He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Vaoutcomes.net
All-Cause Mortality in Randomized Trials of Cancer Screening William C. Black, David A. Haggstrom, H. Gilbert Welch
of all-cause mortality as the primary end point in cardiac drug
Background: The most widely accepted end point in random- ized cancer screening trials is disease-specific mortality. The
In this article, we review the major randomized trials of can-
validity of this end point, however, rests on the assumption
cer screening, point out inconsistencies in their disease-specific
that cause of death can be determined accurately. An alter-
and all-cause mortality results, and offer explanations for why
native end point is all-cause mortality, which depends only
these inconsistencies may have occurred. on the accurate ascertainment of deaths and when they oc- cur. We compared disease-specific and all-cause mortality in SUBJECTS AND METHODS published randomized cancer-screening trials to indirectly assess the validity of the disease-specific mortality end point.
We obtained a list of randomized trials of cancer screening
Methods: We examined all 12 published randomized trials of
from a published authoritative text devoted to this subject (14).cancer screening for which both end points were available
The text cited 16 randomized trials for which disease-specific
(seven of mammography, three of fecal occult blood detec-
mortality has been reported. Eight of these trials pertained to
tion, and two of chest x-ray screening for lung cancer). For
screening for breast cancer with mammography, three pertained
each randomized trial, we subtracted disease-specific mor-
to screening for colorectal cancer with fecal occult blood testing,
tality observed in the screened group from that observed in
and five pertained to screening for lung cancer with chest radi-
the control group and all-cause mortality in the screened
ography. In addition, we performed an electronic search on
group from that in the control group. We then compared the
PubMed (National Library of Medicine) by using authors’
differences in these two mortality measures. Results: In five
names and other relevant terms to obtain updates on these trials. of the 12 trials, differences in the two mortality rates went in
We excluded four of these randomized trials because neither
opposite directions, suggesting opposite effects of screening.
all-cause mortality nor data from which all-cause mortality
In four of these five trials, disease-specific mortality was
could be calculated were reported [the Stockholm mammo-
lower in the screened group than in the control group,
graphic screening trial (15), the London mass radiology trial
whereas all-cause mortality was the same or higher. In two (16), the Johns Hopkins study (17), and the Memorial Sloan-
of the remaining seven trials, the mortality rate differences
Kettering study (18)]. Thus, we found 12 randomized trials of
were in the same direction but their magnitudes were incon-
cancer screening for which we could obtain disease-specific andall-cause mortality (19–30): seven of mammography, three of
sistent; i.e., the difference in all-cause mortality exceeded the
fecal occult blood, and two of chest x-rays for lung cancer
disease-specific mortality in the control group. Thus, results of seven of the 12 trials were inconsistent in their direction or
For each of these 12 trials, we used the most recent source
magnitude. Conclusion: Major inconsistencies were identi-
that allowed us to determine both disease-specific and all-cause
fied in disease-specific and all-cause mortality end points in
mortality. For consistency, we reported mortality as the number
randomized cancer screening trials. Because all-cause mor-
of deaths per 10 000 person-years of observation and, for each
tality is not affected by bias in classifying the cause of death,
randomized trial, we used the same denominator for disease-
it should be examined when interpreting the results of ran-
specific and all-cause mortality. For four of the randomized
domized cancer-screening trials. [J Natl Cancer Inst 2002;
trials, we obtained mortality rates directly from the source
94:167–73] (19,27,28,30). For the remaining eight randomized trials, we
Disease-specific mortality is the most widely accepted end
Affiliations of authors: W. C. Black, Department of Radiology, Dartmouth-
point in randomized clinical trials of screening for cancer (1,2).
Hitchcock Medical Center, Lebanon, NH, and Department of Community and
The validity of this end point, however, rests on the fundamental
Family Medicine, Center for the Evaluative Clinical Sciences, Dartmouth Medi-
assumption that the cause of death can be determined accurately.
cal School, Hanover, NH; D. A. Haggstrom, Department of Medicine, Dart-
This assumption has been seriously challenged by several stud-
mouth-Hitchcock Medical Center; H. G. Welch, Department of Medicine, Dart-
ies on the accuracy of death certificates (3–9).
mouth-Hitchcock Medical Center, and Department of Community and Family
All-cause mortality, in contrast, does not require judgments
Medicine, Center for the Evaluative Clinical Sciences, Dartmouth MedicalSchool, and Department of Veterans Affairs Outcomes Group, Department of
about the cause of death. Instead, all that this end point requires
Veterans Affairs Hospital, White River Junction, VT.
is an accurate ascertainment of deaths and when they occur. Correspondence to: William C. Black, M.D., Department of Radiology, Dart-
Furthermore, all-cause mortality is a measure that can capture
mouth-Hitchcock Medical Center, 1 Medical Center Dr., Lebanon, NH 03756
unexpected lethal side effects of medical care. Because of the
(e-mail: [email protected]).
concern that some cardiac interventions may cause noncardiac
See “Note” following “References.”
deaths (10), for example, there has been a trend toward the use
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
Table 1. Twelve randomized trials of cancer screening reporting both disease-specific and all-cause mortality* Mammography Fecal occult blood Chest x-ray
*CI ס confidence interval; HIP ס Health Insurance Plan. †Insufficient data were reported to calculate CIs.
calculated the mortality from the reported number of deaths and
ferences in disease-specific mortality were more favorable to-
person-years of observation. [Person-years of observation were
ward screening than were the differences in all-cause mortality.
reported for four of these randomized trials (21–23,26) but had
In five of the 12 trials, the differences were inconsistent in
to be approximated by multiplying reported number of subjects
direction. In four of these five trials, disease-specific mortality
and years of follow-up for the other randomized trials
was lower in the screened group than in the control group,
whereas all-cause mortality was the same or higher. Among the
For each randomized trial, we subtracted disease-specific
seven studies in which the differences were in the same direc-
mortality observed in the screened group from that observed in
tion, the difference in all-cause mortality exceeded the disease-
the control group. Similarly, we subtracted the all-cause mortal-
specific mortality in the control group in two trials. As is evident
ity in the two groups. We compared the differences in these two
in Fig. 1, this inconsistency in magnitude was most dramatic for
measures of mortality and considered them to be inconsistent if
the Edinburgh mammography trial (23). In summary, seven of
they satisfied one of two conditions. First, if the differences were
the 12 trials had results that were inconsistent in either direction
not of the same sign, then we considered the differences to be
inconsistent in direction. Second, if the differences were in thesame direction but the difference in all-cause mortality exceeded
DISCUSSION
the disease-specific mortality in the control group, then we con-
Explanations for Inconsistent Direction
sidered the differences to be inconsistent in magnitude. We rea-soned that screening alone could not explain a deficit in all
Although the goal of screening is to prevent deaths from the
deaths that exceeded the number of disease-specific deaths, even
target disease, screening may affect mortality in other ways. On
if screening prevented all disease-specific deaths. Similarly, we
the positive side, earlier detection of the target disease could lead
reasoned that screening alone would not likely explain an excess
to milder treatment and prevent some treatment deaths. In ad-
in all deaths that exceeded the number of disease-specific deaths.
dition, screening could prevent deaths from other diseases that
We also calculated the 95% confidence intervals (CIs) around
are detected earlier incidentally. On the negative side, screening
the differences in mortality (31). All P values were from two-
could lead to deaths from the evaluation of screening test results
sided tests and were based on the Z test for differences in two
or from earlier treatment (of the target or other disease) that
would not have occurred without screening.
Inconsistency in direction may be partly explained by the
inherent ambiguity of disease-specific mortality. Conceptually,
Perspective
this end point should include any cause of death that is modified
Two observations concerning the mortality rates for 12
by screening, including deaths caused by the target disease, by
screening trials are striking (Fig. 1). First, disease-specific mor-
treatment of the target disease, and by the screening process.
tality constitutes only a small proportion of all-cause mortality
However, the actual rules used to determine which deaths count
(3%–16% in the control groups). Second, the differences in all-
for disease-specific mortality are rarely published with trial re-
cause mortality within each trial are generally small.
sults. Furthermore, the determination of cause of death is a com-plex process that is subject to many sources of error. High rates
Inconsistencies
of variation have been demonstrated in the recording of under-
Table 1 shows the disease-specific and all-cause mortality in
lying cause of death on death certificates, especially when mul-
screened and control groups for the 12 trials. Overall, the dif-
tiple causes of deaths are involved (3–7).
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
Fig. 1. Mortality rates in randomized trials of screening for cancers of the breast (A), colon (B), and lung (C) (19–30). HIP ס Health Insurance Plan.
Two biases may explain much of the observed inconsistency
can occur in two different ways. First, a death from another
in the direction of disease-specific mortality and all-cause mor-
cause in the screened group may be falsely attributed to the
tality differences (Fig. 2). These biases, which affect only the
target cancer because it had previously been diagnosed in the
classification of cause of death, occur independently and have
subject. Second, a death from the target cancer in the control
opposite effects on the reporting of disease-specific mortality.
group may be falsely attributed to another cause because the
Sticky-diagnosis bias. Because the target cancer in a screen-
target cancer had not previously been diagnosed in the subject.
ing trial is more likely to be diagnosed in the screened group
Although the death-review process in a screening trial can be
than in the control group, deaths are more likely to be attributed
blinded effectively to randomization, it cannot be blinded com-
to the target cancer in the screened group. This misattribution
pletely to the diagnosis or treatment of cancer, which can greatly
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
Fig. 2. Biases affecting disease-specific mortality. It is as- sumed that screening has no net effect on mortality; i.e., screening causes the same number of deaths as it prevents. For the sticky-diagnosis bias, deaths from other causes in the screened group are falsely attributed to disease, so that disease-specific mortality is reportedly higher in the screened group. For the slippery-linkage bias, deaths from disease, treatment of disease, or screening process in the screened group are falsely attributed to other causes, so that disease-specific mortality is reportedly lower in the screened group.
influence the subject’s subsequent medical care and record. To
slip away from, screening. For example, suppose a subject with
the extent that the target cancer diagnosis sticks in the screened
screen-detected lung cancer has complications of surgery that
group (or another diagnosis sticks in the control group), disease-
lead to intensive care. If the subject dies more than 1 month after
specific mortality will be biased against screening (32,33).
admission, the death might be falsely attributed to another cause,
Sticky-diagnosis bias was probably at least partially respon-
such as pneumonia. Furthermore, the term disease-specific mor-
sible for the excess lung cancer mortality observed in the
tality is too restrictive because it does not imply the inclusion of
screened group of the Mayo Lung Project, and the misclassifi-
deaths from screening in individuals without the target disease,
cation was probably most relevant to metastatic adenocarcinoma
such as a fatal hemothorax after a percutaneous needle biopsy
(30,34). More cases of adenocarcinoma of the lung were diag-
for a benign pulmonary nodule. In none of the randomized trials
nosed in the intervention group than in the control group (59
reported in Table 1 is it made clear that such deaths from screen-
versus 38 cases; P ס .05), and more deaths were attributed to
ing are included in the disease-specific mortality end point or
this cell type in the intervention group (39 versus 25 cases; P ס
how such deaths would have been identified. To the extent that
.10). In addition, adenocarcinoma was the only lung cancer cell
all these screen-related deaths are misattributed to other causes,
type for which case subjects in the screened group had a shorter
disease-specific mortality will be biased in favor of screening.
median survival than case subjects in the control group, 1.3
Slippery-linkage bias may be partly responsible for the dis-
versus 1.8 years. Lead-time, length, and overdiagnosis biases
crepancy in the Minnesota Colon Cancer Control Project (26). In
should have prolonged survival in the screened group, even if
this study, there were 1.2 fewer deaths per 10 000 person-years
early diagnosis had no beneficial effect. Because the primary site
from colon cancer in the screening group than in the control
of metastatic adenocarcinoma is often difficult to determine,
group, but there were 2.1 more deaths per 10 000 person-years
some deaths from adenocarcinoma of other organs in the inter-
from ischemic heart disease in the screening group. Similar dis-
vention group were probably misattributed to lung cancer. In
crepancies were observed in the Nottingham trial (27). These
addition, some deaths from adenocarcinoma of the lung in the
findings raise the possibility that the colon cancer screening or
control group were probably misattributed to adenocarcinoma of
subsequent treatment may cause some cardiac deaths that are not
other organs or other causes because lung cancer had not been
properly attributed to the intervention.
Sticky-diagnosis and slippery-linkage biases can both occur
Slippery-linkage bias. Many subjects in the screened group
in the same trial, and both probably did in the Mayo Lung
may undergo invasive testing for a suspicious screening result,
Project (Table 1). However, that all-cause mortality was higher
and many others may be treated for early disease. These inter-
in the screened group suggests that the slippery-linkage bias was
ventions may lead to deaths that are difficult to trace back to, or
greater than the sticky-diagnosis bias. Thus, more harm than
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
benefit was probably obscured by the combination of these two
gest that healthier subjects were randomly assigned to the
screened group. Large discrepancies in socioeconomic status at
All-cause mortality is not affected by sticky-diagnosis and
baseline confirm that there was a major imbalance after random-
slippery-linkage biases, because it does not depend on the de-
ization, which severely threatens the validity of any comparison
termination of cause of death. If screening effectiveness (as mea-
sured by disease-specific mortality) is obscured because diag-
Similarly, in the Czechoslovakian trial of lung cancer screen-
noses are sticking, deaths from other causes will be decreased
ing (29) (Table 1), the difference in the all-cause mortality be-
correspondingly so that all-cause mortality should still reveal a
tween the control group and the screened group (25.4 per 10 000
trend toward benefit (albeit not statistically significant). If
person-years; P ס .06) was greater than the lung cancer mor-
screening harm is obscured because complications are slipping
tality in the control group (24.7 per 10 000 person-years). How-
away from the intervention, deaths from other causes will be
ever, in this trial, the two groups were almost identical imme-
increased correspondingly so that all-cause mortality should still
diately after randomization. These findings suggest that there
was an underreporting of deaths from all causes in the control
Statistical considerations. Because the 95% CIs around the
group, biasing the results against screening.
differences in all-cause mortality include zero, all of the incon-
Table 2 outlines one possible framework for interpreting vari-
sistencies in direction in Table 1 could be the result of chance.
ous combinations of disease-specific and all-cause mortality.
Of course, that such an important end point has relatively wideCIs is an important observation in itself. Nevertheless, these
Validity
wide CIs do not imply that chance is the only or even the majorcause of the observed inconsistencies in direction, especially
As we have shown, examination of all-cause mortality in
when there are plausible alternative explanations.
combination with disease-specific mortality can reveal major
The problem with conventional statistics in this setting is
threats to the validity of a randomized trial, such as flaws in
highlighted by considering a screening intervention that causes
randomization and ascertainment of vital status. In addition, all-
far more harm than benefit, yet appears to statistically signifi-
cause mortality is unaffected by two biases that affect disease-
cantly reduce disease-specific mortality. For example, consider a
specific mortality—sticky-diagnosis and slippery-linkage biases.
hypothetical trial of screening in which 100 deaths from the
To date, the net effect of these biases appears to have favored
target cancer and 900 deaths from other causes occur in the
screening. In four of the randomized trials where the differences
control group. Suppose that screening prevents 30 deaths from
have been inconsistent in direction, the disease-specific mortal-
the target cancer but causes 90 deaths that are misattributed to
ity has been lower in the screened group. This result suggests
other causes in the screened group. If we assume 10 000 person-
that slippery-linkage bias has been a bigger factor than sticky-
years of observation in each arm, then these results could be
diagnosis bias and that the harms of screening have been under-
reported as a statistically significant 30% reduction in disease-
specific mortality (relative risk [RR] ס 0.70; P ס .02) and no
Increasing the rigor of the death-review process might help to
difference in all-cause mortality (RR ס 1.06; P ס .19).
reduce the effects of slippery-linkage and sticky-diagnosis bi-ases. However, there are two major limitations inherent in the
Explanations for Inconsistent Magnitude
death-review process. First, it is difficult to devise a searchstrategy that efficiently identifies all deaths that are plausibly
A difference in all-cause mortality that exceeds the disease-
related to screening. In the Prostate, Lung, Colorectal and Ovar-
specific mortality in the control group is unlikely to be the result
ian (PLCO) Cancer Screening Trial (33), which has the most
of screening, and this difference cannot be explained by bias in
thorough death-review process ever described, the criteria for
the classification of the cause of death. Instead, an inconsistency
death review include a cancer diagnosis or unknown cause of
in magnitude suggests major problems with either randomiza-
death. This search strategy would not reliably identify fatal com-
tion or the determination of vital status.
plications from an invasive procedure triggered by a false-
In the Edinburgh trial of breast cancer screening (23) (Table
positive screening test (in a patient who did not have a cancer
1), the difference in all-cause mortality between the control
diagnosis), especially if the subject died after being discharged
group and screened group (20.1 per 10 000 person-years;
from the hospital. Second, even if all the deaths could be re-
P<.001) was much greater than the breast cancer mortality in the
viewed, assigning cause of death would still be problematic. For
control group (5.1 per 10 000 person-years). These results sug-
example, if a screened subject had a fatal myocardial infarction
Table 2. Interpretations for various combinations of disease-specific mortality and all-cause mortality
All-cause lower, disease-specific not lower
Sticky-diagnosis bias: too many deaths attributed to target cancer in the screened
group (or too few deaths attributed to target cancer in the control group)
All-cause higher, disease-specific not higher
Slippery-linkage bias: too few deaths from work-up and treatment attributed to
Major flaw in randomization or in ascertainment of vital status
No net effect of sticky-diagnosis or slippery-linkage bias
All-cause higher, disease-specific higher
No net effect of sticky-diagnosis or slippery-linkage bias
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
after an invasive evaluation, it would be difficult to determine
(7) Lloyd-Jones DM, Martin DO, Larson MG, Levy D. Accuracy of death
whether the death was caused by the evaluation and, thus, at-
certificates for coding coronary heart disease as the cause of death. Ann
(8) Newschaffer CJ, Otani K, McDonald MK, Penberthy LT. Causes of death
The main argument for using disease-specific mortality in-
in elderly prostate cancer patients and in a comparison nonprostate cancer
stead of all-cause mortality is that the latter requires far more
cohort. J Natl Cancer Inst 2000;92:613–21.
person-years of observation to generate a statistically significant
(9) Albertsen P. When is a death from prostate cancer not a death from prostate
effect when screening is effective (1). However, all-cause mor-
cancer? [editorial]. J Natl Cancer Inst 2000;92:590–1.
tality should not be abandoned completely because of a large
(10) Hulley SB, Walsh JM, Newman TB. Health policy on blood cholesterol.
sample size requirement. Instead, the highest risk populations
Time to change directions [editorial]. Circulation 1992;86:1026–9.
should be targeted so that the ratio of disease-specific mortality
(11) Pitt B, Poole-Wilson PA, Segal R, Martinez FA, Dickstein K, Camm AJ,
et al. Effect of losartan compared with captopril on mortality in patients
to all-cause mortality is much greater than that in the general
with symptomatic heart failure: randomised trial—the Losartan Heart Fail-
population. This would reduce the required person-years of ob-
ure Survival Study ELITE II. Lancet 2000;355:1582–7.
servation. The selection of a high-risk population would also
(12) Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P, et al.
help to avoid the misinterpretation of statistical significance that
Effect of carvedilol on survival in severe chronic heart failure. N Engl J
could make a harmful screening intervention appear to be ben-
(13) A trial of the beta-blocker bucindolol in patients with advanced chronic
heart failure. N Engl J Med 2001;344:1659–67. (14) Kramer BS, Gohagan JK, Prorok PC, editors. Cancer screening: theory and
Perspective
practice. New York (NY): Marcel Dekker; 1999. (15) Frisell J, Lidbrink E, Hellstrom L, Rutqvist LE. Followup after 11 years—
All-cause mortality also puts the magnitude of expected ben-
update of mortality results in the Stockholm mammographic screening trial.
efit from screening into an appropriate perspective for prospec-
Breast Cancer Res Treat 1997;45:263–70. (16) Brett GZ. Earlier diagnosis and survival in lung cancer. Br Med J 1969;4:
tive decision making. Promotional efforts at screening usually
emphasize death from the target disease, which can lead poten-
(17) Tockman MS. Lung cancer screening: the John Hopkins study. Chest
tial participants to overestimate the impact that screening will
have on their probability of dying (36). One might argue that
(18) Melamed MR, Flehinger BJ, Zaman MB, Heelan RT, Perchick WA, Mar-
providing information on all-cause mortality would confuse the
tini N. Screening for early lung cancer. Results of the Memorial Sloan-
prospective screenee because the decision to be screened would
Kettering study in New York. Chest 1984;86:44–53.
appear to be a very close call, at least in terms of living or dying. (19) Shapiro S, Venet W, Strax P, Venet L. Periodic screening for breast cancer:
the Health Insurance Plan Project and its sequelae, 1963–1986. Baltimore
However, this is precisely the case for most forms of screening,
(MD): John Hopkins University Press; 1988. p. 66–89.
and knowing this may reassure the prospective screenee that
(20) Tabar L, Fagerberg G, Duffy SW, Day NE. The Swedish Two-County Trial
whatever he or she decides, a major adverse outcome is highly
of mammographic screening for breast cancer: recent results and calcula-
unlikely. This reassurance that the death outcomes are likely to
tion of benefit. J Epidemiol Community Health 1989;43:107–14.
be very similar would be extremely helpful for getting individu-
(21) Andersson I, Aspegren K, Janzon L, Landberg T, Lindholm K, Linell F, et
als to enroll in randomized trials of screening and to comply with
al. Mammographic screening and mortality from breast cancer: the Malmo
their assignment. In addition, information on all-cause mortality
mammographic screening trial. BMJ 1988;297:943–8. (22) Bjurstam N, Bjorneld L, Duffy SW, Smith TC, Cahlin E, Eriksson O, et al.
might appropriately redirect the prospective screenee to consider
The Gothenburg breast screening trial: first results on mortality, incidence,
more seriously other interventions that may provide more ex-
and mode of detection for women ages 39–49 years at randomization.
pected benefit to the individual, such as smoking cessation.
In conclusion, disease-specific mortality may miss important
(23) Roberts MM, Alexander FE, Anderson TJ, Chetty U, Donnan PT, Forrest
harms (or benefits) of cancer screening because of misclassifi-
P, et al. Edinburgh trial of screening for breast cancer: mortality at seven
cation in the cause of death. Therefore, this end point should
only be interpreted in conjunction with all-cause mortality. In
(24) Miller AB, Baines CJ, To T, Wall C. Canadian National Breast Screening
Study: 1. Breast cancer detection and death rates among women aged 40 to
particular, a reduction in disease-specific mortality should not be
cited as strong evidence of efficacy when the all-cause mortality
(25) Miller AB, To T, Baines CJ, Wall C. Canadian National Breast Screening
is the same or higher in the screened group.
Study-2: 13-year results of a randomized trial in women aged 50–59 years. J Natl Cancer Inst 2000;92:1490–9. (26) Mandel JS, Bond JH, Church TR, Snover DC, Bradley GM, Schuman LM,
EFERENCES
et al. Reducing mortality from colorectal cancer by screening for fecaloccult blood. Minnesota Colon Cancer Control Study. N Engl J Med 1993;
(1) Morrison AS. Introduction. In: Screening in chronic disease. 2nd ed. New
York (NY): Oxford University Press; 1992. p. 3–20. (27) Hardcastle JD, Chamberlain JO, Robinson MH, Moss SM, Amar SS, Bal-
(2) Prorok PC, Kramer BS, Gohagan JK. Screening theory and study design:
four TW, et al. Randomised controlled trial of faecal-occult-blood screen-
the basics. In: Kramer BS, Gohagan JK, Prorok PC, editors. Cancer screen-
ing for colorectal cancer. Lancet 1996;348:1472–7.
ing: theory and practice. New York (NY): Marcel Dekker; 1999. p. 29–53. (28) Kronborg O, Fenger C, Olsen J, Jorgensen OD, Sondergaard O. Ran-
(3) Hoel DG, Ron E, Carter R, Mabuchi K. Influence of death certificate errors
domised study of screening for colorectal cancer with faecal-occult-blood
on cancer mortality trends. J Natl Cancer Inst 1993;85:1063–8. (4) Lee PN. Comparison of autopsy, clinical and death certificate diagnosis
(29) Kubik A, Parkin DM, Khlat M, Erban J, Polak J, Adamec M. Lack of
with particular reference to lung cancer. A review of the published data.
benefit from semi-annual screening for cancer of the lung: follow-up report
of a randomized controlled trial on a population of high-risk males in
(5) Messite J, Stellman SD. Accuracy of death certificate completion: the need
Czechoslovakia. Int J Cancer 1990;45:26–33.
for formalized physician training. JAMA 1996;275:794–6. (30) Marcus PM, Bergstralh EJ, Fagerstrom RM, Williams DE, Fontana R,
(6) Maudsley G, Williams EM. “Inaccuracy’ in death certification—where are
Taylor WF, et al. Lung cancer mortality in the Mayo Lung Project: impact
we now? J Public Health Med 1996;18:59–66.
of extended follow-up. J Natl Cancer Inst 2000;92:1308–16.
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
(31) Fleiss JL. Statistical methods for rates and proportions. 2nd ed. New York
(35) Gotzsche PC, Olsen O. Is screening for breast cancer with mammography
justifiable? Lancet 2000;355:129–34. (32) Feuer EJ, Merrill RM, Hankey BF. Cancer surveillance series: interpreting
(36) Black WC, Nease RF Jr, Tosteson AN. Perceptions of breast cancer risk
trends in prostate cancer—part II: Cause of death misclassification and the
and screening effectiveness in women younger than 50 years of age. J Natl
recent rise and fall in prostate cancer mortality. J Natl Cancer Inst 1999;
(33) Miller AB, Yurgalevitch S, Weissfeld JL. Death review process in the
Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. Control Clin Trials 2000;21(6 Suppl):400S–406S. (34) Black WC. Overdiagnosis: an underrecognized cause of confusion and
Manuscript received July 2, 2001; revised November 13, 2001; accepted
harm in cancer screening [editorial]. J Natl Cancer Inst 2000;92:1280–2.
Journal of the National Cancer Institute, Vol. 94, No. 3, February 6, 2002
Alcohol and Alcoholism Advance Access published June 30, 2010 Alcohol & Alcoholism, pp. 1–7, 2010Acetyl-L-Carnitine for Alcohol Craving and Relapse Prevention in Anhedonic Alcoholics: A Randomized,Double-Blind, Placebo-Controlled Pilot TrialGiovanni Martinotti1,2,*, Daniela Reina2, Marco Di Nicola2, Sara Andreoli1,2, Daniela Tedeschi2, Ilaria Ortolani2, Gino Pozzi2,Emerenziana Iannoni
Sonochemically Synthesized Vanadyl Phosphate change in capacity under high discharge rate of 0.3 Dihydrate Cathodes C is observed. Sonochemically prepared sample exhibits also good reversibility for the Telecommunication Basic Research Lab., electrochemical lithium insertion/extraction. Electronics and Telecommunications Research Preliminary results on the electrochemical perfor
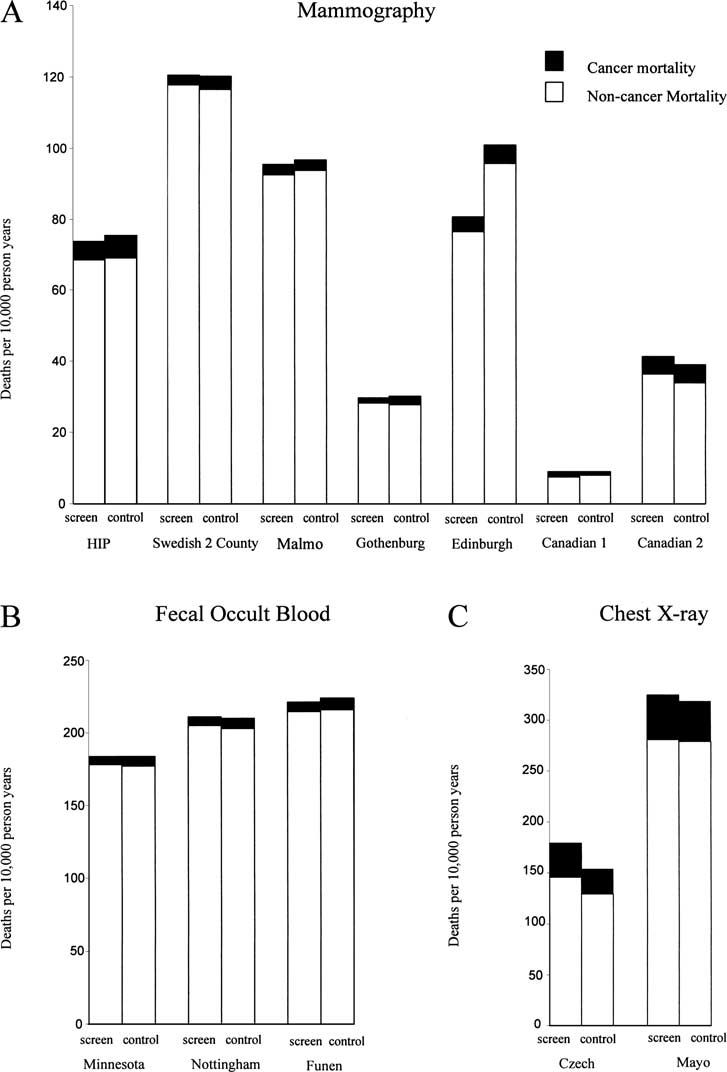 Fig. 1. Mortality rates in randomized trials of screening for cancers of the breast (A), colon (B), and lung (C) (19–30). HIP ס Health Insurance Plan.
Fig. 1. Mortality rates in randomized trials of screening for cancers of the breast (A), colon (B), and lung (C) (19–30). HIP ס Health Insurance Plan.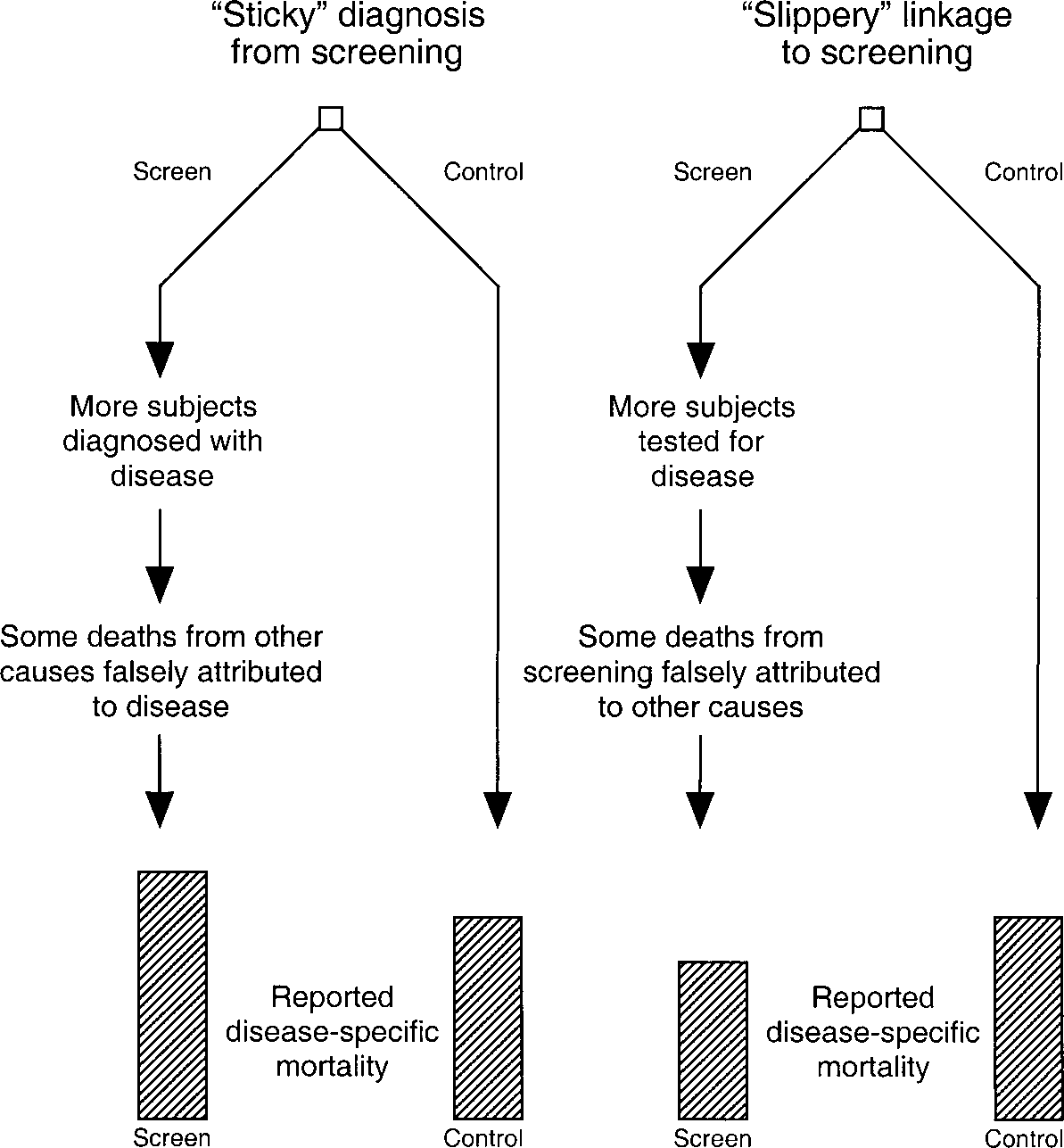 Fig. 2. Biases affecting disease-specific mortality. It is as-
Fig. 2. Biases affecting disease-specific mortality. It is as-