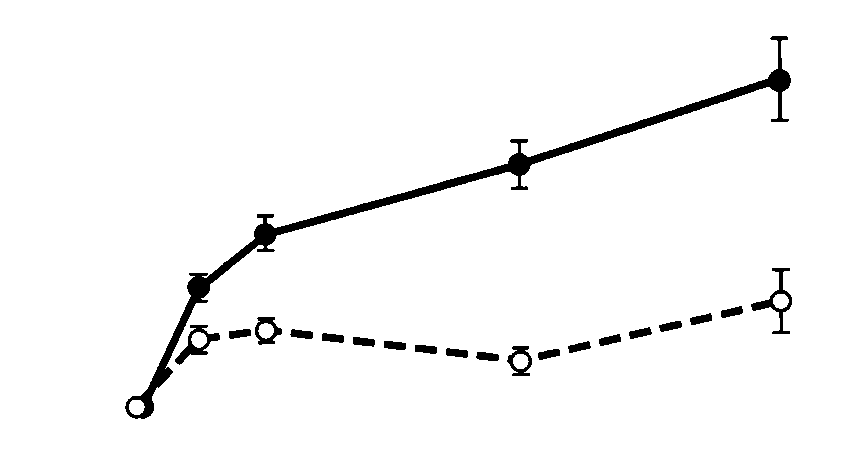
The responses of the CD4 cell count to treatment
were treated with stavudine instead of zidovudine
are shown in Figures 2B and 2C. In the group re-
before the development of an AIDS-defining event
ceiving zidovudine (or stavudine) and lamivudine,
or death. None of the three patients who were ini-
the early increases from base line — those at weeks
tially assigned to stavudine had a protocol-defined
4 and 8 — were smaller in the stratum with 50 CD4
end point. Among the 106 patients in whom stavu-
cells or fewer per cubic millimeter than in the stra-
dine was substituted for zidovudine after random-
tum with 51 to 200 CD4 cells per cubic millimeter.
ization, 3 (all in the two-nucleoside group) had
However, the changes from base line in the longer
AIDS-defining events, and none died.
term — those at weeks 24 and 40 — were similar inthe two strata. Exploratory analyses of the CD4 cell
AIDS-Defining Events
counts in the two treatment groups when the data
In all, there were 91 AIDS-defining events (in-
were censored at the times patients changed from
cluding multiple events per patient). Sixty of these
the treatment to which they were initially assigned
occurred among the patients assigned to receive zi-
showed increases from base line that were similar to
dovudine (or stavudine) and lamivudine, as com-
those in the intention-to-treat analyses at weeks 4,
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T WO N U C L E O S I D E A N A LO G U E S P LU S I N D I N AV I R I N P E R S O N S W I T H H I V I N F E C T I O N
Patients with р50 CD4 Cells/mm3 (Nϭ439)
Patients with 51–200 CD4 Cells/mm3 (Nϭ717)
Figure 2. Mean Changes from Base Line in the CD4 Cell Count.
The number of patients who could be evaluated at each time
point is shown. Bars indicate 95 percent confidence intervals. Figure 1. Kaplan–Meier Estimates of the Proportion of Patients Who Did Not Reach the Primary Study End Point of AIDS or Death.
8, and 24 (data not shown). At week 40, the differ-
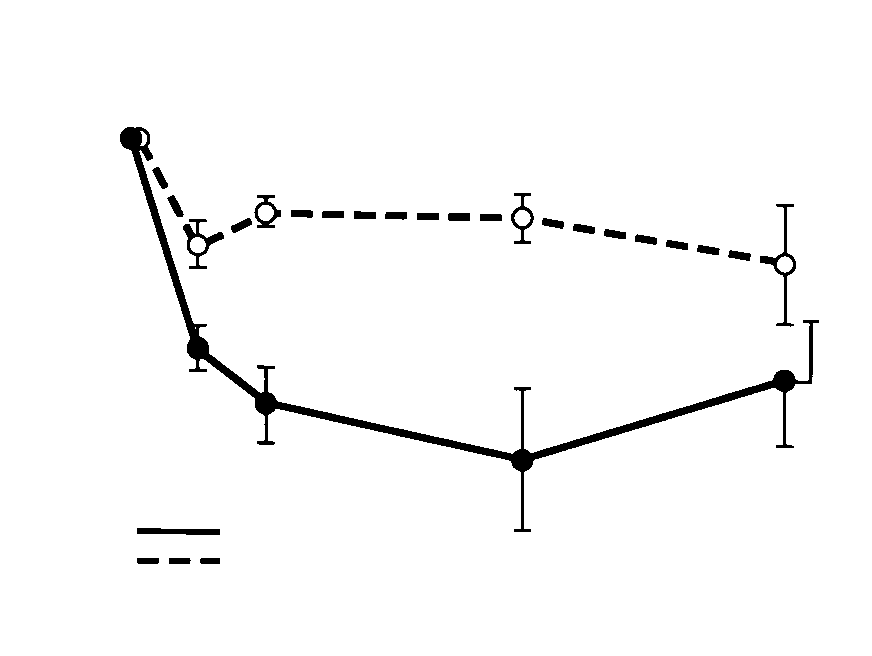
Changes in Plasma HIV-1 RNA Concentrations
ence between the two treatment groups was smaller
The responses of the plasma HIV-1 RNA concen-
in the intention-to-treat analysis than in the cen-
trations to treatment were studied in 190 randomly
sored analysis (difference in mean change, 82 vs. 115
selected patients. There were persistent decreases
cells per cubic millimeter), suggesting that the dif-
from the base-line values in both treatment groups,
ference may have been reduced by the greater pro-
with significantly better responses in the group
portion of subjects who changed treatment in the
whose treatment included indinavir (PϽ0.001 in an
group receiving zidovudine (or stavudine) and lami-
area-under-the-curve analysis). At weeks 4, 8, 24,
and 40, the mean decreases in plasma HIV-1 RNA
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
in the group receiving zidovudine (or stavudine) and
lamivudine were 0.9, 0.6, 0.6, and 1.0 log copies
per milliliter, respectively. The corresponding de-creases in the group receiving indinavir, zidovudine
(or stavudine), and lamivudine were 1.8, 2.3, 2.8,
and 2.1 log copies per milliliter (Fig. 3A). The
changes from base line were significantly greater at
each time point in the group treated with indinavir(PϽ0.001 at weeks 4, 8, and 24; Pϭ0.007 at week
40). At week 24, the proportion of patients with
plasma HIV-1 RNA concentrations of less than 500copies per milliliter was 9 percent in the two-nucle-
oside group, as compared with 60 percent in the
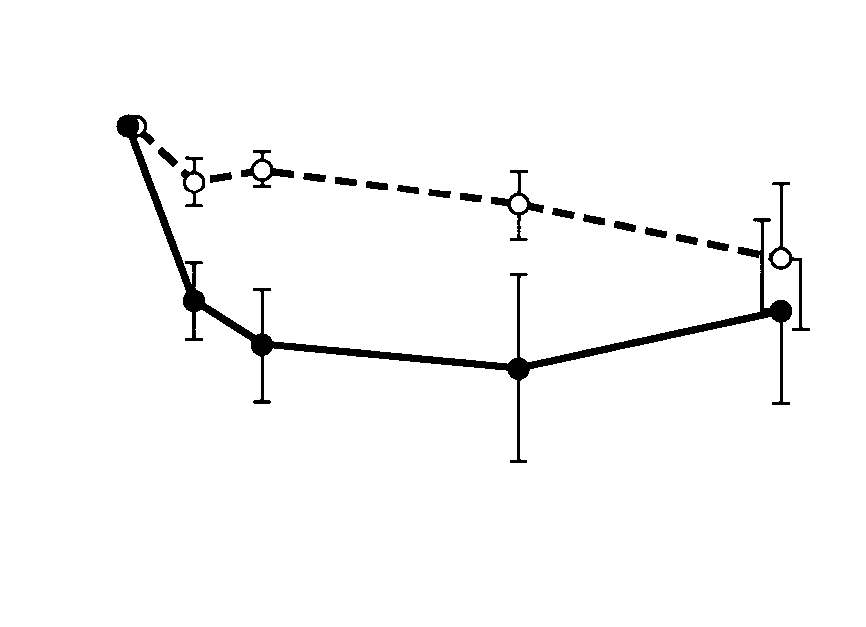
The plasma HIV-1 RNA responses according to
the CD4 cell count are shown in Figures 3B and 3C. In the patients with 50 CD4 cells or fewer per cubicmillimeter, the decreases in plasma HIV-1 RNA ap-
peared to be smaller than those in the patients with51 to 200 CD4 cells per cubic millimeter. However,
conclusions about stratum-specific plasma HIV-1
RNA responses need to be made cautiously because
of the small numbers of patients followed throughweek 40. Adverse Events
The proportion of patients with signs and symp-
toms that were severe (grade 3) or worse (grade 4)
in the group receiving zidovudine (or stavudine) and
lamivudine was 18 percent, as compared with 21percent in the group receiving indinavir, zidovudine
(or stavudine), and lamivudine (Pϭ0.17). The mostcommon symptoms were nonspecific discomfort,malaise, fever, headache, and nausea and vomiting,
with no difference in the reporting of symptoms be-tween treatment groups.
The proportion of patients with severe laboratory
abnormalities or worse in the group receiving zido-
vudine (or stavudine) and lamivudine was 26 per-
cent, as compared with 21 percent in the group
receiving indinavir, zidovudine (or stavudine), andlamivudine (Pϭ0.06). This difference primarily re-
flected a difference between the groups in the inci-
dence of neutropenia (15 percent and 5 percent, re-spectively; PϽ0.001). In contrast, the proportion of
patients with hyperbilirubinemia was 1 percent in
the two-nucleoside group, as compared with 6 per-
cent in the group treated with indinavir (PϽ0.001),a finding compatible with the known elevation of in-
direct bilirubin associated with the use of indinavir.
Two percent of the patients in each treatment grouphad hyperglycemia. Figure 3. Mean Change from Base Line in the Plasma HIV-1
Five patients receiving zidovudine (or stavudine)
and lamivudine (1 percent) had episodes of renal
For this analysis, 190 patients were randomly selected andtheir HIV-1 RNA concentrations were studied. The number of
colic or nephrolithiasis (irrespective of grade), as
patients who could be evaluated at each time point is shown.
compared with 21 patients receiving indinavir, zido-
Bars indicate 95 percent confidence intervals.
vudine (or stavudine), and lamivudine (4 percent,Pϭ0.001). Three of the five patients in the two-
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T WO N U C L E O S I D E A N A LO G U E S P LU S I N D I N AV I R I N P E R S O N S W I T H H I V I N F E C T I O N
nucleoside group in whom renal colic or nephro-
nied by greater suppression of HIV-1 RNA expres-
lithiasis developed had that condition after discon-
sion in lymphoid tissue35 and may prevent the emer-
tinuing the study treatment and starting open-label
gence of resistance — factors that may add to the
clinical benefit now established for this regimen.
Five new diagnoses of diabetes mellitus were re-
Our study also found superior responses of CD4
corded: two in the two-nucleoside group and three
cells and plasma HIV-1 RNA with the three-drug
in the group treated with indinavir.
We chose the combination of zidovudine and la-
mivudine as the control treatment because of the
This study showed the clinical superiority of the
unique interactions between these two agents with
three-drug regimen containing indinavir over the
respect to mutations conferring resistance, the re-
two-nucleoside combination in patients previously
sults of phase 2 trials, the tolerance associated with
treated with zidovudine who had CD4 cell counts
the regimen, and its widespread use in clinical prac-
of 200 per cubic millimeter or less. The proportion
tice.36-40 The clinical benefit of lamivudine when that
of patients whose disease progressed to AIDS or
drug is added to previously available nucleoside an-
death was reduced from 11 percent to 6 percent by
alogues to treat patients with 25 to 250 CD4 cells
the three-drug combination, a 50 percent reduction
per cubic millimeter was recently confirmed in the
(Pϭ0.001). The hazard ratios in the study patients
CAESAR trial, in which the risk of AIDS or death
as a whole (0.50), those with CD4 cell counts of 50
was reduced by approximately 50 percent.41 In the
per cubic millimeter or less (0.49), and those with
control group in our study, there was a relatively low
counts of 51 to 200 per cubic millimeter (0.51)
rate of disease progression, as well as a moderate
were very similar, suggesting that the effect of treat-
increase in the CD4 cell count and a decline in plas-
ment was similar across the study population, al-
ma HIV-1 RNA; these persisted throughout the
though the possibility of differential effects cannot
study, even though it is now recognized that simply
be ruled out. Mortality, low in both groups, was re-
adding lamivudine to a preexisting regimen is not a
duced from 3.1 percent to 1.4 percent with the
standard clinical approach. The strength of the con-
three-drug regimen (Pϭ0.04). Thus, there was evi-
trol group in this study is also an important differ-
dence of a reduction in mortality that was consistent
ence between this study and previously reported
with the reduced risk of progression to the primary
studies of other HIV-protease inhibitors that have
assessed clinical end points.42,43 In the Abbott M94-
The rate of loss to follow-up in this study was low
247 trial, ritonavir or placebo was added to stable
(5 percent), and the overall rate of premature dis-
prior nucleoside-analogue therapy or no therapy.42
continuation of treatment was moderate (20 per-
In the Hoffmann–La Roche NV14256 trial, a regi-
cent). Seventy-nine percent of the 96 AIDS-defining
men of saquinavir plus zalcitabine was compared with
events or deaths occurred while the patients were re-
zalcitabine monotherapy.43 In the context of these
ceiving the study treatment or within seven days of
other trials, our study makes it clear that more po-
its discontinuation. Although rates of withdrawal from
tent therapies, now represented by three-drug regi-
treatment differed between the two study groups, the
mens containing a protease inhibitor, are preferable
tendency for patients who withdrew prematurely
in patients with advanced disease. The durability of
from the two-nucleoside group to seek treatment
the clinical benefit conferred by indinavir as part of
with protease inhibitors would tend to narrow the
a three-drug regimen has not been fully defined,
differences between the groups in rates of disease
progression and therefore should not affect the con-
Improving the use of the currently approved agents
clusions of the study. Conversely, when a study is ter-
to treat HIV-1 infection, and the promising drugs
minated early because a stopping guideline is used,
on the clinical horizon,44-46 in the management of
differences between the treatment groups tend to be
HIV-1 disease remains a challenge.47 However, this
overestimated because of random variation.34 How-
study supports the view that employing well-tolerat-
ever, it is impossible to determine the relative mag-
ed regimens of increasing potency will translate into
greater clinical benefits for patients with HIV-1 in-
These findings confirm on the basis of clinical end
points the results of earlier trials of the combinationof indinavir, zidovudine, and lamivudine in patients
Supported in part by the AIDS Clinical Trials Group, National Institute
previously treated with zidovudine, trials that showed
of Allergy and Infectious Diseases; by the General Clinical Research Center
that the three-drug combination produces superior
units funded by the National Center for Research Resources; and by Merckand Co. (for institutions enrolling more than 30 patients).
responses in plasma HIV-1 RNA concentrations and
Drs. Hammer, Squires, Hughes, Demeter, Currier, Eron, Feinberg, Bal-
CD4 cell counts.24,25 The suppression of plasma
four, Fischl, and Phair have served as ad hoc consultants for, or received
HIV-1 RNA to unquantifiable levels in the majority
honorariums or research grants from, one or more of the pharmaceuticalfirms whose products were studied (Merck, Glaxo–Wellcome, and Bristol-
of subjects with this drug combination is accompa-
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
12. Mellors JW, Rinaldo CR Jr, Gupta P, White RM, Todd JA, Kingsley LA. Prognosis in HIV-1 infection predicted by the quantity of virus in
The following institutions and investigators participated in the AIDS
Clinical Trials Group 320 Study: University of North Carolina — T. Lane
13. Mellors JW, Munoz A, Giorgi JV, et al. Plasma viral load and CD4ϩ
and J. Horton; University of Cincinnati — D. Neumann and B. Letcher;
lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med
University of Puerto Rico — G. Vazquez, M. Cruz-Ortiz, and I. Lopes;
University of Minnesota — C. Kumekawa, R. Schut, and S. Swindells; Wash-14. Welles SL, Jackson JB, Yen-Lieberman B, et al. Prognostic value of ington University — P. Tebas, W. Powderly, and A. Slack; Ohio State Uni-
plasma human immunodeficiency virus type 1 (HIV-1) RNA levels in pa-
versity College of Medicine — M. Para, R. Fass, and J. Neidig; Northwestern
tients with advanced HIV-1 disease and with little or no zidovudine ther-
University — J. Pulvirenti and J. Pottage, Jr.; University of Alabama andEmory University — J. Lennox and K. Tamburello; New YorkUniversity15. Coombs RW, Welles SL, Hooper C, et al. Association of plasma hu- Medical Center and Bellevue Hospital — R. Gulick, J. Dowling, and M. La-
man immunodeficiency virus type 1 RNA level with risk of clinical progres-
verty; University of Miami — E. Scerpella and A. Rodriguez; University of
sion in patients with advanced infection. J Infect Dis 1996;174:704-12. Texas at Galveston — R. Pollard, S. Hausrath, and M. Pickthall; Case West-16. Hughes MD, Johnson VA, Hirsch MS, et al. Monitoring plasma HIV- ern Reserve University — B. Gripshover, H. Valdez, and M. Chance;
1 RNA levels in addition to CD4ϩ lymphocyte count improves assessment
Howard University — R. Delapenha, J. McNeil, and Y. Butler; Harvard
of antiretroviral therapeutic response. Ann Intern Med 1997;126:929-38. University and Boston Medical Center — L. Jackson-Pope and T. Cooley;
17. O’Brien WA, Hartigan PM, Daar ES, Simberkoff MS, Hamilton JD, University of Rochester — R. Hewitt and C. Greisberger; University of Cal-
The VA Cooperative Study Group on AIDS. Changes in plasma HIV RNA
ifornia, Los Angeles — R. Mitsuyasu, M. Guerrero, and P. Miller; Indiana
levels and CD4ϩ lymphocyte counts predict both response to antiretroviral
University Hospital — K. Fife, H. Nixon, and D. Heise; Meharry Medical
therapy and therapeutic failure. Ann Intern Med 1997;126:939-45. College and Vanderbilt University Medical Center — M.A. South, D. Haas,
18. Kohl NE, Emini EA, Schleif WA, et al. Active human immunodeficien-
and S. Raffanti; Duke University — C. Hicks, P. Robinson, and K. Shipp;
cy virus protease is required for viral infectivity. Proc Natl Acad Sci U S A
University of California, San Diego — C. Fegan, T.-C. Meng, and S. Little;
Johns Hopkins University — R. Becker, M. Higgins, L. Apuzzo, and J.B. 19. Peng C, Ho BK, Chang TW, Chang NT. Role of human immunode-
Jackson; Mount Sinai Medical Center — P. Gerits, H. Mendoza, and
ficiency virus type 1-specific protease in core protein maturation and viral
D. Mildvan; University of Pennsylvania — R.R. MacGregor, I. Matozzo,
infectivity. J Virol 1989;63:2550-6.
and E. McCann; University of Southern California — M. Dube and C. Ol-
20. Seelmeier S, Schmidt H, Turk V, von der Helm K. Human immuno-
sen; University of Colorado — D. Kuritzkes, B. Putnam, and D. Torre; Tu-
deficiency virus has an aspartic-type protease that can be inhibited by pep-
lane University and Louisiana State University — J. Lertora, R. Clark, and
statin A. Proc Natl Acad Sci U S A 1988;85:6612-6.
M. Beilke; University of Hawaii — S. Souza, M. Millard, and L. Oshita;
21. Danner SA, Carr A, Leonard JM, et al. A short-term study of the safe- Stanford University — T. Merigan, Jr., J. Fessel, and D. Israelski; Memorial
ty, pharmacokinetics, and efficacy of ritonavir, an inhibitor of HIV-1 pro-
Sloan-Kettering Cancer Center — M. Giordano, P. Ristau, and
tease. N Engl J Med 1995;333:1528-33.
M. Granville; University of Washington, Seattle — A. Collier, R. Vasquez,
22. Markowitz M, Saag M, Powderly WG, et al. A preliminary study of ri-
B. Royer, and R. Coombs; New York University Medical Center and Belle-
tonavir, an inhibitor of HIV-1 protease, to treat HIV-1 infection. N Engl
vue Hospital (pediatricsite) — W. Borkowsky, S. Chandwani, and M. Mint-
er; Columbus Children’s Hospital — M. Brady, J. Hunkler, and C. Callaway;
23. Stein D, Drusano G, Steigbigel R, et al. Two year follow-up of patients Medical University of South Carolina — G. Johnson and E. Matters; Na-
treated with indinavir 800 mg q 8 h. In: Program and abstracts of the
tional Hemophilia Foundation — T. Coates, T. Hofstra, W.-Y. Wong,
Fourth Conference on Retroviruses and Opportunistic Infections, Wash-
E. Eyster, S. Seremetis, C. Kessler, S. Stabler, W. Hanna, C. Leissenger,
ington, D.C., January 22–26, 1997:100. abstract.
J. Gill, P. Timmons, W.K. Hoots, and M. Cantini; Division of AIDS, Na-24. Gulick RM, Mellors JW, Havlir D, et al. Treatment with indinavir, zi- tional Institute of Allergy and Infectious Diseases — J. Ioannidis and A. Mar-
dovudine, and lamivudine in adults with human immunodeficiency virus
tinez; Statistical and Data Management Center — K. Kazial; Harvard
infection and prior antiretroviral therapy. N Engl J Med 1997;337:734-9. School of Public Health — S.-H. Liou; Community Constituency Group —
25. Hirsch M, Protocol 039 (Indinavir) Study Group, Meibohm A, Rawlins
H. Chang; Bristol-Myers Squibb — J. Skovronski and L. Dunkle; Merck and
S, Leavitt R. Indinavir in combination with zidovudine and lamivudine in
ZDV-experienced patients with CD4 cell counts р50 cells/mm3. In: Pro-gram and abstracts of the Fourth Conference on Retroviruses and Oppor-
tunistic Infections, Washington, D.C., January 22–26, 1997:207. abstract. 26. Powderly W, Sension M, Conant M, Stein A, Clendeninn N. The ef- 1. Hammer SM, Katzenstein DA, Hughes MD, et al. A trial comparing
ficacy of Viracept (nelfinavir mesylate, NFV) in pivotal phase II/III dou-
nucleoside monotherapy with combination therapy in HIV-infected adults
ble-blind randomized controlled trials as monotherapy and in combination
with CD4 cell counts from 200 to 500 per cubic millimeter. N Engl J Med
with d4T or AZT/3TC. In: Program and abstracts of the Fourth Confer-
ence on Retroviruses and Opportunistic Infections, Washington, D.C., Jan-
2. The Delta Coordinating Committee. Delta: a randomised double-blind
controlled trial comparing combinations of zidovudine plus didanosine or
27. Division of AIDS. Division of AIDS table for grading severity of adult
zalcitabine with zidovudine alone in HIV-infected individuals. Lancet
adverse experiences. Rockville, Md.: National Institute of Allergy and In-
3. Englund JA, Baker CJ, Raskino C, et al. Zidovudine, didanosine, or 28. Peto R, Pike MC, Armitage P, et al. Design and analysis of randomized
both as the initial treatment for symptomatic HIV-infected children.
clinical trials requiring prolonged observation of each patient. I. Introduc-
tion and design. Br J Cancer 1976;34:585-612. 4. Wei X, Ghosh SK, Taylor ME, et al. Viral dynamics in human immuno- 29. Mulder J, McKinney N, Christopherson C, Sninsky J, Greenfield L,
deficiency virus type 1 infection. Nature 1995;373:117-22.
Kwok S. Rapid and simple PCR assay for quantitation of human immuno-
5. Ho DD, Neumann AU, Perelson AS, Chem W, Leonard JM, Markowitz
deficiency virus type 1 RNA in plasma: application to acute retroviral in-
M. Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 in-
fection. J Clin Microbiol 1994;32:292-300. 30. Kalbfleisch JD, Prentice RL. The statistical analysis of failure time da- 6. Perelson AS, Neumann AU, Markowitz M, Leonard JM, Ho DD. HIV-
1 dynamics in vivo: virion clearance rate, infected cell life-span, and viral
31. Laird NM, Ware JH. Random-effects models for longitudinal data. Bi-
generation time. Science 1996;271:1582-6. 7. Havlir DV, Richman DD. Viral dynamics of HIV: implications for drug 32. Pocock SJ. Clinical trials: a practical approach. Chichester, England:
development and therapeutic strategies. Ann Intern Med 1996;124:984-94. 8. Haase AT, Henry K, Zupancic M, et al. Quantitative image analysis of 33. The Lifereg procedure. In: SAS/STAT user’s guide. 4th ed. Cary,
HIV-1 infection in lymphoid tissue. Science 1996;274:985-9. 9. Fauci AS. Host factors and the pathogenesis of HIV-induced disease. 34. Hughes MD, Pocock SJ. Stopping rules and estimation problems in
clinical trials. Stat Med 1988;7:1231-42. 10. Katzenstein DA, Hammer SM, Hughes MD, et al. The relation of vi- 35. Wong JK, Gunthard HF, Havlir DV, et al. Reduction of HIV in blood
rologic and immunologic markers to clinical outcomes after nucleoside
and lymph nodes after potent antiretroviral therapy. In: Program and ab-
therapy in HIV-infected adults with 200 to 500 CD4 cells per cubic mil-
stracts of the Fourth Conference on Retroviruses and Opportunistic Infec-
limeter. N Engl J Med 1996;335:1091-8.
tions, Washington, D.C., January 22–26, 1997:207. abstract. 11. Mellors JW, Kingsley LA, Rinaldo CR Jr, et al. Quantitation of HIV- 36. Larder BA, Kemp SD, Harrigan PR. Potential mechanism for sustained
1 RNA in plasma predicts outcome after seroconversion. Ann Intern Med
antiretroviral efficacy of AZT-3TC combination therapy. Science 1995;
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
T WO N U C L E O S I D E A N A LO G U E S P LU S I N D I N AV I R I N P E R S O N S W I T H H I V I N F E C T I O N 37. Eron JJ, Benoit SL, Jemsek J, et al. Treatment with lamivudine, zido- 43. Salgo M, Beattie D, Bragman K, et al. Saquinavir (Invirase, SQV) vs.
vudine, or both in HIV-positive patients with 200 to 500 CD4ϩ cells per
HIVID (zalcitabine, ddC) vs. combination as treatment for advanced HIV
cubic millimeter. N Engl J Med 1995;333:1662-9.
infection in patients discontinuing/unable to take retrovir (zidovudine
38. Katlama C, Ingrand D, Loveday C, et al. Safety and efficacy of lami-
ZDV). In: Volume 1 of the Abstracts of the XI International Conference
vudine-zidovudine combination therapy in antiretroviral-naive patients: a
on AIDS, Vancouver, B.C., July 7–12, 1996:24. abstract.
randomized controlled comparison with zidovudine monotherapy. JAMA
44. Harrigan R, Stone C, Griffin P, et al. Antiretroviral activity and resist-
ance profile of the carbocyclic nucleoside HIV reverse transcriptase inhib-
39. Staszewski S, Loveday C, Picazo JJ, et al. Safety and efficacy of lami-
itor 1592U89. In: Program and abstracts of the Fourth Conference on
vudine-zidovudine combination therapy in zidovudine-experienced pa-
Retroviruses and Opportunistic Infections, Washington, D.C., January 22–
tients: a randomized controlled comparison with zidovudine monotherapy.
45. Schooley RT, 141W94 International Study Group. Preliminary data 40. Bartlett JA, Benoit SL, Johnson VA, et al. Lamivudine plus zidovudine
from a phase I/II study on the safety and antiviral efficacy of the combi-
compared with zalcitabine plus zidovudine in patients with HIV infection:
nation of 141W94 plus 1592U89 in HIV-infected patients with 150 to
a randomized, double-blind, placebo-controlled trial. Ann Intern Med
400 CD4ϩ cells/mm3. In: Program and abstracts of the Fourth Confer-
ence on Retroviruses and Opportunistic Infections, Washington, D.C., Jan-
41. CAESAR Coordinating Committee. Randomised trial of addition of
lamivudine or lamivudine plus loviride to zidovudine-containing regimens
46. Ruiz N, DuPont Merck Study Group. A double-blind pilot study to
for patients with HIV-1 infection: the CAESAR trial. Lancet 1997;349:
evaluate the antiretroviral activity, tolerability of DMP 266 in combination
with indinavir (cohort III). In: Program and abstracts of the Fourth Con-
42. Cameron DW, Heath-Chiozzi M, Kravcik S, et al. Prolongation of life
ference on Retroviruses and Opportunistic Infections, Washington, D.C.,
and prevention of AIDS complications in advanced HIV immunodeficien-
January 22–26, 1997:206. abstract.
cy with ritonavir: update. In: Volume 1 of the Abstracts of the XI Interna-
47. Carpenter CCJ, Fischl MA, Hammer SM, et al. Antiretroviral therapy
tional Conference on AIDS, Vancouver, B.C., July 7–12, 1996:24. ab-
for HIV infection in 1997: updated recommendations of the International
AIDS Society-USA panel. JAMA 1997;77:1962-9.
Downloaded from www.nejm.org at UNIVERSITY OF BIRMINGHAM on December 18, 2007 .
Copyright 1997 Massachusetts Medical Society. All rights reserved.
TECHNICAL DATA SHEET XYLADECOR Xyladecor Total Wood Care is the ultimate preservation and protection product. Its Triple Action Formula, protects, treats and enhances the natural wood. It is suitable for exterior and interior use on new or pre- treated wood. It penetrates deep into the wood. It does not peel or blister. Protects against wood destroying insects and blue stain fungi. If using i
Polyploidy in Sugar Beets Induced by the Use of Colchicine, Ethyl Mercury Phosphate, and Other Chemicals1 F R A N K F . L Y N E S A N D C . D . H A R R I S 2 Chemically induced polyploids, particularly those of economic plants, have attracted considerable attention during the past 4 years. Colchicine has been widely used and is now generally accepted as a standard chemical for th
 T WO N U C L E O S I D E A N A LO G U E S P LU S I N D I N AV I R I N P E R S O N S W I T H H I V I N F E C T I O N
T WO N U C L E O S I D E A N A LO G U E S P LU S I N D I N AV I R I N P E R S O N S W I T H H I V I N F E C T I O N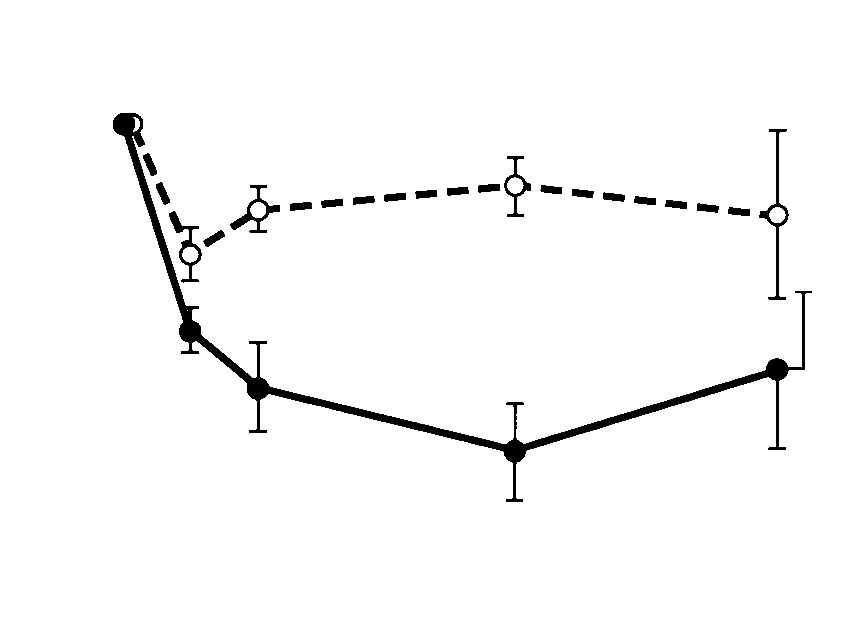
 T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
in the group receiving zidovudine (or stavudine) and
lamivudine were 0.9, 0.6, 0.6, and 1.0 log copies
per milliliter, respectively. The corresponding de-creases in the group receiving indinavir, zidovudine
(or stavudine), and lamivudine were 1.8, 2.3, 2.8,
and 2.1 log copies per milliliter (Fig. 3A). The
changes from base line were significantly greater at
each time point in the group treated with indinavir(PϽ0.001 at weeks 4, 8, and 24; Pϭ0.007 at week
40). At week 24, the proportion of patients with
plasma HIV-1 RNA concentrations of less than 500copies per milliliter was 9 percent in the two-nucle-
oside group, as compared with 60 percent in the
The plasma HIV-1 RNA responses according to
the CD4 cell count are shown in Figures 3B and 3C.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
in the group receiving zidovudine (or stavudine) and
lamivudine were 0.9, 0.6, 0.6, and 1.0 log copies
per milliliter, respectively. The corresponding de-creases in the group receiving indinavir, zidovudine
(or stavudine), and lamivudine were 1.8, 2.3, 2.8,
and 2.1 log copies per milliliter (Fig. 3A). The
changes from base line were significantly greater at
each time point in the group treated with indinavir(PϽ0.001 at weeks 4, 8, and 24; Pϭ0.007 at week
40). At week 24, the proportion of patients with
plasma HIV-1 RNA concentrations of less than 500copies per milliliter was 9 percent in the two-nucle-
oside group, as compared with 60 percent in the
The plasma HIV-1 RNA responses according to
the CD4 cell count are shown in Figures 3B and 3C.