He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Pii: s1569-9056(02)00112-4
European Urology Supplements 1 (2002) 4±11
What Do Patients Expect from Erectile DysfunctionTherapy?Geoffrey I. Hackett*Good Hope Hospital, Sutton Cold®eld, Elford Road, Fisherwick, Lich®eld, Straffordshire WS 149JR, UK
Erectile insuf®ciency can precipitate emotional distress and a negative spiral of events and feelings. Excessive
focus by the patient on the penis as the dysfunctional unit may be associated with physical and psychological
problems in the female partner. With the advent of effective, well-tolerated treatments for erectile dysfunction,
including the phosphodiesterase type 5 (PDE5) inhibitor sildena®l citrate, the needs and expectations of patients and
their partners concerning their medications, their physicians and other factors have come into focus. In addition to
the effectiveness or tolerability of a medication, a number of nonmedical outcomes may in¯uence patients and their
partners when choosing between therapeutic modalities or pharmacotherapies. These include the spontaneity and
naturalness of the sexual encounter, as well as the treatment's acceptability to the sexual partner, onset/duration of
action and potential interactions with food or alcohol. Patients of different ages, marital statuses or cultures may
assign distinct values to each of these criteria. Couples should therefore be involved in formulating treatment plans
and afforded wide latitude when initially selecting therapy and/or deciding how, or whether, to take medications. For
the physician, erectile dysfunction represents an opportunity to diagnose and treat other comorbid diseases,
including hypertension, ischemic heart disease and diabetes.
# 2002 Published by Elsevier Science B.V.
Keywords: Apomorphine; Erectile dysfunction; Intracavernosal injection therapy; Male sexuality;
Phosphodiesterase type 5 inhibitors; Treatment outcome
marks to assess how expectations are being met .
The ideal tablet would be effective; safe; rapidly acting
In the 1980s, the only available treatment option for
and long-acting; unaffected by food, alcohol and other
the sexually challenged man was sex therapy, a pros-
drugs; and consistent with discreet, on-demand use and
thetic implant, a vacuum device or testosterone ther-
apy, which was often inappropriate. The advent of
With the advent of effective and well-tolerated oral
intracavernosal injection therapy (ICIT) enabled stoi-
therapies, a number of ED patients can expect their sex
cal couples to resume sexual relationships, but many
lives to be restored to normal. For many, the concept of
found such treatment painful and invasive. Despite
a tablet with proven proerectile ef®cacy in response
efforts to re®ne the procedures, more than half of
to sexual stimulation in about 70% of intercourse
the couples initiated on injection programs dropped
attempts (or patients), usually within 1 hour, would
out. According to certain literature reviews , about
15±22% of men in some clinical trials declined more
Notwithstanding the widespread use and notoriety of
than one trial injection of ICIT, and discontinuation
sildena®l, large segments of ED patients either do not
rates with treatment in clinical trials ranged from
come forward for treatment or discontinue therapy
approximately 40% after 3 months to as high as 70±
prematurely. For instance, in an Australian study
involving 62 general medical practices, 88% of men
In 1998, Eardley described the ` ideal'' tablet for
with ED failed to avail themselves of treatment, as did
erectile dysfunction (ED; providing bench-
about 75% in a European study Discontinuation
rates range from 36% when ED is managed in a
* Tel. 44-1-543-432-757; Fax: 44-1-543-433-303.
specialist clinic to 78% when care is initiated by
E-mail address: [email protected] (G.I. Hackett).
a primary-care physician (Data on ®le, Abbott, UK).
1569-9056/02/$ ± see front matter # 2002 Published by Elsevier Science B.V.
PII: S 1 5 6 9 - 9 0 5 6 ( 0 2 ) 0 0 1 1 2 - 4
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
changed the mindsets of many patients and their part-
ners. The availability of effective and well-tolerated
oral therapy taken as needed by men with ED enabled
many patients and their partners to expect treatment to
For many patients, the onset of erectile failure can be
catastrophic, depending on such factors as culture,
levels of physician and partner support, and age.
Reproduced from Eardley et al. with permission.
The patient's self-con®dence can also be eroded by
ED. Up to 51% of European men reported that erectile
dif®culties made them feel generally less con®dent in
In addition, discontinuation rates for ED treatment
life, according to a recent survey of 26,000 European
with sildena®l range from 29% at 5 months in sildena®l
and American men aged 40±60 years (Data on ®le,
responders to as high as 72% after 1 year These
data suggest that currently available therapies do not
In this survey, the impact of ED on self-con®dence
meet all patient and partner expectations, that insuf®-
was less marked in UK men than their counterparts in
cient advice and follow-up are being furnished by
other European countries. Moreover, only 41% of
physicians or that some combination of these
British men considered sex important to their relation-
factors serves to compromise patient compliance and
ships compared with 71% of respondents in Turkey.
Sixteen percent of UK respondents admitted concerns
over sexual problems, but only 4% remembered ever
being asked about sex by their family doctors, a ®nding
that ranked the United Kingdom as the lowest of the
seven countries studied. Only 36% of Britons felt that
Advances in the clinical management of erectile
their general practitioners should routinely ask about
insuf®ciency have been accompanied by a marked
sex compared with 70% of respondents in Turkey.
evolution of ED treatment objectives and patients'
expectations over the past ®ve decades (Before
2.1. What do patients expect of their physicians?
1960, when only surgery and natural remedies were
When presenting with a health problem, most
available, to the introduction of vacuum devices in the
patients would expect their primary-care physicians
1960s and penile implantation in the 1960s through
to be interested and initiate investigations of the
1970s, the modest aim of treatment was any improve-
problem and/or specialist referrals. When the problem
is ED, however, a number of patients are reluctant to
With the availability of ICIT in the 1980s and 1990s,
come forward, often for fear of embarrassing them-
an erection suf®cient for successful sexual intercourse
selves and/or their physicians. In a US survey
became a rational treatment goal. Finally, the introduc-
approximately 70% of respondents believed that their
tion of oral therapy with the phosphodiesterase type 5
physicians would either dismiss, or be uncomfortable
(PDE5) inhibitor sildena®l citrate has completely
discussing, their concerns about sexual dysfunction.
In the United Kingdom, men infrequently attend their
family physicians, and many patients may be surprised
when the physician discusses the associations between
ED and important medical conditions. A British survey
of 789 men and 979 women demonstrated that
sexual problems were associated with a range of social,
psychological and physical problems, particularly pros-
Erectile insuf®ciency represents an excellent oppor-
tunity for health interventions that may result in long-
term improvements in cardiovascular and overall health,
because ED may be a risk marker for, or the ®rst sign of,
occult coronary artery disease (CAD) or cardiovascular
Fig. 1. Changing treatment, changing mindset.
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
2.2. What do patients expect from their medications?
Several studies have looked at patient expectations
Reasons for sildena®l treatment discontinuation in 53 (30.9%) of 171
from ED therapy, and the results obtained have varied
according to what questions were asked and how they
were phrased. When devising a treatment plan, it is
important to leave the patient and partner wide latitude
for personal choice. Couples will assess the success of
any ED therapy largely on the basis of its ef®cacy and
tolerability, but a range of social, cultural, religious and
potentially incomprehensible reasons will help to
determine how a particular couple will take treatment
(e.g. frequency) or whether they will continue with the
Many patients are hoping for a cure, and most expect
that treatment will involve a tablet. Among 52 US
men of varying demographic and socioeconomic
a lifetime of medication taking. One recent UK study
pro®les, including ages ranging from 18 to 70 years
involving 260 consecutive patients addressed the
outcome variables valued by participants when
reasons for discontinuation of oral therapy with sil-
de®ning the success of ED treatment, in descending
dena®l 12 months after hospital clinic attendance
order of importance, were (1) cure, which was de®ned
by some patients as ``bringing back normal sexual
study population, or 11% of sildena®l patients who
intercourse''; (2) pleasure (e.g. ``sensation,'' ``orgasm
discontinued therapy, stopped treatment because their
is achieved''); (3) partner satisfaction with inter-
erections had returned to normal. This study was more
course; (4) reproduction (e.g. ``ability to ejaculate'');
likely to re¯ect the true reasons for discontinuation of
and (5) naturalness with reference to the temperature,
therapy than clinical trials, in which patients with
size, color and overall appearance of the penis during
high motivation may in effect be preselected and
administered greater quantities of medications for
This study also demonstrated that patients with
different demographic and socioeconomic character-
A total of 19% of 791 patients seen in an Argentinean
istics may attach distinct values to health outcome
clinic discontinued sildena®l therapy because of
variables when either deciding whether to use surgery,
recovery of erectile function. Finally, a majority of men
pharmacotherapy or vacuum devices as a treatment for
in a recent open-label study reported the return of
ED, or choosing between competing pharmacothera-
spontaneous erections over 12 months of treatment
pies. For instance, whereas men younger than 40 years
with self-injected prostaglandin E1 (PGE1).
were more concerned about the long-term conse-
quences of therapy, those over the age of 60 were
more concerned with immediate results .
Initially, men often focus on penile rigidity as their
main treatment objective. However, recent work by
A reliable and consistent erection for sexual activity
Riley in the United Kingdom demonstrated that
was rated as the highest priority in younger patients and
ED may be associated with sexual problems (e.g.
the second-most important among older men
urogenital atrophy) and relationship con¯ict in the
(Data on ®le, Lilly ICOS LLC). Among patients with
female partner (see below). Treatment outcomes are
severe ED, a PDE5 inhibitor is more likely to be
likely to be enhanced if the objectives of treatment are
oriented toward the restoration of a satisfying sexual
Where proerectile ef®cacy is high, other features
relationship rather than enhancing penile tumescence
of a given medication may be less important for
the majority of patients. For patients seeking a therapy
that confers reliable, consistent improvements in
erectile function, the physician should recommend
the drug that will, in his or her opinion, be most
effective, because repetitive treatment failures may
Finding a cure for ED was the central hope of
compromise the patient's outlook and compliance with
many younger men, as it would deliver them from
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
have advantages for couples who desire more sponta-
Clinicians often forget that ED therapy is prescribed
neous or more frequent sexual activity. As discussed by
to facilitate a pleasurable experience for a patient and
Prof. Porst elsewhere in this supplement, treatment
his partner. In younger men, pleasure is more likely to
with tadala®l enabled a majority of ED patients to
revolve around sexual performance and the rigidity of
experience successful intercourse at any time up to
penile erections, whereas, for older couples, vaginal
penetration may not be the main goal.
Safety concerns may in¯uence partner satisfaction,
The concept of pleasure is in¯uenced by not only age
and these concerns may be greater if a drug remains in
but also by ethnic, cultural, religious and even ®nancial
the bloodstream for several days. However, the pro-
factors. The search for a better sexual experience
longed plasma residence of tadala®l, which has a half-
frequently leads patients to try new therapies, even
life of 17.5 hours has not been associated with an
if the existing one seems to be effective. Such an
increase in the frequency or severity of adverse events
approach is virtually unique to therapies for sexual
reported with other (shorter-lived) PDE5 inhibitors,
dysfunction and may also be in¯uenced by the require-
according to large, multicenter, randomized, double-
ment of the patient to pay for treatment.
blind, placebo-controlled clinical trials .
The assessment of satisfaction with ED therapy is
Invasive therapies, such as ICIT and medicated
largely based on traditional methods such as the Inter-
urethral system for erection (MUSE1), are often less
national Index of Erectile Function (IIEF) Global
satisfying options for patients' partners. For instance,
Assessment Question (GAQ), Sexual Encounter Pro-
partners of MUSE patients may experience vaginal
®le (SEP) and Erectile Dysfunction Inventory of Treat-
burning or itching, although these symptoms may be
ment Satisfaction (EDITS) . However, more
manifestations of resuming sexual intercourse rather
sensitive measures of ejaculation and desire may be
than a direct consequence of transurethral PGE1 per se
required to establish a reliable index or de®nition of
The female partner may also resent or feel unin-
volved with the ``pharmacologically induced'' erection
associated with ICIT . Vacuum constriction is also
generally less satisfying to the female partner, although
Erectile dysfunction can adversely affect patients'
occasionally, her desire for the ED patient to avoid
sexual partners. In one study approximately 60%
medication use can result in selection of the vacuum
of women whose partners experienced ED reported a
device as the preferred treatment option. Apart from
diminished interest in sex compared with 29% of those
psychosexual counseling, vacuum devices represent
the least-invasive ED treatment alternative.
Many men who are resuming sexual activityÐespe-
Sexual satisfaction may be in¯uenced by a disparity
cially those in new relationships after bereavement or
in sexual desire between the man and his partner, and
divorceÐput themselves under extreme pressure to
health authorities have stressed the importance
satisfy a new partner. It may be necessary for these
of assessing potential sexual problems in the partner.
men not to inform their new partner that they are taking
The sexual history should evaluate the patient's and
therapy, at least until the relationship is established. In
partner's expectations and motivations concerning ED
such cases, a rapidly acting therapy, such as sublingual
therapy, and the effectiveness of therapy may be opti-
apomorphine, may be more appropriate than a drug such
mized by including both parties in formulating treat-
as sildena®l, as these men are more likely to complain
ment plans Vaginal dryness is the most common
about the need for premeditation associated with taking
partner problem unmasked when ED therapy is
the therapy 1 hour before planned sexual intercourse.
initiated. Fortunately, unlike a disparity in sexual
However, a recent study suggested that, among
desire, vaginal dryness is readily treatable.
the majority of men in stable relationships, such plan-
ning is a minor issue. Further, a randomized, double-
blind, placebo-controlled trial involving 247 ED
Among younger patients, reproduction is considered
outpatients showed that men who were treated with
an important issue in the treatment of ED erecti le
sildena®l, as well as their partners, exhibited signi®-
dif®culties, as well as premature ante portas and retro-
cantly higher levels of treatment satisfaction (accord-
grade ejaculation, are not uncommon causes of inferti-
ing to the EDITS) compared with their counterparts in
lity. Many patients for whom fertility is an issue expect
their physicians to show a high level of interest and offer
Agents with the potential for a longer duration of
clinical support, such as prescribing oral therapies for
action, such as tadala®l (a PDE5 inhibitor), may also
frequent use or medications for ejaculatory disorders
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
when indicated, as well as providing other, supportive
Among men under 40 years of age in the study by
Hanson-Divers et al. ``naturalness,'' or the degree
to which a treatment had a physiologic effect on the
body, was rated as moderately important when choos-
ing between pharmacotherapies for ED, but not more
important than the success associated with each drug
Oral therapy with a rapidly acting agent that potenti-
ates the physiologic erectile response to sexual stimu-
lation is more likely to ful®ll the requirement for
naturalness than MUSE1 or ICIT. The planning asso-
Fig. 2. Patient expectations. About half of the patients surveyed preferred
ciated with the use of an agent such as sildena®l, which,
not to plan their sexual activities. Data on ®le, Lilly ICOS LLC.
for optimal effectiveness, must be administered on an
empty stomach approximately 1 hour before sexual
intercourse, may not satisfy the patient's concept of a
ED and the likelihood that a newly presenting ED
natural erection and sexual encounter.
patient has undiagnosed IHD has been estimated at
In addition, a rapidly acting agent such as sublingual
apomorphine, whose pharmacokinetics are not affected
Case reports of myocardial infarction (MI) in silde-
by food intake, may also provide a more natural
na®l users together with avid coverage in popular
erection and be easier to use, but it must also be
media, have prompted concerns among many patients
effective and reliable. Of note, tadala®l has been
and their partners that resumption of sexual activity
administered in clinical trials without any instructions
while using oral ED therapy may be dangerous. Such
concerning timing of intercourse relative to dosing or
concerns need to be discussed openly with the ED
any restrictions regarding food or alcohol intake.
patient and his partner so that they understand that the
risk usually results from the underlying IHD and not
Younger men value spontaneity as a more important
Many patients will select sublingual apomorphine or
issue than men over 40 years of age, for whom sex is
ICIT because of concerns about MI with sildena®l.
more likely to be organized and scheduled into a busy
However, a number of men with severe IHD may be
work and family life, particularly when both partners
disappointed in the outcomes of therapy with sublin-
have careers. In some countries in the Middle and Far
gual apomorphine. In a recent randomized, double-
East, spontaneity and facility for multiple sexual
blind, placebo-controlled crossover study of 296
attempts may be important; among 460 Saudi Arabian
men with ED of various severities and etiologies, 42%
men with ED seen from 1991 to 1995, a lack of sexual
of attempts resulted in erections ®rm enough for sexual
spontaneity and naturalism accounted for 24% of pre-
intercourse among men with CAD who were treated
with sublingual apomorphine 3 mg for 4 weeks com-
A recent study of 30,000 men in six countries
pared to 28% with placebo; this difference was not
showed that approximately 50% of European and
statistically signi®cant, although the number of CAD
American men did not want to plan their sexual
patients was small (n 14). Consensus recommenda-
activities ((Data on ®le, Lilly ICOS LLC). If
tions can assist clinicians in risk-stratifying and coun-
approved by regulatory agencies, a longer-acting oral
seling ED patients with cardiovascular disease who are
drug such as tadala®l might have practical advantages
interested in resuming sexual activity and/or treatment
Administration of PDE5 inhibitors can amplify the
hypotensive effects of nitrates or nitric oxide donors,
with deleterious outcomes, and sildena®l is hence abso-
lutely contraindicated for concomitant use with these
A number of studies have clearly demonstrated an
association between ischemic heart disease (IHD) and
therapy is being considered, the prescribing physician
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
may stop nitrate therapy and/or change therapy to a drug
of nitrates that should not be overlooked in the medical
that in¯uences the prognosis of IHD rather than merely
treating its symptoms with nitrates. Analyses of large
clinical databases suggested that the overall
incidences of MI with either sildena®l or tadala®l were
Compared with men seeking treatment for largely
asymptomatic conditions (e.g. hypertension, hypercho-
lesterolemia), some ED patients might be expected to
assign a higher priority to therapies that enhance sexual
Compared with the reporting of adverse events in
function; such men might even be more willing to pay
randomized, controlled, clinical trials, side effects
out of pocket for ED treatment. For other patients who
tend to be reported less frequently in daily clinical
expect their ED therapies to be covered in the same
practice. Patients often tolerate side effects, including
way as interventions for other medical conditions,
headache, dyspepsia and ¯ushing with sildena®l,
issues such as private cost and medication rationing
because these effects are far outweighed by the gains
may have adverse effects on treatment compliance and
in erectile function obtained from effective treatment.
outcomes. The common practice of tablet splitting is
In general, ED therapies are well tolerated, with few
evidence that cost is a signi®cant issue.
Few population studies have surveyed patients about
Some patients will wish to try other medications to
the issue of cost. In a transitional Latin American econ-
avoid side effects. For instance, the centrally acting
omy, nearly one of every four sildena®l responders who
dopamine agonist apomorphine has a different
discontinued did so because of medication costs
mechanism of action and side-effect pro®le than those
whereas, in the United Kingdom, ®nancial reasons
of PDE5 inhibitors. Nausea, headache and dizziness
accounted for about 9% of sildena®l discontinuations
were among the predominant side effects seen in
. Whether the availability of treatment is regulated or
clinical trials with sublingual apomorphine In a
restricted by what the patient can or is willing to afford,
large, long-term European study involving ICIT,
costs can ultimately in¯uence patient expectations.
penile pain (occurring in 29% of patients), hematoma
Results with oral therapy are improved if the patient is
(33%), ®brotic changes (12%) and prolonged erection
exposed to multiple doses early in the course of ther-
apeutic regimens, but such regimens often prove to be
unsuccessful because patients cannot or will not pay for
them. Depending on post-registration costs, potentially
longer-acting drugs may represent improved values.
Much public concern has been expressed about
patients' ordering sildena®l over the Internet or
through newspaper advertisements. The common view
of such patients is that they are seeking performance
There are fundamental differences between treat-
enhancement, but it is likely that most of them have
ments for ED and other chronic diseases. The aim
mild ED and, like other men, resort to alternative drug-
of treating sexual problems in couples is to enable them
seeking behaviors to avoid consultations with their
to enjoy a satisfactory sexual experience. For these
reasons, simple or conventional considerations as to
Obtaining therapy through the Internet or other
whether one medication is more effective than another
alternative sources is probably a feature of modern
may be of little relevance to couples when selecting
consumerism and may, to some extent, be reinforced by
treatment. Many couples will experiment with different
the ED patient's knowledge that he will have to pay
therapies to see if the sexual experience is enhanced.
privately for his ED treatment irrespective of how it is
They may also decide that they want a variety of
obtained. Because many of these patients also have
experiences and may wish to alternate therapies. The
undiagnosed CAD, hypertension and/or diabetes,
couple will also decide, based on a number of social,
accessing them represents an important challenge.
cultural, religious and often incomprehensible reasons,
Clinicians should also be vigilant for occult, recrea-
how often they take therapy and when to discontinue
tional nitrate use in their patients who are taking PDE5
treatment. Consequently, physicians need a range of
inhibitors. Amyl nitrate ` poppers'' represent one source
therapies to satisfy these diverse patient needs.
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
[1] Hatzichristou DG, Apostolidis A, Tzortzis V, Ioannides E, Yanna-
[22] Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD,
koyorgos K, Kalinderis A. Sildena®l versus intracavernous injection
Wicker PA, for the Sildena®l Study Group. Oral sildena®l in
therapy: ef®cacy and preference in patients on intracavernous
the treatment of erectile dysfunction. N Engl J Med. 1998;328:
injection for more than 1 year. J Urol 2000;164:1197±200.
[2] Weiss JN, Badlani GH, Ravalli Curn R, Brettschneider Curn N.
[23] Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A.
Reasons for high drop-out rate with self-injection therapy for
The International Index of Erectile Function (IIEF): a multidimen-
impotence. Int J Impot Res 1994;6:171±4.
sional scale for assessment of erectile dysfunction. Urology 1997;49:
[3] Eardley I, Sethia K, Dean J. Erectile dysfunction: assessment and
management in primary care. London: Mosby-Wolfe Publications,
[24] Althof SE, Corty EW, Levine SB, et al. EDITS: development of
questionnaires for evaluating satisfaction with treatments for erectile
[4] Chew KK, Earle CM, Stuckey BG, Jamrozik K, Keogh EJ. Erectile
dysfunction. Urology 1999;53:793±9.
dysfunction in general medicine practice: prevalence and clinical
[25] Wagner G, Fugl-Meyer KS, Fugl-Meyer AR. Impact of erectile
correlates. Int J Impot Res 2000;12:41±5.
dysfunction on quality of life: patient and partner perspectives. Int J
[5] Meuleman EJ, Donkers LH, Robertson C, Keech M, Boyle P,
Klemeney LA. Erectile dysfunction: prevalence and effect on the
[26] Heaton J, Hackett GI, Savage D, Padley RJ. Patient choice is
quality of life: Boxmeer study. Ned Tijdschr Geneeskd 2001;145:
critical in managing erectile dysfunction. Eur Urol Suppl 2002;1(3):
[6] Hackett GI, Milledge D. A 12-month follow up of 260 patients
[27] Lewis R, Bennett C, Borkon W. Patient and partner satisfaction with
taking sildena®l. NHS clinical experience. In: Fourth Congress of the
European Society for Sexual and Impotence Research (ESSIR),
[28] Patterson B, Bedding A, Jewell H, Payne C, Mitchell M. Dose-
Rome, 30 September±3 October 2001 [poster 171].
normalized pharmacokinetics of tadala®l (IC351) administered as a
[7] Casabe A, Cobreros C, Bechara A, Roletto L, CheÂliz G, Hochman S.
single oral dose to healthy volunteers. Eur Urol Suppl 2002;1(1):152
Drop out reason in responders to sildena®l. Int J Impot Res
2001;13(Suppl 2):S5 [moderated poster 9].
[29] Brock GB, McMahon CG, Chen KK, Costigan T, Shen W, Watkins
[8] Viagra persistency rates. August 2000 to July 2001. Atlanta (GA):
V, Anglin G, Whitaker S. Ef®cacy and safety of tadala®l in the
treatment of erectile dysfunction: results of integrated analyses. J
[9] Hatzichristou DG. Sildena®l failures may be due to inadequate
instructions and follow-up: a study on 100 non-responders. Int J
[30] Padma-Nathan H, McMurray JG, Pullman WE, Whitaker JS, Saoud
Impot Res 2001;13:S32 [abstract 85].
JB, Ferguson KM. Rosen RC for the IC351 On-Demand Dosing
[10] Marwick C. Survey says patients expect little physician help on sex.
Study Group. On-demand IC351 (CialisTM) enhances erectile
function in patients with erectile dysfunction. Int J Impot Res
[11] Dunn K, Croft P, Hackett GI. Association of sexual problems with
social, psychological, and physical problems in men and women: a
[31] MUSE1 (alprostadil urethral suppository). VIVUS. In: Physicians'
cross-sectional population survey. J Epidemiol Comm Health 1998;
Desk Reference. 55th ed. Montvale (NJ): Medical Economics, 2001.
[12] O'Kane PD, Jackson G. Erectile dysfunction: is there silent
[32] NIH Consensus Development Panel on Impotence. Impotence. NIH
obstructive coronary artery disease? Int J Clin Pract 2001;55:219±20.
Consensus Conference. JAMA 1993;270:83±90.
[13] Kirby M, Jackson G, Betteridge J, Friedi K. Is erectile dysfunction a
[33] Jardin A, Wagner G, Khoury S, Giuliano F, Goldstein I, Padma-
marker for cardiovascular disease? Int J Clin Pract 2001;155:614±8.
Nathan H, editors. Recommendations of the First International
[14] Goldstein I. The mutually reinforcing triad of depressive symptoms,
Consultation on Erectile Dysfunction, cosponsored by the World
cardiovascular disease, and erectile dysfunction. Am J Cardiol 2000;
Health Organization (WHO). Plymouth: Health Publications Ltd.,
[15] Shabsigh R, Klein LT, Seidman S, Kaplan SA, Lehrhoff BJ, Ritter JS.
[34] Hanash KA. Comparative results of goal oriented therapy for erectile
Increased incidence of depressive symptoms in men with erectile
dysfunction. J Urol 1997;157:2135±8.
dysfunction. Urology 1998;52:848±52.
[35] MontorsiF, Salonia A, MontorsiP, et al. May erectile dysfunc-
[16] Burchardt M, Burchardt T, Anastasiadis AG, Kiss AJ, Shabsigh A,
tion predict ischemic heart disease? J Urol 2002;167(Suppl):148
De La Taille A, et al. Erectile dysfunction is a marker for
cardiovascular complications and psychological functioning in men
[36] Arora RR, Timoney M, Melilli L. Acute myocardial infarction after
with hypertension. Int J Impot Res 2001;13:276±81.
the use of sildena®l. N Engl J Med 1999;341:700.
[17] Buvat J, Lemaire A, Buvat-Herbaut M, Guieu JD, Bailleul JP, Fossati
[37] DeBusk R, Drory Y, Goldstein I, et al. Management of sexual
P. Comparative investigations in 26 impotent and 26 nonimpotent
dysfunction in patients with cardiovascular disease: recommenda-
diabetic patients. J Urol 1985;133:34±8.
tions of The Princeton Consensus Panel. Am J Cardiol 2000;86:
[18] Hanson-Divers C, Jackson E, Lue TF, Crawford SY, Rosen RC.
Health outcomes variables important to patients in the treatment of
[38] Webb DJ, Muirhead GJ, Wulff M, Sutton JA, Levi R, Dinsmore WW.
erectile dysfunction. J Urol 1998;159:1541±7.
Sildena®l citrate potentiates the hypotensive effects of nitric oxide
[19] Riley A. The role of the partner in erectile dysfunction and its
donor drugs in male patients with stable angina. J Am Coll Cardiol
treatment. Int J Impot Res 2002;14(Suppl 1):S105±9.
[20] Brock G, Tu LM, Linet OI. Return of spontaneous erection during
[39] Cheitlin MD, Hutter Jr AM, Brindis RG, Ganz P, Kaul S, Russell Jr
long-term intracavernosal alprostadil (Caverject) treatment. Urology
RO, et al. ACC/AHA expert consensus document. Use of sildena®l
(Viagra) in patients with cardiovascular disease. Circulation 1999;99:
[21] Dula E, Bukofzer S, Perdok R, George M, The Apomorphine SL
Study Group. Double-blind, crossover comparison of 3 mg
[40] Viagra1 (sildena®l citrate) prescribing information. P®zer. In:
apomorphine SL with placebo and with 4 mg apomorphine SL in
Physicians' Desk Reference. 55th ed. Montvale (NJ): Medical
male erectile dysfunction. Eur Urol 2001;39:558±64.
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
[41] Mittleman MA, Glasser DB, Orazem J, Collins M. Incidence of myo-
[43] Bukofzer S, Livesey N. Safety and tolerability of apomorphine SL
cardial infarction and death in 53 clinical trials of Viagra1 (sildena®l
(Uprima1). Int J Impot Res 2001;13(Suppl 3):S40±4.
citrate). J Am Coll Cardiol 2000;35(Suppl A):302 [abstract 807-6].
[44] Porst H, Buvat J, Meuleman E, Michal V, Wagner G. Intracavernous
[42] Kloner RA, Watkins VS, Costigan TM, Bedding A, Mitchell MI,
alprostadil alfadexÐan effective and well tolerated treatment for
Emmick J. Cardiovascular pro®le of tadala®l, a new PDE5 inhibitor. J
erectile dysfunction: results of a long-term European study. Int J
Urol 2002;167(Suppl):176 [abstract 707].
GERMAN ECONOMIC TEAM IN BELARUS 76 Zakharova Str., 220088 Minsk, Belarus. Tel./fax: +375 (17) 210 0105 E-mail: [email protected]. Internet: http://research.by/ Public Private Partnership Summary In recent decades governments in most industrial and developing countries promote co-operation between the public and private sectors in providing public goods. This cooperation takes the
Activity 2.1 1. Drug Dose Continuous data, i.e. you could inject 2.2ml or 2.211ml or 2.5ml 2. Hours slept Continuous data, i.e. you could sleep 9hrs, 9.5 hrs or 9.75 hrs 3. Movies watched Discrete data, i.e. you would have seen 5 or 6 movies not 6.5 movies 4. Clients seen in the past month Discrete data, i.e. you might have had 22 clients or 25 clients 5. Caffeine intake
 European Urology Supplements 1 (2002) 4±11
What Do Patients Expect from Erectile DysfunctionTherapy?Geoffrey I. Hackett*Good Hope Hospital, Sutton Cold®eld, Elford Road, Fisherwick, Lich®eld, Straffordshire WS 149JR, UK
Erectile insuf®ciency can precipitate emotional distress and a negative spiral of events and feelings. Excessive
focus by the patient on the penis as the dysfunctional unit may be associated with physical and psychological
problems in the female partner. With the advent of effective, well-tolerated treatments for erectile dysfunction,
including the phosphodiesterase type 5 (PDE5) inhibitor sildena®l citrate, the needs and expectations of patients and
their partners concerning their medications, their physicians and other factors have come into focus. In addition to
the effectiveness or tolerability of a medication, a number of nonmedical outcomes may in¯uence patients and their
partners when choosing between therapeutic modalities or pharmacotherapies. These include the spontaneity and
naturalness of the sexual encounter, as well as the treatment's acceptability to the sexual partner, onset/duration of
action and potential interactions with food or alcohol. Patients of different ages, marital statuses or cultures may
assign distinct values to each of these criteria. Couples should therefore be involved in formulating treatment plans
and afforded wide latitude when initially selecting therapy and/or deciding how, or whether, to take medications. For
the physician, erectile dysfunction represents an opportunity to diagnose and treat other comorbid diseases,
including hypertension, ischemic heart disease and diabetes.
European Urology Supplements 1 (2002) 4±11
What Do Patients Expect from Erectile DysfunctionTherapy?Geoffrey I. Hackett*Good Hope Hospital, Sutton Cold®eld, Elford Road, Fisherwick, Lich®eld, Straffordshire WS 149JR, UK
Erectile insuf®ciency can precipitate emotional distress and a negative spiral of events and feelings. Excessive
focus by the patient on the penis as the dysfunctional unit may be associated with physical and psychological
problems in the female partner. With the advent of effective, well-tolerated treatments for erectile dysfunction,
including the phosphodiesterase type 5 (PDE5) inhibitor sildena®l citrate, the needs and expectations of patients and
their partners concerning their medications, their physicians and other factors have come into focus. In addition to
the effectiveness or tolerability of a medication, a number of nonmedical outcomes may in¯uence patients and their
partners when choosing between therapeutic modalities or pharmacotherapies. These include the spontaneity and
naturalness of the sexual encounter, as well as the treatment's acceptability to the sexual partner, onset/duration of
action and potential interactions with food or alcohol. Patients of different ages, marital statuses or cultures may
assign distinct values to each of these criteria. Couples should therefore be involved in formulating treatment plans
and afforded wide latitude when initially selecting therapy and/or deciding how, or whether, to take medications. For
the physician, erectile dysfunction represents an opportunity to diagnose and treat other comorbid diseases,
including hypertension, ischemic heart disease and diabetes.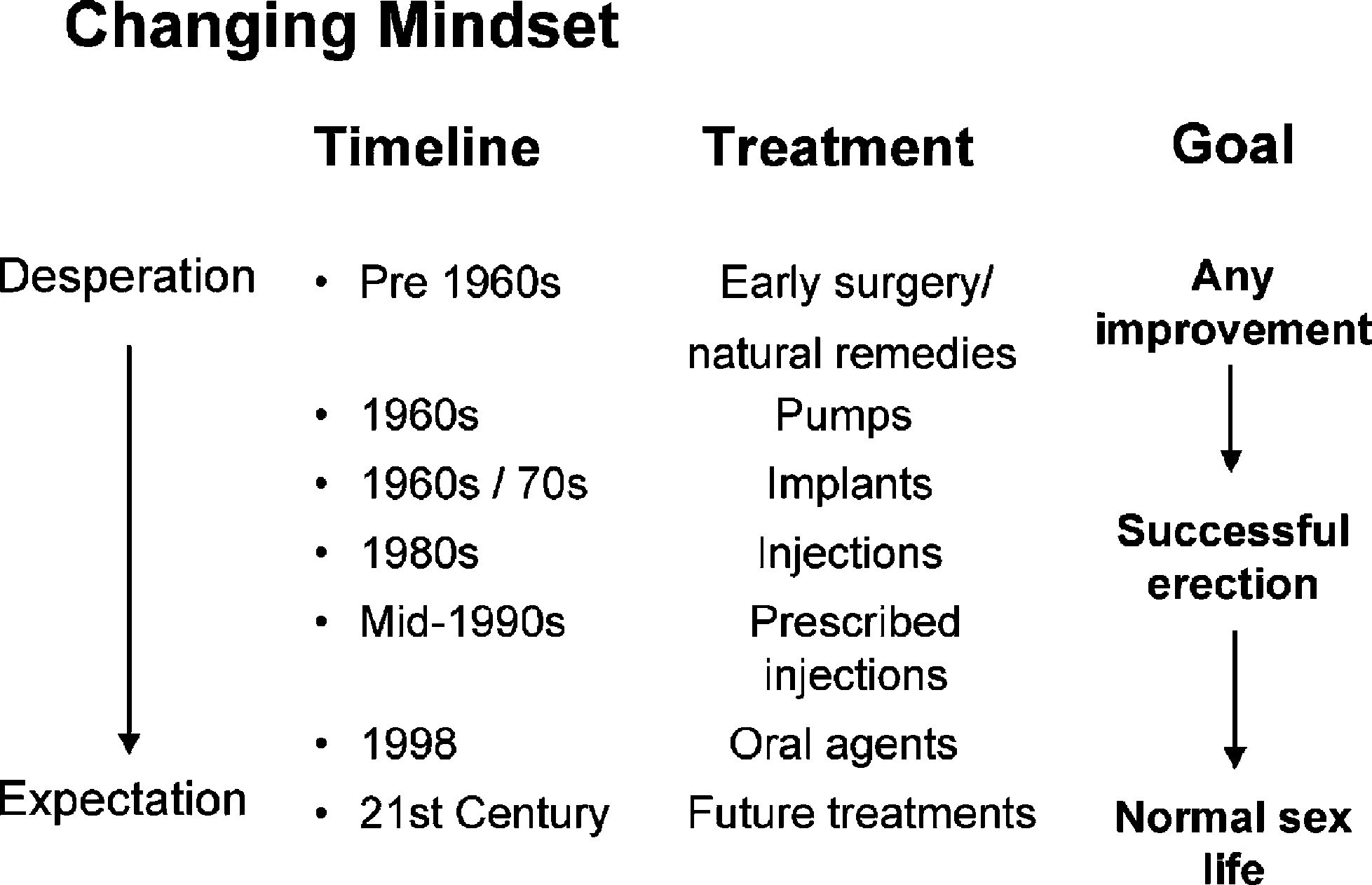 G.I. Hackett / European Urology Supplements 1 (2002) 4±11
changed the mindsets of many patients and their part-
ners. The availability of effective and well-tolerated
oral therapy taken as needed by men with ED enabled
many patients and their partners to expect treatment to
For many patients, the onset of erectile failure can be
catastrophic, depending on such factors as culture,
levels of physician and partner support, and age.
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
changed the mindsets of many patients and their part-
ners. The availability of effective and well-tolerated
oral therapy taken as needed by men with ED enabled
many patients and their partners to expect treatment to
For many patients, the onset of erectile failure can be
catastrophic, depending on such factors as culture,
levels of physician and partner support, and age.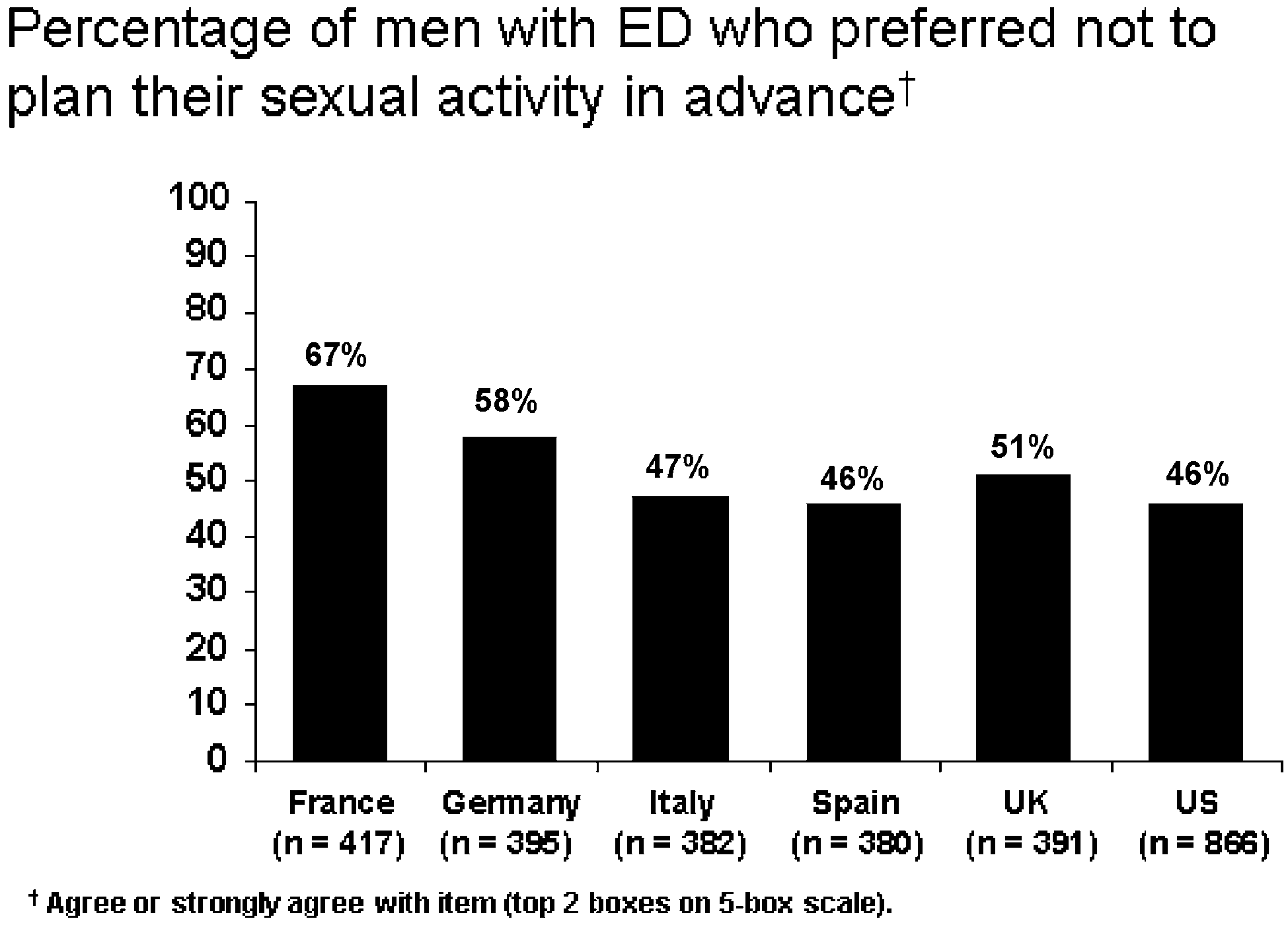 G.I. Hackett / European Urology Supplements 1 (2002) 4±11
when indicated, as well as providing other, supportive
Among men under 40 years of age in the study by
Hanson-Divers et al. ``naturalness,'' or the degree
to which a treatment had a physiologic effect on the
body, was rated as moderately important when choos-
ing between pharmacotherapies for ED, but not more
important than the success associated with each drug
Oral therapy with a rapidly acting agent that potenti-
ates the physiologic erectile response to sexual stimu-
lation is more likely to ful®ll the requirement for
naturalness than MUSE1 or ICIT. The planning asso-
Fig. 2. Patient expectations. About half of the patients surveyed preferred
ciated with the use of an agent such as sildena®l, which,
not to plan their sexual activities. Data on ®le, Lilly ICOS LLC.
G.I. Hackett / European Urology Supplements 1 (2002) 4±11
when indicated, as well as providing other, supportive
Among men under 40 years of age in the study by
Hanson-Divers et al. ``naturalness,'' or the degree
to which a treatment had a physiologic effect on the
body, was rated as moderately important when choos-
ing between pharmacotherapies for ED, but not more
important than the success associated with each drug
Oral therapy with a rapidly acting agent that potenti-
ates the physiologic erectile response to sexual stimu-
lation is more likely to ful®ll the requirement for
naturalness than MUSE1 or ICIT. The planning asso-
Fig. 2. Patient expectations. About half of the patients surveyed preferred
ciated with the use of an agent such as sildena®l, which,
not to plan their sexual activities. Data on ®le, Lilly ICOS LLC.