He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Wound-treatment.jp
C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o n / P s y c h o s o c i a l R e s e a r c h O R I G I N A L Relationships Between Daily Acute Glucose Fluctuations and Cognitive Performance Among Aged Type 2 Diabetic Patients ARIA ROSARIA RIZZO, MD, PHD FRANCESCO VESTINI, MD AFFAELE MARFELLA, MD, PHD BIAGIO LETTIERI, MD
tions is still difficult. Considering that the
ICHELANGELA BARBIERI, MD, PHD SILVESTRO CANONICO, MD
brain is dependent on an appropriate sup-
IRGINIA BOCCARDI, MD GIUSEPPE PAOLISSO, MD, PHD
ply of glucose as its principal energysource, one cannot rule out the possibilitythat plasma glucose instability over 24 h
OBJECTIVE — The mean amplitude of glycemic excursions (MAGE) is a significant deter-
minant of overall metabolic control as well as increased risk for diabetes complications. Older
more practical point of view, exposure to
individuals with type 2 diabetes are more likely to have moderate cognitive deficits and structural
changes in brain tissue. Considering that poor metabolic control is considered a deranging factor
function of two components: 1) the dura-
for cognitive performance in diabetic patients, we evaluated whether the contributions of MAGE
to cognitive status in older patients with type 2 diabetes were independent from the main
hyperglycemia and 2) the acute fluctua-
markers of glycemic control, such as sustained chronic hyperglycemia (A1C), postprandialglycemia (PPG), and fasting plasma glucose (FPG).
tions of glucose over a daily period (6,7). The first component was integrated by
RESEARCH DESIGN AND METHODS — In 121 older patients with type 2 diabetes,
48-h continuous subcutaneous glucose monitoring (CSGM) were assessed. MAGE and PPG were
evaluated during CSGM. The relationship of MAGE to performance on cognitive tests was
assessed, with adjustment for age, glycemic control markers, and other determinants of cognitive
status. The cognitive tests were a composite score of executive and attention functioning and the
trol (8). The acute fluctuations of glucose
Mini Mental Status Examination (MMSE).
around a mean value is more difficult toassess, but the recent development of de-
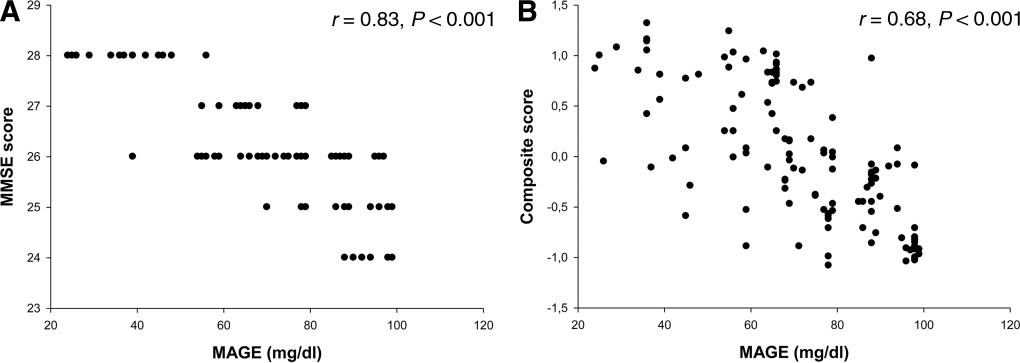
RESULTS — MAGE was significantly correlated with MMSE (r ϭ 0.83; P Ͻ 0.001) and with
cognition composite score (r ϭ 0.68; P Ͻ 0.001). Moreover, MAGE was associated with theMMSE (P Ͻ 0.001) and cognition composite score (P Ͻ 0.001) independently of age, sex, BMI,
waist-to-hip (WHR) ratio, drug intake, physical activity, mean arterial blood pressure, FPG, PPG,
the influence of acute blood glucose fluc-tuations in real life (9). By applying this
CONCLUSIONS — MAGE during a daily period was associated with an impairment of
cognitive functioning independent of A1C, FPG, and PPG. The present data suggest that inter-
further insight into the respective role of
ventional trials in older patients with type 2 diabetes should target not only A1C, PPG, and FPG
but also daily acute glucose swings.
and acute glucose fluctuations over a dailyperiod on global cognitive functioning as
Diabetes Care 33:2169–2174, 2010
well as executive and attention function-ing neuropsychological tests. Itiswidelyknownthatolderindividu- A1Cbutnotfastingplasmaglucose(FPG) RESEARCH DESIGN AND
lower scores on two cognitive tests (3). METHODS — A total of 121 older
those without type 2 diabetes (1). The un-
ing other indexes of dysglycemia, such as
glucose control and cognitive function ex-
the fact that several studies have investi-
A1C levels. Eligibility for the study was
ists (2). For instance, a cross-sectional
analysis in 378 high-functioning individ-
1-year period. The main clinical and lab-
diabetic cognitive disorders, an accurate
oratory characteristics of the patients are
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Department of Geriatrics and Metabolic Diseases, Second University of Naples, Naples, Italy; the
of walking and other leisure-time physical
2Department of Anesthesiology and Emergency, Second University of Naples, Naples, Italy; and the
activities were assessed by interview. Ex-
3Department of Surgery, Second University of Naples, Naples, Italy.
clusion criteria, assessed with self-report
Corresponding author: Raffaele Marfella, [email protected]. Received 27 February 2010 and accepted 16 May 2010. Published ahead of print at http://care.
diabetesjournals.org on 23 June 2010. DOI: 10.2337/dc10-0389.
2010 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.
illness during the 3-month period preced-
org/licenses/by-nc-nd/3.0/ for details.
ing the investigation, and cerebrovascular
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be herebymarked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
DIABETES CARE, VOLUME 33, NUMBER 10, OCTOBER 2010
Glycemic control and cognitive performance Table 1—Clinical characteristics of patients
medica, Milan, Italy) (intra-assay coefficient
of variation 3.1 ϩ 0.3%; cross-reactivity
days 1, 2, and 3. After an overnight fast,
quantified from fresh samples drawn after
participants had been fasting for at least
breakfast, respectively. The standardized
glyceride (Roche Diagnostics) levels.
white matter lesions, significant signs of
cortical or subcortical atrophy. Patients
present study for assessing glucose fluc-
white matter lesions or cortical or subcor-
tical atrophy were considered lost to fol-
data on study days 1 and 2, i.e., from con-
blinded to the study design. In brief, all
Data are means Ϯ SD, n, or n (%).
mia, is of particular interest because the
ness of the far wall was evaluated as the
distance between the luminal-intimal inter-
face and the medial-adventitial interface.
sis over a period of 3 consecutive days by
were obtained from 10 contiguous sites at
1-mm intervals, and the average of the 10
Menarini Diagnostics, Florence, Italy) as
measurements were used for the analysis.
described previously (10). The sensor was
inserted on day 0 and removed on day 3 at
consists of two parts: TMT-A and TMT-B.
one to draw a line connecting consecutive
on days 1 and 2 to avoid bias due to both
thus, to insufficient stabilization of the
and letters in alternating sequence (14).
glucose pattern of each patient was calcu-
for assays. Plasma insulin was determined
typically used to examine aspects of atten-
DIABETES CARE, VOLUME 33, NUMBER 10, OCTOBER 2010
Rizzo and Associates
Figure 1—A: Relationship between MMSE and MAGE. B: Relationship between cognitive composite score and MAGE.
quired for the study to reject the null hy-
of cognitive efficiency (15). The Wechsler
pothesis 99% of the time (i.e., with a one-
tailed type II error rate of 0.01) when r
was Ն0.80 with a two-tailed type I error
well as of brief storage and mental manip-
at the 0.05 level of significance. Because
this calculation led to a sample size of at
(DSP–Backward) requires the participant
least 110, the number of required patients
plaque at 20 –25% without significant al-
listen to increasingly longer lists of digits
was set at 121. A cluster analysis, using
terations in blood flow) on a carotid ultra-
presented for immediate recall in the re-
the squared sum of z scores, showed
lesions or significant signs of cortical or
(data not show). All patients were treated
participants to generate as many words as
we created a cognition composite score of
alone (10 –15 mg/day in 19 patients) or
possible in 1 min for a given letter (F, A, S)
attention and executive functions, as sum
of the z scores of TMT-A, TMT-B, DIFF
Verbal Fluency. A z score indicates the
day) (in 51 patients) or a combination of
position of an individual value of a vari-
able in the total distribution of the vari-
lidinediones (4 mg/day) (in 13 patients).
able in the population and is calculated as
follows: (individual value – mean value)/
those with a score of 26 were directed to
ual test scores to z scores, summing these
evaluation of older individuals with cog-
of several covariates. The effect of therapy
etiology was established using a standard
in patients categorized for number of an-
MMSE (r ϭ 0.83 P Ͻ 0.001) and with the
cognition composite score (r ϭ 0.68, P Ͻ
teria (18). All participants with diagnosed
ANOVA, and Ptrend was calculated. P Ͻ
0.05 was used of levels of significance in
thropometric (BMI and waist-to-hip ratio[WHR]), metabolic (FPG and 2-h PPG
RESULTS — The study group had
All data are expressed as means Ϯ SD.
Plasma insulin and triglycerides were log
88 – 65 years), A1C of 7.9 Ϯ 0.3%, and
and fasting insulin was observed (r ϭ
DIABETES CARE, VOLUME 33, NUMBER 10, OCTOBER 2010
Glycemic control and cognitive performance Table 2—Linear multivariate analyses with MMSE and composite score as dependent variable
For MMSE: R2 ϭ 0.73 (model 1); R2 ϭ 0.73 (model 2); R2 ϭ 0.77 (model 3). For composite score: R2 ϭ 0.40 (model 1); R2 ϭ 0.41 (model 2); R2 ϭ 0.44 (model3). SBP, systolic blood pressure; DBP, diastolic blood pressure.
nitive function (Table 2, model 3). All of
scores were tested in three different mul-
sults, even after adjustment for education
CONCLUSIONS — Our study shows
having, respectively, age, sex, BMI, WHR,
associated with daily acute glucose fluc-
postprandial glucose (model 3) as covari-
To assess the impact of antidiabetes ther-
functioning, and this relationship was in-
apy, all patients were categorized in three
tion, physical activity, mean arterial blood
according to antidiabetes treatment: gly-
of the different glycemic indexes partici-
pating in diabetic cognitive disorders (2–
4), accurate assessment of their respective
contributions is still being debated. By us-
thiazolidinediones, 73.8 Ϯ 23. No differ-
DIABETES CARE, VOLUME 33, NUMBER 10, OCTOBER 2010
Rizzo and Associates
certainly an independent risk factor of de-
as observed over interprandial periods. As
diabetes. For instance, it has been estab-
type 2 diabetes might also evoke a decline
cognitive function in individuals withtype 2 diabetes and other cardiovascular
risk factors: the action to control cardio-
bolic activity in the brain, the rapid glu-
(20). The toxicity of these substances can
levels during postprandial periods to low
mia and cognitive function in older adults
decline of metabolic activity in the brain
ited a more specific triggering effect on
Grella R, Arciello A, Laieta MT, Acampora
glucose nadirs, may affect cognitive func-
R, Passariello N, Cacciapuoti F, Paolisso G.
tion in older individuals, increasing oxi-
and cognitive functioning in aged type 2 di-
appropriate brain supply of glucose.
These observations provide a possible ex-
5. Cox DJ, Kovatchev BP, Gonder-Frederick
tive stress caused by free radicals damages
the endothelial cells in the blood vessels,
adults with type 1 and type 2 diabetes. Di-abetes Care 2005;28:71–77
6. Diabetes Control and Complications Trial
complications of type 2 diabetes. Various
the present study is its cross-sectional, ob-
tive stress can lead to microvascular cere-
servational nature, and it is therefore dif-
ficult to draw causal relationships.
cations Trial. Diabetes 1995;44:968 –983
7. Ceriello A, Hanefeld M, Leiter L, Monnier
reason for high risk of microvascular ce-
are risk factors for mild cognitive impair-
ilehto J. Postprandial glucose regulation
8. Monnier L, Lapinski H, Colette C. Contri-
tional studies with the aim of treating gly-
bution of fasting and postprandial plasma
glucose increments to the overall diurnal
hyperglycemia of type 2 diabetic patients:
flattening acute glucose fluctuations.
variations with increasing levels of HbA . Acknowledgments — No potential conflicts of
toring: roadmap for 21st century therapy.
interest relevant to this article were reported.
10. Marfella R, Barbieri M, Ruggiero R, Rizzo
lyzed and interpreted data, wrote the manu-
script, and revised/edited the manuscript.
olisso G. Bariatric surgery reduces oxida-
M.B., V.B., and F.V. analyzed and interpreted
tive stress by blunting 24-h acute glucose
ers of upward variations, there is a reason
data. B.L. designed the study and revised/
fluctuations in type 2 diabetic obese pa-
study, wrote the manuscript, and revised/
11. Service FJ, Molnar GD, Rosevear JW, Ack-
study, analyzed and interpreted data, and re-
associated with cognitive functioning in-
sure of diabetic instability. Diabetes 1970;
12. Service FJ, O’Brien PC, Rizza RA. Mea-
References
surements of glucose control. DiabetesCare 1987;10:225–237
acute glycemic excursions should be inte-
1. Fontbonne A, Berr C, Ducimetie`re P, Alp-
e´rovitch A. Changes in cognitive abilities
13. Lezak M, Howieson D, Loring D. Neuro-
over a 4-year period are unfavourably af-
psychological Assessment. 4th ed. Oxford,
larger than chronic hyperglycemia, i.e.,
fected in elderly diabetic subjects: results
14. Reiten R, Wolfson D, eds. The Halstead–
clines from relatively high glucose levels
Reitan Neuropsychologic Test Battery: The-
during postprandial periods to low values
ory and Clinical Interpretation. Tucson, AZ,
DIABETES CARE, VOLUME 33, NUMBER 10, OCTOBER 2010
Glycemic control and cognitive performance
18. American Psychiatric Association. Diag-nostic and Statistical Manual of Mental Dis-orders: DSM-IV. 4th ed. Washington, DC,
22. Dickinson PJ, Carrington AL, Frost GS,
logic findings in relapsing-remitting and
chronic-progressive multiple sclerosis. J
19. Ryan CM, Freed MI, Rood JA, Cobitz AR,
tioxidants and glycation in diabetes. Di-
16. Carlesimo GA, Caltagirone C, Gainotti G.
metabolic control leads to better working
memory in adults with type 2 diabetes. Di-
23. Ratcliff G, Dodge H, Birzescu M, Ganguli
tive data, diagnostic reliability and quali-
tative analyses of cognitive impairment.
20. Brownlee M: The pathobiology of diabetic
24. Mussell M, Hewer W, Kulzer B, Bergis K,
17. Grigoletto F, Zappala` G, Anderson DW,
Rist F. Effects of improved glycaemic con-
tion of oxidative stress by acute glucose
trol maintained for 3 months on cognitive
function in patients with type 2 diabetes.
DIABETES CARE, VOLUME 33, NUMBER 10, OCTOBER 2010
American Academy of Developmental Medicine and Dentistry Developmental Medicine & Dentistry Reviews and Reports This month’s issue of the AADMD DevelopmentalX-rays in a 45-year-old woman with a neurodevelop-Medicine & Dentistry Reviews & Reports features anarticle by Horbelt and Fenton which demonstratespoliomyelitis and complicated by severe cognitivethe value of dental
ELECTRIC FIELD MEASUREMENTS IN SEA AND GROUND: RECENT DEVELOPMENTS AND EXPERIMENTAL RESULTS Lviv Centre of Institute of Space Research, 5-A Naukova St., 290601 Lviv, Ukraine ABSTRACT The measurements of slow fluctuations of weak electricfields in the conductive media (soil, water, space plasmaetc.) is one of the most difficult problems ofmeasurement science. That is because of extremel
 Rizzo and Associates
Rizzo and Associates