He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Cannabinoids for the treatment of movement disorders
Cannabinoids for the Treatment of Movement Disorders
Catherine O’Neill, BA and Juan Sanchez-Ramos, MD
Cannabis has been used to treat a wide range of medical conditions by many cultures for
thousands of years. The first written records of therapeutic use of cannabis were found in
Egyptian medical papyri dating from approximately 1700 BC. An excellent historical review of
the medicinal use of cannabis has recently been published (Russo, 2007). The first description of
cannabis to specifically treat muscle spasms was in the writings of Al-Kindi in the ninth century
AD. Almost one thousand years later, cannabis extracts were used to increase survival from
tetanus in India, and the use of cannabis preparations as muscle relaxants and anti-spasmodics
became prevalent in Britain and North America (Russo, 2007). A supply of cannabis herbal
material (in the form of “Squire’s Extract”, a tincture of Indian hemp) was brought to England
from Calcutta by a British physician who provided this to other practitioners in the British Isles.
The use of tincture of Indian hemp to treat the tremor of Parkinson’s Disease was first described
by Sir William Gowers in his landmark textbook of Neurology published in the late nineteenth
“In one case tremor had commenced in the right arm and leg an hour after a railway accident and extended, three months later into the left arm. Two years subsequently there was a constant lateral movement at the writst joints, but no tremor of the fingers. A great improvement occurred on Indian hemp and a year later the tremor had almost ceased, being occasional only.”Plant Cannabinoids, Endocannabinoids and Cannabinoid Receptors in the Brain
Cannabis contains around 60 related molecules, the phytocannabinoids (plant
cannabinoids). What purpose these molecules serve for the plant itself is not really understood.
Cannabinoids are seen by some researchers as by-products of intermediary metabolism with no
specific function in the plant. However, they may serve to repel destructive insects and to attract
others (e.g., to lure bees for cross-pollination). Some cannabinoids may possess physiological
properties involved in the regulation of plant growth and sexual development. Unlike many
biologically active plant compounds (plant alkaloids), cannabinoids contain no nitrogen.
In contrast to the paucity of information regarding the function of cannabinoids in plants,
the actions of this compound in the human brain are much better understood.
Tetrahydrocannabinol (THC) is the predominant plant cannabinoid (CB) responsible for actions
on the nervous system. The actions triggered by the binding of THC with specific cannabinoid
receptors mediate the neurologic and psychoactive effects. Cannabinol (CBN) is a metabolite of
THC and also mediates mild psychoactive effects.
Identification of brain receptors with which cannabinoids interact stimulated the quest for
the brain’s own cannabis-like drug, or endogenous cannabinoid (endocannabinoid). After many
years of research, the elusive endogenous cannabinoid was identified as arachidonyl
ethanolamide and named anandamide. The molecule is found in nearly all tissues in many
animals. Anandamide binds to both types of CB receptors, the CB1 receptor found in the central
nervous system and the CB2 receptors distributed in peripheral tissues. Anandamide is derived
from fatty acid metabolism and serves as a “lipid messenger” that activates the CB receptors on
nearby cells. Although its pharmacological properties are similar to THC, its chemical structure
Distribution of Cannabinoid Receptors in Basal Ganglia
The cannabinoid receptor has been shown to be heavily distributed in the basal ganglia of
the brain (Egertova, 2000). The basal ganglia is a term that refers to a set of interconnected deep
grey matter structures in the brain responsible for the automatic execution of learned motor
programs (See Figure 1). Dysfunction of the basal ganglia results in diseases characterized by
involuntary movements or difficulties in initiating or terminating movement. A prototype of a
basal ganglia disease is Paralysis agitans (Parkinson’s disease) which is characterized by
slowness of movement, rigidity of muscles, tremors and loss of balance. Another example is
Huntington’s chorea, a hereditary neurodegenerative disease known by its involuntary
movements that gradually worsen from tic-like jerks of muscles to complex dance-like
Figure 1 The basal ganglia are a network of inter-connected structures deep in the brain
hemispheres that are responsible for the automatic execution of learned motor programs. The
main components of the basal ganglia are the putamen, caudate, globus pallidus, substantia nigra
Injury to these structures result in diseases of motor control. The cannabinoid receptors are
heavily distrubted in these structures. Motor Effects of Cannabis
Given the abundance of cannabinoid receptors in the basal ganglia, it is not surprising
that cannabinoids have significant effects on the control of movement, both in health and disease.
Since the development of synthetic cannabinoids acting on CB receptors, dozens of studies have
reported effects on motor activity in animals. CB agonists (agents that act to stimulate the CB1
receptors) tend to initially increase locomotor activity followed by a late phase of motor
depression. Other actions reported includ the inhibition of psychomotor stimulant-induced
behavior, inhibition of exploratory behavior and production of anxiety-like behavior. Drugs that
inhibit the breakdown, or hydrolysis, of anandamide tend to potentiate its actions, resulting in
decreased locomotor and exploratory activity. The effects of specific CB receptor antagonists,
drugs which bind and block the receptors, depend on species of animal and on whether the
animals are drug naïve. CB antagonists increase locomotor activity in mice, but have no effects
on locomotion in rats. However, the antagonists increase grooming, scratching, and facial
rubbing in rats while also decreasing their exploratory behavior. Cannabinoids Modulate Neurotransmission
Cannabinoids interact with three major neurotransmitters of the basal ganglia: dopamine,
gamma amino butyric acid (GABA) and glutamate (Christie, 2001). Dopamine (DA) is the
major neurotransmitter produced by neurons located in the substantia nigra (SN). These neurons
project their fibers to the corpus striatum. Neurons that bear DA receptors in the striatum are part
of a network of neuronal feedback loops critical for the normal execution of motor programs.
Gradual loss of DA neurons of the SN results in decreased concentrations of the neurotransmitter
DA in the striatum. The loss of DA is responsible for the gradual manifestation and progression
of slowness, rigidly, and tremor, the signs and symptoms of Parkinson’s disease. Antipsychotic
drugs that block the actions of dopamine at dopamine receptors in the striatum produce sedation
as well as a parkinson-like syndrome. It is known that the CB1 receptors are co-localized with
two dopamine receptors known as the D1 and D2 receptor families. Activation of the CB1
receptor with a cannabinoid agonist inhibits both the D1 and D2 receptors and this may correlate
with the decrease in locomotor activity and sedation noted in animals given cannabinoids.
However, activation of the CB1 receptor inhibits DA re-uptake thereby potentiating the effects of
DA. Drugs that specifically inhibit DA re-uptake (dopamine transporter blockers like cocaine)
increase locomotor activity and can produce anxiety. These contrary actions are like driving with
one foot on the accelerator and the other foot on the brake. The paradoxical effects may seem
difficult to understand, but the consensus is that stimulation of CB1 receptors by cannabinoid
agonists is important for the long-term modulation of DA neuro-transmission.
Cannabinoids also act to increase GABA neurotransmission, mostly inhibiting its re-
uptake into GABA nerve terminals. GABA is the major inhibitory neurotransmitter in the
nervous system. In the basal ganglia, GABA plays a major role as a “brake” in the network of
feedback loops involved in the control of movement. GABA-like drugs and cannabinoids appear
to act synergistically. In rats the combination results in catalepsy, a profound state of immobility
during which the limbs remain in whatever position they are placed, but this is not typically seen
Cannabinoids modulate glutamate neurotransmission. Glutamate is the primary excitatory
transmitter in basal ganglia. Neurons of the sub-thalamic nucleus (an important relay station in
the feedback loops of the basal ganglia) employ glutamate as their transmitter. In Parkinson’s
disease, there is overactivity of glutamatergic transmission in the pathway from the sub-thalamic
nucleus to the globus pallidus. An overactive glutamate system may contribute to progression of
neuronal degeneration (“excitotoxicity”). In addition, many of the motor manifestations of PD
and the involuntary movements that development after long-term use of dopamine replacement
medications (levodopa) can be attributed to over activation of this glutamate-mediated pathway.
By modulating glutamate neurotransmission, some symptoms of PD can be alleviated and in
addition, may serve to slow progression of disease. In other words cannabinoids may prevent
neuronal death and can be said to possess neuroprotective properties. (Editor’s note: please see
Cannabinoids for Parkinson’s Disease
As mentioned in the beginning, tincture of cannabis indica was prescribed for Parkinson’s
disease in the nineteenth century, along with belladonna alkaloids. These latter drugs are
represented by the anti-cholinergic drugs trihexyphenydyl (Artane) and bentropine (Cogentin)
both of which continue to be occasionally prescribed to alleviate tremor which doesn’t respond
to dopamine replacement. Cannabis was rarely recommended for treatment of PD in the
twentieth century primarily because of societal and legal restrictions. However, there are many
anecdotal reports on the usefulness of cannabis preparations for treatment of symptoms of PD
and for alleviation of the involuntary movements (dyskinesias) that often plague patients who
The frequency of self-medication with cannabis in the USA is not known, but a survey of
PD patients in the Czech Republic revealed a significant proportion of respondents to a mailed
questionnaire admitted using marijuana for treatment of PD (Venderova, 2004). The survey was
triggered by many reports in the Czech media describing marijuana as potentially helpful in PD.
Out of 630 questionnaires sent by mail 339 (53.8%) were returned. The responders’ mean age
was 65.7 years and the patients had carried the diagnosis of PD for an average of 8.5 years.
Cannabis use was reported by 85 patients (25% of returned questionnaires; 55 men, 29 women).
Most of them used approximately half a teaspoon of fresh or dried leaves orally; only 1 patient
smoked the cannabis. There was no major difference in age and duration of PD between the sub-
group of patients who used cannabis and those who had never tried it. Patients usually ingested
the marijuana with meals. Interestingly, none of the patients had any experience with recreational
use of cannabis and none had been advised to use the medication by a doctor. Most decided to
give it a try based on information given in the media (newspapers and television). All of them
continued using the antiparkinsonian medications prescribed by their neurologist. After starting
to use cannabis, 39 patients (45.9%) reported mild or substantial alleviation of their PD
symptoms in general, 26 (30.6%) improvement of resting tremor, 38 (44.7%) alleviation of
bradykinesia (slowness of movement), 32 (37.7%) alleviation of muscle rigidity, and 12 (14.1%)
improvement of L-dopa-induced dyskinesias. Only 4 patients (4.7%) claimed that cannabis
actually worsened their symptoms. Alleviation of symptoms was noted within an average of 1.7
months of use. Patients who used cannabis for at least 3 months more often reported a mild or
substantial alleviation of symptoms in general. Only 2 patients used cannabis for purposes other
than alleviation of PD symptoms. One patient used it to relieve depression and the other to have
more energy. In a small analytical component of this study, a cannabinoid assay was done in the
donated urine samples from 7 patients who had taken cannabis regularly for more than one year
and a single patient who had only taken it 1 day before analysis. In the group of 7 patients with
chronic use of cannabis, there was a relationship between level of the major metabolite of THC
in the urine and the improvement of symptoms: those that had high levels (>50 ng/mL) reported
improvement in bradykinesia or rigidity. In those patients where the THC metabolite was < 50
ng/mL, there was no reported improvement in either slowness or rigidity.
Self-medication of PD with cannabis appears to be beneficial in a significant proportion
of patients. Although questionnaires have many limitations, they are quite commonly used in
clinical research because data can be collected from large numbers of individuals. Findings from
these kinds of studies cannot be conclusive but can serve as a stimulus for conducting more
Scientific evidence documenting the merits of cannabis for treating levodopa-induced
dyskinesia is spotty. Dyskinesia refers to the involuntary twisting and turning movements that
frequently result from use of the major anti-PD medicine (levodopa/carbidopa). While
laboratory work provides promising results, studies with actual patients are less conclusive. In a
pilot study published in 2001, researchers enrolled 7 PD patients with stable levodopa-induced
dyskinesias occupying 25-50% of the day (Sieradzan, 2001). All individuals received a total
dose of 0.03 mg/kg nabilone, (Cesamet, a synthetic THC and cannabinoid receptor stimulator
used to alleviate nausea and vomiting), or placebo in addition to daily levodopa. The active drug
dosage was split, with the first dose given twelve hours prior to and the second dose one hour
prior to testing. Subjects underwent two sessions of experimental treatment two weeks apart;
one involved the placebo, the other involved the active compound nabilone. Compared to
placebo, nabilone significantly reduced total dyskinesias by an average of 22.2% as measured
with the Dyskinesia Disability Scale. However, with only 7 subjects and a single trial of the
active compound, no true conclusions can be made from the data, other than more testing with a
In another study, researchers implemented a 4-week dose escalation study assessing the
safety and tolerability of cannabis in six PD patients with levodopa-induced dyskinesias.
Subsequently, the team conducted a larger randomized placebo-controlled crossover study
(RCT), that failed to demonstrate cannabis has a beneficial effect on dyskinesia in PD (Carroll,
2004). In this study, nineteen patients ages 18 to 78 received Cannador, an alcohol- based extract
from Cannabis sativa, followed by placebo or vice versa. The active drug capsules contained
2.5mg of THC and 1.25mg of cannabidiol; the placebo pills were identical in appearance.
Dosages depended on subject body weight, with a maximum of 0.25mg of THC/kg of body
weight each day. Subjects increased their intake of Cannador over a period of four weeks,
attaining a stable dose for a minimum of four days prior to testing. Assessments occurred three
times—at baseline, after treatment with placebo, and after treatment with the active drug.
However, 11 of 17 (65%) of subjects failed to reach their target dose of Cannador, averaging
instead 0.146 mg per kg of body weight/day with a range of 0.034 to 0.25mg. Dosages split into
morning and evening portions were to be increased every three days until the target weight-
adjusted quantity was reached, but subjects commonly developed intolerable side effects and
dropped back to a former tolerated dose. The most common side effect was dry mouth, though
subjects also reported constipation, nausea, lethargy, detachment, vivid dreams or nightmares and
poor concentration. Each treatment phase lasted 4 weeks with an intervening 2-week washout
period between placebo and active treatment phases. The primary outcome measure was a
change in Unified Parkinson's Disease Rating Scale (UPDRS) (items 32 to 34) dyskinesia score.
Secondary outcomes assessed how Cannador affected functioning with dyskinesia, precursors to
and duration of dyskinesia, quality of life, sleep, pain related to PD and general parkinsonism.
Seventeen of 19 patients completed the study. Cannador was well tolerated, and had no pro- or
antiparkinsonian action at the doses provided. There was no evidence for a treatment effect on
levodopa-induced dyskinesia as assessed by the UPDRS, or any of the secondary outcome
measures. Researchers were left to conclude orally administered cannabis extract resulted in no
objective or subjective improvement in dyskinesias or parkinsonism. Cannabinoids for Tourette’s Syndrome
Tourette’s syndrome is a neuropsychiatric disorder characterized by sudden involuntary
muscle jerks (tics) that commonly involve facial muscles, eyes, and head but can involve the
extremities as well. The tics often include vocalizations such as grunting, snorting sounds,
coughing and bouts of cursing . The uncontrolled verbal outbursts of coprolalia may be shocking
to anyone nearby and leads to a great deal of embarrassment. Tourette’s syndrome includes more
than motor and vocal tics and comprises a spectrum of behavioral and emotional features
including hyperactivity-attention deficit disorder and obsessive-compulsive disorders.
Past studies provide evidence that Cannabis sativa, and its major psychoactive compound
THC, are beneficial for the treatment of tics and behavioral problems seen in Tourette’s
syndrome (Muller-Vahl, 2003; Muller-Vahl, 2003b). Human and animal studies suggest the
central cannabinoid receptor CB1 is involved in regulating attention, memory and other
cognitive functions. Yet concerns exist about the effects of the drug on acute and long- term
cognition. For this reason, investigators conducted a randomized, double- blind, placebo-
controlled study of up to 10mg THC provided over a span of six weeks, on the
neuropsychological performance of 24 patients with Tourette’s syndrome (Muller-Vahl, 2003a).
Subjects ranged in age from 18 to 68 years, averaging 33 years of age. Of the 24 subjects, 17 had
never used marijuana, 4 reported occasional use, and 3 regularly smoked the herb, using it twice
or more weekly. All were asked to suspend use for six weeks prior to entering the study;
investigators conducted urine and blood analyses to confirm that THC and its metabolites were
absent before the investigation began. Subjects in the active treatment phase began taking 2.5
mg/day, increasing the dosage by 2.5mg/day over 4 days to reach 10mg/day. If individuals found
they could not tolerate the maximum dose, they were allowed to adjust the amount taken until
they achieved a maximal, yet tolerable, level. Treatment was to be taken with breakfast, once
daily. Four subjects withdrew from the study: one dropped out due to feelings of anxiety and
restlessness, two were discharged due to noncompliance, and one for questionable results on a
blood test. Of the 9 subjects who received the active drug, 6 achieved the maximal dosage of
10mg/day, 2 patients took 7.5mg/day and 1 took 2.5 mg/day. Three tests were used to assess
changes in function: the VLMT (the German version of the auditory verbal learning test,) the
Benton visual retention test (BVRT), and a divided attention test (TAP). Researchers performed a
multiple choice vocabulary test (Mehrfachwahl- Wortschatztest MWT-B) measuring verbal
intelligence at the first visit, which was later compared to results from the BVRT. Data
demonstrated no significant deterioration in cognitive function during the six week investigation.
In fact, the authors found a trend toward significance in immediate memory span in the group
given THC. Withdrawal from medication did not impact neuropsychological function. Thus, it
can be concluded that THC is beneficial for the control of tics and appears to be well-tolerated
with no significant negative influence on neuropsychological function. Dystonia
Dystonia refers to neurological conditions characterized by abnormal posturing or
movement of limbs because of sustained contractions of muscles. Dystonia can be focal, as in
torticollis, or generalized, as in idiopathic dystonia. Focal dystonias of the hand or neck resond
very well to injections of botox which produces a reversible mild paralysis of muscles.
Generalized dystonia, however, is very difficult to treat with medications. After many
medications are tried and fail, implantation of intracerebral pacemakers may be helpful in some
patients. Cannabinoids have been administered very rarely for treatment of dystonia.
Cannabadiol was shown to be minimally effective in an open label study that only included 5
patients with dystonia secondary to diverse causes (Consroe et al. 1986). In another study,
fifteen patients with regional or generalized dystonia received a single dose of placebo or
nabilone followed by the other treatment within two weeks (Fox, 2002). Two patients withdrew
due to postural hypotension or sedation. No difference between the treatments was seen in mean
total dystonic movements as assessed by a dystonia rating scale (Burke-Fahn-Marsden scale).
However in a single case study of a patient with dystonia associated with Wilson’s Disease (a
disorder of copper metabolism), smoking 3 to 4 grams of marijuana each day resulted in marked
improvement of the dystonia, documented on video in the Movement Disorders journal (Uribe
Roca, 2005). The usefulness of cannabinoids for dystonia will clearly depend on the correct
formulation of the cannabinoid. The complex mixture of smoked marijuana appeared to be very
helpful in the single case of Wilson’s Disease. The ability to gradually titrate the dose to a
tolerable and effective one will be important when chosing the formulation and dosage regimen
Huntington’s Disease
Huntington’s Disease (HD) is a hereditary neurodegenerative disease that affects mood,
cognition and control of movements. It follows an autosomal dominant inheritance pattern, so
that a parent with the gene will, on average, transmit the illness to 50% of his/her children. The
illness is not expressed immediately; the average age of onset is in the late 30s or early 40s.
There is no cure for this illness; medications are used to alleviate symptoms of depression and to
control involuntary movements. Chorea is the most common movement observed in HD,
constant dance-like movements that plague the patients as the disease evolves. There are many
anecdotal reports of HD patients, who tend to be relatively young, smoking marijuana to relieve
their chorea. However, controlled clinical trials of cannabinoids for HD are rare and have not
used THC or its variations. There is a single study of cannabidiol for treatment of HD in 15
patients that failed to produce significant benefit (Consroe, 1991). Clearly, there is a need to do
more studies with various preparations of cannabis or synthetic cannabinoids in this patient
Neuroprotective Effects
Cannabinoids have been found to have antioxidant properties. In fact, a US Patent was
awarded to researchers from the National Institute of Health in 2003 entitled “Cannabinoids as
Antioxidants and Neuroprotectants” (Hampson, 2003). This new found property makes
cannabinoids useful for limiting neurological damage following ischemic insults, such as stroke
and trauma, or in the treatment of neurodegenerative diseases such as Alzheimer's disease,
Parkinson's disease and HIV dementia (Grundy, 2002; Croxford, 2003; Alsasua del Valle, 2006).
Theoretically, use of cannabinoids may delay onset or mitigate the course of various
neurodegenerative diseases. What is not known is how long, what dose, and which formulation
of cannabis will be the most effective neuroprotective agent.
1. Cannabinoid receptors are distributed heavily in outflow nuclei of basal ganglia.
2. Basal ganglia are responsible for the automatic execution of learned motor programs.
3. Cannabinoid drugs modify movement in rodents and in humans.
4. Cannabinoids have potential to serve as therapeutic agents for movement disorders.
5. Cannabinoids have anti-oxidant effects and may serve as neuroprotective agents to slow
progression of neurodegenerative diseases.
References
Alsasua del Valle A (2006): Implication of cannabinoids in neurological diseases. Cell Mol
Carroll CB, Bain PG, Teare L, Liu X, Joint C, Wroath C, Parkin SG, Fox P, Wright D, Hobart J,
Zajicek JP (2004): Cannabis for dyskinesia in Parkinson disease: a randomized double-blind crossover study. Neurology 63:1245-1250.
Christie MJ, Vaughan CW (2001): Neurobiology Cannabinoids act backwards. Nature 410:527-
Consroe P, Laguna J, Allender J, Snider S, Stern L, Sandyk R, Kennedy K, Schram K (1991):
Controlled clinical trial of cannabidiol in Huntington's disease. Pharmacol Biochem Behav 40:701-708.
Consroe P, Sandyk R, Snider SR (1986): Open label evaluation of cannabidiol in dystonic
movement disorders. Int J Neurosci 30:277-282.
Croxford JL (2003): Therapeutic potential of cannabinoids in CNS disease. CNS Drugs 17:179-
Egertova M, Elphick MR (2000): Localisation of cannabinoid receptors in the rat brain using
antibodies to the intracellular C-terminal tail of CB. J Comp Neurol 422:159-171.
Fox SH, Kellett M, Moore AP, Crossman AR, Brotchie JM (2002): Randomised, double-blind,
placebo-controlled trial to assess the potential of cannabinoid receptor stimulation in the treatment of dystonia. Mov Disord 17:145-149.
Gowers W (1888): A Manual of Diseases of the Nervous System. Philadelphia, PA, P. Blakiston
Grundy RI (2002): The therapeutic potential of the cannabinoids in neuroprotection. Expert Opin
Hampson A, Axelrod J, Grimaldi M (2003): Cannabinoids as Antioxidants and Neuroprotectants;
in Office USP, (ed). USA, vol US 6,630,507 B1.
Muller-Vahl KR (2003): Cannabinoids reduce symptoms of Tourette's syndrome. Expert Opin
Muller-Vahl KR, Prevedel H, Theloe K, Kolbe H, Emrich HM, Schneider U (2003a): Treatment
of Tourette syndrome with delta-9-tetrahydrocannabinol (delta 9-THC): no influence on neuropsychological performance. Neuropsychopharmacology 28:384-388.
Muller-Vahl KR, Schneider U, Prevedel H, Theloe K, Kolbe H, Daldrup T, Emrich HM (2003b):
Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial. J Clin Psychiatry 64:459-465.
Russo EB (2007): History of cannabis and its preparations in saga, science, and sobriquet. Chem
Sieradzan KA, Fox SH, Hill M, Dick JP, Crossman AR, Brotchie JM (2001): Cannabinoids
reduce levodopa-induced dyskinesia in Parkinson's disease: a pilot study. Neurology 57:2108-2111.
Uribe Roca MC, Micheli F, Viotti R (2005): Cannabis sativa and dystonia secondary to Wilson's
Venderova K, Ruzicka E, Vorisek V, Visnovsky P (2004): Survey on cannabis use in Parkinson's
disease: subjective improvement of motor symptoms. Mov Disord 19:1102-1106.
Pretreatment for Nerve Agent Exposure Chapter 6 PRETREATMENT FOR NERVE AGENT EXPOSURE MICHAEL A. DUNN, M.D., FACP*; BRENNIE E. HACKLEY, JR., PH.D.†; AND FREDERICK R. SIDELL, M.D.‡ INTRODUCTION AGING OF NERVE AGENT–BOUND ACETYLCHOLINESTERASE PYRIDOSTIGMINE, A PERIPHERALLY ACTING CARBAMATE COMPOUND Efficacy Safety Wartime Use Improved Delivery CENTRALLY ACTING NERVE AGENT
Journal of Food Protection, Vol. 73, No. 2, 2010, Pages 376–379Copyright G, International Association for Food ProtectionAntibiotic Resistance in Salmonella Isolates from ImportedChicken Carcasses in Bhutan and from Pig Carcasses in VietnamL. ELLERBROEK,1* D. NARAPATI,2 N. PHU TAI,3 N. POOSARAN,4 R. PINTHONG,4 A. SIRIMALAISUWAN,4P. TSHERING,2 R. FRIES,5 K.-H. ZESSIN,5 M. BAUMANN,5 AND A. SCH
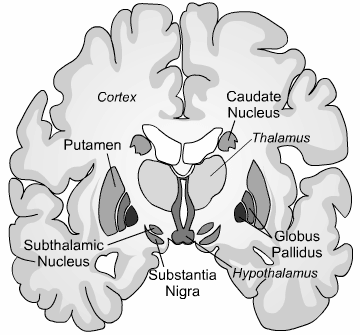 Figure 1 The basal ganglia are a network of inter-connected structures deep in the brain
Figure 1 The basal ganglia are a network of inter-connected structures deep in the brain