He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Sample report - summarization
__________ MD of Facility name – Emergency treatment record. The patient presented to ER for the complaints of pain in the right hip and lower back, heavy per vaginal bleeding, and cramping in abdomen. She has had these complaints since last 6-7 months. She has had three back injections. Pain was sharp and diaphoretic with movement. Examination showed +2 tenderness in the lumbosacral region. Laboratory tests were reviewed revealing normal CBC, urinalysis, and BHCG. Diagnosis was “Lumbosacral strain and dysmenorrhea.” The patient was given intramuscular Toradol and Phenergan. She was mini-cathed for clear yellow urine and it was sent to lab. Advil and Darvocet were prescribed and the patient was recommended follow-up in 2-3 days and off work for three days with bed rest. She was discharged in good condition. Facility name – Laboratory report. Hematology, urinalysis was unremarkable. HCG pregnancy test was negative.
__________ MD of Facility name – Emergency room report. The patient presented with complaints of face pain and left-sided neck pain. She reported she struck her face about an hour ago when she was breaking up a fight between her two children. One of them was waving a plaster splint around and hit her on the face and side of the neck two or three times with it. She was seen at the ???? Center before coming to the ER and received an intramuscular injection of Toradol. History was significant for fibromyalgia and chronic neck and back pain. Examination showed tenderness in the paraspinous muscle in the cervical spine with muscle spasm. The patient did hold her head tilted to the right, slightly. On the face, there was an abrasion which was very superficial on the right cheek. She had tenderness over the left temporomandibular joint and generalized diffuse tenderness about the face. The face was tender to even light touch. X-ray of the mandible was reviewed as normal. The impression was “Contusions, cervical muscle strain, and facial abrasion.” The patient was advised to use heat alternating with ice to the muscles of the neck. Prescriptions for Vicodin, Flexeril, and ibuprofen were provided and she was advised to follow-up with Dr. ??? for re-evaluation. She left in good condition. ????, MD of ???? Medical Center – Report of x-rays of mandible, 4 views. The findings/impression was “Bone density and alignment were normal without evidence of fracture or dislocation. Adjacent visualized bony structures were unremarkable.” ????, MD of ???? Medical Center – Report of ultrasound of the pelvis. The study was performed for the complaints of dyspareunia and the history of hysterectomy. The findings showed absent uterus. Right ovary measured 1.7 x 2.7 x 2.1 cm in size. It contained a single small follicular cyst. There was no solid mass. The left ovary measured 1.6 x 1.0 x 2.0 cm in size which contained follicular cysts that were quite small. There was no evidence of a pelvic mass. There was no cul-de-sac fluid. The impression was “Normal examination of a post-hysterectomy pelvis.” ????, MD of???? Medical Center – Emergency room report. The patient was evaluated for epigastric abdominal pain since a month with abdominal bloating and distension. The discomfort was essentially constant but episodically exacerbated for approximately a minute at a time. She had no change in symptoms with eating meals. Bowel movements were daily and quite soft. She had treated herself with Mylanta which resulted in some diarrhea but no change in symptoms of discomfort. Her primary care physician had started her on Mylanta and Zantac, but without any improvement. She was referred to gastroenterology but was unable to be seen until May. Review of systems was positive for diminished appetite such as early satiety, shortness of breath, and some stress incontinence which was a chronic symptom. Medical history was significant for hiatal hernia, stress incontinence, status post abdominal hysterectomy in January 1997 for dysfunctional uterine bleeding, para 8-0-3-4, status post appendectomy which sounded like a perforated appendicitis as a child requiring a three-week hospitalization. Ongoing medications were Zantac and Mylanta. Abdominal exam was remarkable for well-healed surgical incisions in the lower quadrants. She tolerated deep palpation in all extremities but there was some mild to moderate tenderness over the epigastrium and right upper quadrant. The patient was given IV droperidol. Lab data was reviewed. The patient was not pregnant. CT scan was obtained. The diagnosis was “Abdominal pain and distension of unclear etiology.” The patient was encouraged to return to emergency department for fevers, increasing abdominal pain, distention, or worsening course. She was encouraged to continue her Zantac and Mylanta therapy and was discharged home with referral to gastroenterology clinic for follow-up within one week. ???? Medical Center – Laboratory report. Basic metabolic panel and liver functions were unremarkable. WBC was 9.5, hematocrit 42.6, platelet count 192,000 with 39% neutrophils, 5% bands 25% lymphocytes. Eosi was high at 2.4. Urinalysis was unremarkable. Urine pregnancy test was negative.
???, MDof ???? Medical Center – Report of CT of the abdomen and pelvis. The liver, gallbladder, spleen, pancreas, adrenal glands, kidneys, and GI tract, and pelvic organs were of normal appearance. No intra- abdominal or retroperitoneal mass or adenopathy was present. The lung bases were clear. The impression was “Normal CT of the abdomen and pelvis.” ???? Medical Center – Laboratory report. Hormonal assay was normal.
???? Medical Center – Cytology report. Specimen was vaginal. The impression was “No evidence of intraepithelial lesion or malignancy.” ????, PT of ???? – Physical therapy evaluation. The patient had a lifelong history of low back pain but she had been pain free since L4-5 discectomy in August 2001 until MVA of 06/08/02. She had improved tremendously since the accident by doing the exercises on her own, but she still had pain rated at 7-8/10 in her lower back and left buttock. She had attended pool therapy in the past with very good results. The diagnosis was “Fibromyalgia/back pain.” The patient was recommended pool therapy for six sessions and then to release to independent pool program so she could continue to use pool on her own for exercise. Treatment goals were reviewed and documented. ????, DOof ???? Medical Center – Report of lumbar myelogram. The indication for study was low back and left leg pain. It revealed mild ventral defects at L2-L3 through L4-L5 but no evidence of central canal stenosis. Nerve root sleeves bilaterally opacified at all visualized levels. Vertebral body height and disc spaces were maintained. The impression was “Mild ventral defects due to disc bulges at L2-L3 through L4-L5 but no evidence of central canal stenosis.” Findings would be further evaluated on CT scan. ????, MD of ???? Medical Center – Report of post lumbar myelogram CT scan enhanced with 2D reconstructions. Comparison was made with outside MRI of the lumbar spine dated 04/29/03. Findings at T12 to L3-4 showed mild disc bulge at L3-4 and a small central disc protrusion L2-3, similar to the prior MRI scan as well as an MRI scan from 02/07/02. The nerve root sleeves opacified well at all visualized levels. The conus medullaris terminated at the upper L1 level. Neural foramina were normal in appearance at all levels. At L4-5, there had been a left hemilaminotomy. There was a disc bulge present more prominent on the left resulting in mild left ventral defect. Both L5 nerve root sleeves opacified well, transit and exit the neural foramina without contact. No central canal stenosis. At L5-S1, there was no significant findings except for minimal neuroforaminal stenosis. Nerve roots transit and exited without contact. Sagittal and coronal reconstruction images showed maintained alignment as well as vertebral body heights. The impression was “The myelographic findings are similar to that described on prior MRI scans dating back to 02/07/02. These include a small central disc protrusion at L2-3, resulting in mild central ventral defect, but lateral recess or central canal stenosis. Additionally, postoperative changes at L4-5 with a mild disc bulge and postoperative granulation at this level, but no evidence of nerve root contact or significant lateral recess stenosis.” ????, MD of ???? Medical Center – Operative report. The preoperative and postoperative diagnosis was “Spinal headache.” The procedure performed was Epidural blood patch. The indication of the procedure was a posture headache following a diagnostic myelogram without any fevers. The headaches were better with lying flat and she had failed conservative measures. Following the procedure, the patient had relief of her headache and discharged in good condition with instructions to follow- up. She was given Versed 6 mg intravenously and monitored throughout by the nurse in attendance prior to the procedure. ????, MD of ???? Medical Center – Operative/procedure report. The preoperative diagnosis was lumbar radiculopathy. The procedure performed was Selective nerve root injection, L5. The patient was contacted the next day and said that she had complete relief of pain until 10 o’clock that night and then had a gradual return of the pain. While the block was in effect, she had a left foot drop and numbness in the distribution of her usual pain. She was advised to follow-up with Dr. ????. ????, MD of ???? Clinic – Report of EMG and NCV of the lower extremities. The conclusion was “There is mild denervation at this time in the left L5 myotome (tibialis, anterior and extensor hallucis muscles) with no denervation in the lumbar paraspinals. Not able to assess motor units because she had no volitional movement of these muscles during today’s EMG. This suggests an age indeterminate L5 radiculopathy. There is no evidence of peripheral neuropathy, myopathy or plexopathy at this time. A new disposable monopolar EMG needle was used and discarded for this study.” ????, MD of ???? Center – Initial neurosurgical consultation. The patient was seen at the request of Dr. ???? for low back pain and left leg pain, left-sided foot drop, neck pain, and bilateral arm pain with numbness, and weakness. She described several years’ history of lumbar problems as well as neck pain and bilateral hand weakness. She was involved in a motor vehicle accident on ????.Prior to the accident she did have a history of L4-5 laminectomy and had initially done well from this. She then was involved in the accident on ???? and since that time complained of severe pain in the left leg, which radiated into the L5 distribution down to the lateral calf. She also described weakness of dorsiflexion in the left leg as well. She had difficulty driving secondary to the left sided foot drop. She had undergone a bladder stimulator by Dr. ???? recently and had done very well in this regard. She also described neck pain and bilateral arm pain and numbness as well as weakness in grip primarily in the left hand but also in the right hand. Overall she was getting worse with regard to the
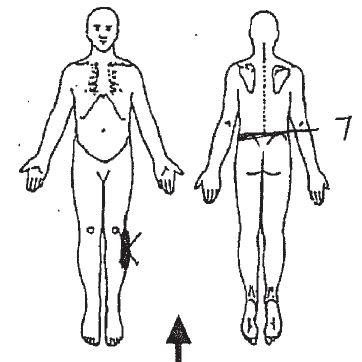
foot drop as well as neck pain, bilateral arm pain and numbness and weakness. The review of systems was positive for occasional headaches and arthralgias. The past medical history was significant for arthritis, incontinence, and fibromyalgia. She had a bladder stimulator placed in 2004 and lumbar laminectomies and discectomies in 2002 and 2003. Her medications included Ditropan and Effexor. On physical examination, the lumbar range of motion was decreased to 70 degrees of flexion and 20 degrees of extension. She had positive Spurling’s sign bilaterally. She had 4/5 strength in the biceps and hand grip bilaterally. She had complete foot drop of the left leg and very weak plantar flexion of the left leg with 1/5 in plantar flexion and 0/5 in dorsiflexion. In the right leg, the plantar flexion was 2-3/5 and dorsiflexion was 1-2/5. The radiographic studies were reviewed. It was noted that the lumbar MRI did not show anything which explained the left foot drop and she showed no signs of myelopathy to suggest any compressive lesions higher. As far as her hand weakness was concerned upper extremities nerve conduction studies were ordered. It was believed that the patient could be a candidate for C5-6 anterior cervical discectomy and fusion given her moderate neural foraminal narrowing, C6 distribution of pain, intermittent numbness into the thumb and index finger of both hands, weakness, and biceps function bilaterally worse on the left side. She was advised to follow-up after completion of the studies ordered. ????, PT of???? - Physical therapy evaluation.The patient presented with decreased strength in trunk and left lower extremity muscles, left drop foot, bilateral upper extremity weakness, and cervical pain. date of onset was 06/08/02. She described her pain as dull ache, only with movement, associated with numbness, pain located in lumbar spine on the left side radiating to the left lower extremity, exacerbated by activity, bend, lie, stairs, stand, walk, and alleviated by rest. She had difficulty with walking and activities of daily living. She rated her pain as 7/10. A pain diagram identified the symptomatic areas as shown below:
She also had bladder urgency and frequency incontinence, rated at 8/10. She had been on Ditropan for 5 years. Even with InterStim unit she was
unable to control bladder. Examination showed kyphosis of the lower thoracic region and flat lumbar spine with increased left sided cervical paraspinals. Lumbar spine range of motion was limited by pain. the patient attempted substitution pattern due to fear of moving into pain and weakness. There was tenderness in the upper thoracic and lumbar paraspinals. Range of motion was measured as flexion 15 with pain, extension 30 with pain, bilateral side bending 25 with pain, and right and left rotation to 50. Myotomes showed strength of hip flexors 4/5 on the right and 3+/5 on the left, knee extensors 4-/5 on the right and 3/5 on the left, ankle dorsiflexion 4-/5 on the right and 0/5 on the left, EHL/peroneals 4-/5 on the right and 0/5 on the left, gastrocs/hamstring 4/5 bilaterally. There was poor control of multifidus muscle bilaterally, weak/painless poor control of transverse abs, 4-/5 of psoas, weak/painless poor control of back extensors, 3-/5 of gluteus maximus, and 3/5 of gluteus medius. Straight leg raise test was negative but caused increased tension through left hip causing discomfort due to InterStim unit. Double knee to chest caused decreased symptoms. Examination of the hip showed neurostim device palpable at left superior glut. The patient was shaky with all muscle testing, difficult to get true assessment of strength. Tenderness was elicited around the InterStim device. Iliopsoas strength on the left was 4-/5, gluteus maximus and hamstring was 3-/5, gluteus medius was 3/5. She had no active ankle dorsiflexion on left and her PROM ankle dorsiflexion was decreased. She ambulated with increased knee and hip flex to accommodate drop foot on the left. She was recommended trial of AFO in the clinic and if helpful ordering a custom one made. Due to weakness and extreme pain level, she was recommended pool therapy for general strengthening and lumbar stabilization. The diagnosis was “Left leg pain and neuropathy.” The treatment plan was therapy for 12 visits to include self care techniques, therapeutic exercises, gait training, hot packs, and cryotherapy. Goals were defined. ???? of ???? – Progress note. The patient was three weeks status post C4- 5 ACDF with removal of the hardware from C6-7. Her severe preoperative neck pain and bilateral shoulder pain and arm pain had improved significantly. She was one-week status post L4-5 PLIF with significant improvement in severe low back pain and left greater than right leg pain. She was unable to tolerate oral narcotics and had been taking ibuprofen with good results. She was returning to many of her daily usual activities without difficulty. On examination, the cervical incisions were well healed and lumbar staples were in place. The impression was “The patient doing well status post C4-5 ACDF and L4-5 PLIF.” The staples were removed from the lumbar incision without complications or drainage. Her lifting and activity restrictions were discussed. She was to be reassessed in three months with plain film cervical and lumbar x-rays. ????, MD of ???? – History and physical note. The patient presented for follow-up and noted improving neck pain and bilateral shoulder and arm pain, numbness and weakness for six months; improving headaches from six months; and worsening lumbar pain and left greater than right leg pain, numbness and weakness with urinary incontinence since six months. She had multiple cervical and lumbar spinal fusion surgeries. Over last six months, she had increasing low back pain and left greater than right leg pain, numbness and weakness, constant severe headaches that radiated to the top of her head, severe neck pain, bilateral arm pain, numbness and weakness and urinary incontinence. She noted that her symptoms were constant and progressive and she described the pain as a burning pain in all areas. The patient had tried and failed conservative measures for four months including time, rest, physical therapy, chiropractic care, anti- inflammatory medications, and narcotic pain medications. She had some improvement in her headaches, neck pain, and bilateral shoulder and arm pain with the chiropractic care. She had no improvement in the low back pain and left greater than right radicular pain. She described sharp shooting pain in the back radiating to both the legs, worse on the left side than the right, with pain and numbness in the lateral calf of the leg. She was miserable about her symptoms which had worsened to the point that she could now barely walk and had difficulty sleeping at night. Review of systems was positive for intermittent headaches, neck pain, bilateral arm pain, severe low back pain and bilateral burning dysesthetic leg pain. On physical examination, the patient was in moderate distress secondary to severe low back pain and left greater than right bilateral radicular leg pain. She walked with an antalgic gait and appeared uncomfortable on the examination table. The cervical range of motion was reduced to 30 degrees of forward flexion and 30 degrees of extension and 30 degrees on lateral bending in either direction with 45 degrees of lateral rotation in either direction. The Spurling maneuver was positive bilaterally and the Lhermitte sign was positive as well. She had severe occipital and posterior cervical muscle spasms. Lumbar range of motion was reduced to 40 degrees of forward flexion with 10 degrees of extension. She did have moderate paralumbar muscle spasms present. She did have well healed midline lumbar scar. The motor examination showed 4+/5 strength diffusely in the upper and lower extremities. The patient was unable to stand on her heels and toes or squat to a seated position secondary to pain. There were numbness and paresthesias into the posterior and lateral aspects of both legs. The deep tendon reflexes were 4+ at the knees and 3+ at the ankles bilaterally. Toes were up going bilaterally. The gait was not ataxic but was antalgic. Previous diagnostic studies were reviewed. The assessment was “Improving headaches, neck pain, and bilateral shoulder pain and arm pain with normal brain and cervical MRI. Severe worsening of low back pain and recurrent left greater than right radicular leg pain, numbness, and weakness with urinary incontinence despite seven months of conservative measures.” The patient was having good results with chiropractic care to her cervical spine and she was to continue this. The patient was to undergo L3-4 and L4-5 decompression and posterior lumbar interbody fusion. She was scheduled for the same. The risks and benefits of the surgery were explained to the patient in detail.
????, MD of ???? – Report of x-ray of the cervical spine, lateral view. This study was compared to CT cervical spine dated 02/03/11. The findings and impression revealed that there had been “Interval anterior discectomy at C3-C4, with insertion of interbody fusion implant. Anterior fusion hardware has been revised, now consisting of a plate and attaching screws spanning C3-C5. There had been earlier discectomies at C4-5, C5-6 and C6-7. Vertebral body heights and alignment are preserved from C2-7 [sic].” ???? MD of ???? – Progress note. The patient returned two weeks status post L5-S1 PLIF and three weeks status post C3-4 ACDF. Her severe preoperative neck pain and right arm radicular pain had resolved. Her preoperative low back pain and right leg radicular pain had improved significantly. She had some residual numbness in both the feet that had been troublesome and kept her awake at night. She stated that the pain medications made her feel sick and she could take only Tylenol. She was returning to her usual daily activities without difficulty and stated that she was much better than she was prior to the surgery. On examination, the cervical incision Steri-Strips were in place. The incision was clean, dry, and intact. She had numbness in the left calf and dorsal plantar aspect of both the feet. The impression was “The patient healing status post cervical and lumbar fusion.” She was reassured that her symptoms should improve with time. She was to be reassessed in six weeks.
ANOTHER SAMPLE
05/02/11 DOCTOR NAME / FACILITY Fluoroscopic-guided left wrist arthrogram. Impression: 1. Successful fluoroscopic-guided left wrist arthrogram, demonstrating TFC tear.
• The patient presented for a final surgical decision making visit
• The risks, benefits, and nonsurgical alternatives were discussed and
the patient understood these and agreed to proceed with the surgical procedure,
• The patient’s ulnar nerve neurologic findings were normal by Dr.
• Do not recommend any type of intervention on the ulnar nerve.
• The wrist remained very painful and the patient wanted something to
• The TFCC central perforation seen on MRI could be treated with debridement.
• Suggest repair using a Mitek anchor to assist in stabilizing the TFCC
• The patient signed the informed consent, but was made aware that his
pain could persist due to aggravation of some underlying arthritic changes in the wrist.
Operative report.
Preoperative and postoperative diagnoses:
o Peroneus brevis tendon tear, left ankle
1. Exploration of peroneal tendons on the left. Débridement of left peroneal brevis tendon, and tubularization of left peroneus brevis tendon.
2. The patient tolerated the procedure well without any
Operative report
????, MD (Bilateral L4 SNRB #2)
• Confirm bilateral L4 nerve root mediated symptoms
Procedure 1. Right L4 selective nerve root block with steroid injection. 2. Left L4 selective nerve root block with steroid injection. 3. Epidurography. Result o Tolerated well with no complications. o Complete resolution of low back pain and bilateral lower extremity symptoms
o 7/10 to 0/10
o 45 yo o Low back and left lower extremity radiculopathy o Left arm pain o S/P MVA o Last seen 6/09/11 underwent confirmatory L4 SNRB o Reported complete temporary resolution of pain o Had a week of significant improvement and then pain gradually
o Not as intense o 4-6/10 now o Across low back o Occasional left lower extremity o He tells me that has been evaluated by a spine surgeon Dr. ????
o On discussion I explained that do not think L5 SNRB will offer much
o Patient suffers from discogenic mediated pain and confirmatory
o Recommend second surgical opinion o Patient will take this into consideration and follow up in 4 weeks.
Recent Advances in the Prevention andTreatment of Congenital Cytomegalovirus InfectionsStuart P. Adler, MD,* Giovanni Nigro, MD,† and Lenore Pereira, PhD‡Continued but slow progress has led to recent advances in our understanding that con-genital cytomegalovirus (CMV) infection has occurred. We understand that the mostsevere congenital disease occurs following a primary maternal infection
NOTAS TÉCNICAS El programa globos + bases ha sido estudiado para permitir iluminar, rayos ultravioletas, se conserva mejor contra el envejecimiento. con una luz controlada o difusa, tanto los espacios al aire libre como CARACTERíSTICAS TÉCNICAS ambientes internos. Los globos se realizan empleando las tecnologías Globos: De policarbonato irrompible y autoextinguible V2,
 foot drop as well as neck pain, bilateral arm pain and numbness and
foot drop as well as neck pain, bilateral arm pain and numbness and