North Sydney Orthopaedic and Sports Medicine Centre
The meniscus is a commonly injured structure in the knee. The injury can occur in any age group. In younger people the meniscus is fairly tough and rubbery, and tears usually occur as a result of a fairly forceful twisting injury. In older people, the meniscus grows weaker with age, and meniscal tears may occur as a result of a fairly minor injury.
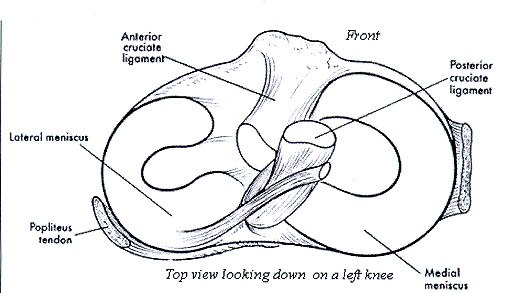
The meniscus is a half moon shaped piece of cartilage that lies between the weight bearing joint surfaces of the thigh and the shin, and is attached to the lining of the knee joint. There are two menisci in a normal knee; the outside one is called the lateral meniscus and the inner one is called the medial meniscus. The menisci play an important role as a shock absorber in the knee joint, protecting the cartilage that lies on the surface of the bones from impact. The cartilage surface is a tough, very slick material that allows the surfaces to slide against one another
without damage to either surface. This ability of the
meniscus to spread out the force on the joint surface
The most common problem caused by a torn meniscus is pain.
as we walk is important because it protects the
The pain may be felt along the joint line where the meniscus is
cartilage from excessive forces occurring in anyone
located or may be more vague and involve the whole knee.
area on the joint surface. Without the meniscus, the
Any twisting, squatting or impacting activities will pinch the
concentration of force into a small area on the
meniscus tear or flap and cause pain. Often the pain
cartilage can damage the surface, leading to
may improve with rest after the initial injury, but as soon as
degeneration over time. The menisci also cup the
aggressive activity is attempted the pain recurs.
joint surfaces of the thigh and therefore provide
some degree of stabilization to the knee.
Swelling of the joint may occur although meniscal tears by themselves usually don’t cause a large, tensely swollen knee.
Typically, low level swelling sets in the next day after the
injury and is associated with stiffness and limping.
There are two different mechanisms for tearing a meniscus.
If the torn portion of the meniscus is large enough, locking
Traumatic tears result from a sudden load being applied to
may occur. Locking simply refers to the inability to completely
the mensical tissue that is severe enough to cause the
straighten out the knee. Locking occurs when the fragment of
meniscal cartilage to fail and let go. These usually occur from
torn meniscus gets caught in the hinge mechanism of the
a twisting injury or a blow to the side of the knee that causes
knee, and will not allow the leg to straighten completely. The
the meniscus to be pushed against and compressed.
torn fragment actually acts like a wedge to prevent the joint
Degenerative meniscal tears are best thought of as a failure of
the meniscus over time. The meniscus becomes less elastic
There are long term effects of a torn meniscus as well. The
and complaint, and as a result may fail with only minimal
constant rubbing of the torn meniscus on the cartilage may
trauma (such as just getting down into a squat). Sometimes
cause wear and tear on the surface, leading to degeneration
there are no memorable injuries or violent events that can be
of the joint. The knee may swell with use and become stiff
and tight. This is usually because of fluid accumulating inside
Treatment: Initial treatment for a torn meniscus usually is directed towards reducing the pain and swelling in the knee. You may be asked to attend physiotherapy to reduce the pain and swelling and improve the range of movement. If the knee is locked and cannot be straightened out, surgery may be recommended as soon as reasonably possible to remove the torn portion that is caught in the knee joint. Once a meniscus is torn, it will most likely not heal on its own. If the symptoms continue, surgery will be required to either remove the torn portion of the meniscus or to repair the tear.
North Sydney Orthopaedic and Sports Medicine Centre
loading activities in order to prevent the onset of early
Meniscal surgery is done using the arthroscope. Small
incisions are made in the knee to allow the insertion of a
small TV camera into the joint. Through another small
incision, special instruments are used to remove the torn
Potential Complications related to surgery:
portion of meniscus while the arthroscope is used to see
As with all operations if at any stage anything seems amiss
it is better to call up for advice rather than wait and worry.
In some cases the meniscus tear can be repaired. Sutures
A fever, or redness or swelling around the line of the
are then placed into the torn meniscus until the tear is
wound, an unexplained increase in pain should all be
repaired. Repair of the meniscus is not possible in all cases.
brought to the attention of the Surgeon.
Young people with relatively recent meniscal tears are the most likely candidates for repair. Degenerative type tears in
• Pneumonia: Patients with a viral respiratory tract
older people are not usually repairable.
infection (common cold or flu) should inform the
Surgeon as soon as possible and will have their surgery
postponed until their chest is clear. Patients with a
• Healthy patients are admitted on the morning of their
history of asthma should bring their inhalers to hospital.
surgery. You should inform your Surgeon and Anaesthetist
of any medical conditions or previous medical treatment as
embolus: Although this complication is rare following
arthroscopic surgery, a combination of knee injury,
• It is extremely important that there are no cuts,
prolonged transport and immobilisation of the limb,
scratches, pimples or ulcers on your lower limb as this
smoking and the oral contraceptive pill or hormonal
greatly increases the risk of infection. Your surgery will be
replacement therapy all multiply to increase the risk. Any
postponed until the skin lesions have healed. You should
past history of thrombosis should be brought to the
not to shave or wax your legs for one week prior to surgery.
attention of the Surgeon prior to your operation. The
• After the operation you will be required to stay in
oral contraceptive pill, hormonal replacement therapy
hospital for the day. Overnight stay may be required due
and smoking should cease one week prior to surgery to
to the affects of the anaesthetic or an inability to manage
• Excessive bleeding resulting in a haematoma is
known to occur with patients taking aspirin or
operatively. A physiotherapist will supervise muscle
nonsteroidal anti-inflammatory drugs - such as Voltaren,
contractions, walking and weight bearing. Physiotherapy
Naprosyn or Indocid. They should be stopped at least
will continue on a daily basis following your surgery until
the dressings are removed 7-10 days following surgery.
• Surgery is carried out under strict germ free
Sedentary and office workers may return to work
conditions in an operating theatre. Antibiotics are
approximately 2-3 days following surgery. Most patients
administered intravenously at the time of your surgery.
should be walking normally 7 days following surgery
Any allergy to known antibiotics should be brought to the
although there is considerable patient to patient variation.
attention of your Surgeon or Anaesthetist. Despite these
• Should the left knee be involved then driving an
measures there is a less than 1 in 300 chance of
automatic car is possible as soon as pain allows. Should the
developing an infection within the joint. This may require
right knee be involved driving is permitted when you are
treatment with antibiotics or may require hospitalisation
able to walk without crutches. You must not drive a motor
and arthroscopic draining of the joint with intravenous
vehicle whilst taking severe pain killing medications.
antibiotics. Subsequent to such procedures prolonged
• Return to vigorous activities will be determined by the
periods of antibiotics are required and the post operative
extent of the damage to your meniscus and the amount of
meniscus that required removal. If minimal damage was
present then you may return to vigorous activities after 6 weeks. If significant damage was present then you may be
North Sydney Orthopaedic and Sports Medicine Centre
Q. How long does it take for the swelling to go away?
A. After 8 weeks most of the swelling should be gone.
A. Sedentary and office workers may return to work
approximately 2-5 days following surgery.
A. Yes, unless advised otherwise by Dr Roe.
A. You can travel domestically after 3 days and
A. Yes. You will need to bring these with you on the day of
your surgery and they can be organised through your own
physiotherapist or through your local chemist. We advise
patients to bring crutches for added support on the day.
A. This will vary depending on your surgical outcome.
Q. When do I see a physiotherapist after the surgery?
A. Physiotherapy is commenced immediately. Your
Q. When do I need to see Dr Roe after the surgery?
physiotherapist will supervise strengthening and walking.
A. You will return for removal of the superficial dressings
and a wound check at 7-10 days from surgery, then at the
Q. What medications should I cease prior to the surgery?
A. Any blood thinning medication should be stopped.
A. Driving an automatic car is possible as soon as pain
allows after left knee surgery. Should the right knee be
involved driving is permitted when you can walk
For any questions please do not hesitate in conta cting our staff at NSOSMC on (02) 9409 0500
Yolanda Armstrong (Personal Assistant), Dr Lucy Salmo n (Physiotherapist), Alison Waller (Physiotherapist)
Photochemistry and Photobiology, 2012, 88: 590–595Antimicrobial Photodynamic Therapy on Drug-resistant Pseudomonasaeruginosa-induced Infection. An In Vivo Study†Maria C. E. Hashimoto1, Renato A. Prates1, Ilka T. Kato1, Silvia C. NuMartha S. Ribeiro*11Center for Lasers and Applications, Institute of Energetic and Nuclear Researches, IPEN–CNEN ⁄ SP,2Institute of Health Researches, INPES-
Docteur François BOBIN Service ORL POLYCLINIQUE DE POITIERS 1 rue de la Providence 86035 Poitiers Cedex( + 33 (0)5 49 41 23 04( + 33 (0)5 49 61 72 50 L'oreille interne est fragile, quelques conseils pour la préserver. 1- Voici une liste des principales substances médicamenteuses ayant une toxicité potentielle pour l'oreille interne (même normale). Ne les prendre que s'il sont i
 North Sydney Orthopaedic and Sports Medicine Centre
The meniscus is a commonly injured structure in the knee. The injury can occur in any age group. In younger people the meniscus is fairly tough and rubbery, and tears usually occur as a result of a fairly forceful twisting injury. In older people, the meniscus grows weaker with age, and meniscal tears may occur as a result of a fairly minor injury.
The meniscus is a half moon shaped piece of cartilage that lies between the weight bearing joint surfaces of the thigh and the shin, and is attached to the lining of the knee joint. There are two menisci in a normal knee; the outside one is called the lateral meniscus and the inner one is called the medial meniscus. The menisci play an important role as a shock absorber in the knee joint, protecting the cartilage that lies on the surface of the bones from impact. The cartilage surface is a tough, very slick material that allows the surfaces to slide against one another
without damage to either surface. This ability of the
meniscus to spread out the force on the joint surface
The most common problem caused by a torn meniscus is pain.
as we walk is important because it protects the
The pain may be felt along the joint line where the meniscus is
cartilage from excessive forces occurring in anyone
located or may be more vague and involve the whole knee.
area on the joint surface. Without the meniscus, the
Any twisting, squatting or impacting activities will pinch the
concentration of force into a small area on the
meniscus tear or flap and cause pain. Often the pain
cartilage can damage the surface, leading to
may improve with rest after the initial injury, but as soon as
degeneration over time. The menisci also cup the
aggressive activity is attempted the pain recurs.
joint surfaces of the thigh and therefore provide
some degree of stabilization to the knee.
Swelling of the joint may occur although meniscal tears by themselves usually don’t cause a large, tensely swollen knee.
Typically, low level swelling sets in the next day after the
injury and is associated with stiffness and limping.
There are two different mechanisms for tearing a meniscus.
If the torn portion of the meniscus is large enough, locking
Traumatic tears result from a sudden load being applied to
may occur. Locking simply refers to the inability to completely
the mensical tissue that is severe enough to cause the
straighten out the knee. Locking occurs when the fragment of
meniscal cartilage to fail and let go. These usually occur from
torn meniscus gets caught in the hinge mechanism of the
a twisting injury or a blow to the side of the knee that causes
knee, and will not allow the leg to straighten completely. The
the meniscus to be pushed against and compressed.
torn fragment actually acts like a wedge to prevent the joint
Degenerative meniscal tears are best thought of as a failure of
the meniscus over time. The meniscus becomes less elastic
There are long term effects of a torn meniscus as well. The
and complaint, and as a result may fail with only minimal
constant rubbing of the torn meniscus on the cartilage may
trauma (such as just getting down into a squat). Sometimes
cause wear and tear on the surface, leading to degeneration
there are no memorable injuries or violent events that can be
of the joint. The knee may swell with use and become stiff
and tight. This is usually because of fluid accumulating inside
Treatment: Initial treatment for a torn meniscus usually is directed towards reducing the pain and swelling in the knee. You may be asked to attend physiotherapy to reduce the pain and swelling and improve the range of movement. If the knee is locked and cannot be straightened out, surgery may be recommended as soon as reasonably possible to remove the torn portion that is caught in the knee joint. Once a meniscus is torn, it will most likely not heal on its own. If the symptoms continue, surgery will be required to either remove the torn portion of the meniscus or to repair the tear.
North Sydney Orthopaedic and Sports Medicine Centre
The meniscus is a commonly injured structure in the knee. The injury can occur in any age group. In younger people the meniscus is fairly tough and rubbery, and tears usually occur as a result of a fairly forceful twisting injury. In older people, the meniscus grows weaker with age, and meniscal tears may occur as a result of a fairly minor injury.
The meniscus is a half moon shaped piece of cartilage that lies between the weight bearing joint surfaces of the thigh and the shin, and is attached to the lining of the knee joint. There are two menisci in a normal knee; the outside one is called the lateral meniscus and the inner one is called the medial meniscus. The menisci play an important role as a shock absorber in the knee joint, protecting the cartilage that lies on the surface of the bones from impact. The cartilage surface is a tough, very slick material that allows the surfaces to slide against one another
without damage to either surface. This ability of the
meniscus to spread out the force on the joint surface
The most common problem caused by a torn meniscus is pain.
as we walk is important because it protects the
The pain may be felt along the joint line where the meniscus is
cartilage from excessive forces occurring in anyone
located or may be more vague and involve the whole knee.
area on the joint surface. Without the meniscus, the
Any twisting, squatting or impacting activities will pinch the
concentration of force into a small area on the
meniscus tear or flap and cause pain. Often the pain
cartilage can damage the surface, leading to
may improve with rest after the initial injury, but as soon as
degeneration over time. The menisci also cup the
aggressive activity is attempted the pain recurs.
joint surfaces of the thigh and therefore provide
some degree of stabilization to the knee.
Swelling of the joint may occur although meniscal tears by themselves usually don’t cause a large, tensely swollen knee.
Typically, low level swelling sets in the next day after the
injury and is associated with stiffness and limping.
There are two different mechanisms for tearing a meniscus.
If the torn portion of the meniscus is large enough, locking
Traumatic tears result from a sudden load being applied to
may occur. Locking simply refers to the inability to completely
the mensical tissue that is severe enough to cause the
straighten out the knee. Locking occurs when the fragment of
meniscal cartilage to fail and let go. These usually occur from
torn meniscus gets caught in the hinge mechanism of the
a twisting injury or a blow to the side of the knee that causes
knee, and will not allow the leg to straighten completely. The
the meniscus to be pushed against and compressed.
torn fragment actually acts like a wedge to prevent the joint
Degenerative meniscal tears are best thought of as a failure of
the meniscus over time. The meniscus becomes less elastic
There are long term effects of a torn meniscus as well. The
and complaint, and as a result may fail with only minimal
constant rubbing of the torn meniscus on the cartilage may
trauma (such as just getting down into a squat). Sometimes
cause wear and tear on the surface, leading to degeneration
there are no memorable injuries or violent events that can be
of the joint. The knee may swell with use and become stiff
and tight. This is usually because of fluid accumulating inside
Treatment: Initial treatment for a torn meniscus usually is directed towards reducing the pain and swelling in the knee. You may be asked to attend physiotherapy to reduce the pain and swelling and improve the range of movement. If the knee is locked and cannot be straightened out, surgery may be recommended as soon as reasonably possible to remove the torn portion that is caught in the knee joint. Once a meniscus is torn, it will most likely not heal on its own. If the symptoms continue, surgery will be required to either remove the torn portion of the meniscus or to repair the tear.
 North Sydney Orthopaedic and Sports Medicine Centre
loading activities in order to prevent the onset of early
Meniscal surgery is done using the arthroscope. Small
incisions are made in the knee to allow the insertion of a
small TV camera into the joint. Through another small
incision, special instruments are used to remove the torn
Potential Complications related to surgery:
portion of meniscus while the arthroscope is used to see
As with all operations if at any stage anything seems amiss
it is better to call up for advice rather than wait and worry.
In some cases the meniscus tear can be repaired. Sutures
A fever, or redness or swelling around the line of the
are then placed into the torn meniscus until the tear is
wound, an unexplained increase in pain should all be
repaired. Repair of the meniscus is not possible in all cases.
brought to the attention of the Surgeon.
Young people with relatively recent meniscal tears are the most likely candidates for repair. Degenerative type tears in
• Pneumonia: Patients with a viral respiratory tract
older people are not usually repairable.
infection (common cold or flu) should inform the
Surgeon as soon as possible and will have their surgery
postponed until their chest is clear. Patients with a
• Healthy patients are admitted on the morning of their
history of asthma should bring their inhalers to hospital.
surgery. You should inform your Surgeon and Anaesthetist
of any medical conditions or previous medical treatment as
embolus: Although this complication is rare following
arthroscopic surgery, a combination of knee injury,
• It is extremely important that there are no cuts,
prolonged transport and immobilisation of the limb,
scratches, pimples or ulcers on your lower limb as this
smoking and the oral contraceptive pill or hormonal
greatly increases the risk of infection. Your surgery will be
replacement therapy all multiply to increase the risk. Any
postponed until the skin lesions have healed. You should
past history of thrombosis should be brought to the
not to shave or wax your legs for one week prior to surgery.
attention of the Surgeon prior to your operation. The
• After the operation you will be required to stay in
oral contraceptive pill, hormonal replacement therapy
hospital for the day. Overnight stay may be required due
and smoking should cease one week prior to surgery to
to the affects of the anaesthetic or an inability to manage
• Excessive bleeding resulting in a haematoma is
known to occur with patients taking aspirin or
operatively. A physiotherapist will supervise muscle
nonsteroidal anti-inflammatory drugs - such as Voltaren,
contractions, walking and weight bearing. Physiotherapy
Naprosyn or Indocid. They should be stopped at least
will continue on a daily basis following your surgery until
the dressings are removed 7-10 days following surgery.
• Surgery is carried out under strict germ free
Sedentary and office workers may return to work
conditions in an operating theatre. Antibiotics are
approximately 2-3 days following surgery. Most patients
administered intravenously at the time of your surgery.
should be walking normally 7 days following surgery
Any allergy to known antibiotics should be brought to the
although there is considerable patient to patient variation.
attention of your Surgeon or Anaesthetist. Despite these
• Should the left knee be involved then driving an
measures there is a less than 1 in 300 chance of
automatic car is possible as soon as pain allows. Should the
developing an infection within the joint. This may require
right knee be involved driving is permitted when you are
treatment with antibiotics or may require hospitalisation
able to walk without crutches. You must not drive a motor
and arthroscopic draining of the joint with intravenous
vehicle whilst taking severe pain killing medications.
antibiotics. Subsequent to such procedures prolonged
• Return to vigorous activities will be determined by the
periods of antibiotics are required and the post operative
extent of the damage to your meniscus and the amount of
meniscus that required removal. If minimal damage was
present then you may return to vigorous activities after 6 weeks. If significant damage was present then you may be
North Sydney Orthopaedic and Sports Medicine Centre
loading activities in order to prevent the onset of early
Meniscal surgery is done using the arthroscope. Small
incisions are made in the knee to allow the insertion of a
small TV camera into the joint. Through another small
incision, special instruments are used to remove the torn
Potential Complications related to surgery:
portion of meniscus while the arthroscope is used to see
As with all operations if at any stage anything seems amiss
it is better to call up for advice rather than wait and worry.
In some cases the meniscus tear can be repaired. Sutures
A fever, or redness or swelling around the line of the
are then placed into the torn meniscus until the tear is
wound, an unexplained increase in pain should all be
repaired. Repair of the meniscus is not possible in all cases.
brought to the attention of the Surgeon.
Young people with relatively recent meniscal tears are the most likely candidates for repair. Degenerative type tears in
• Pneumonia: Patients with a viral respiratory tract
older people are not usually repairable.
infection (common cold or flu) should inform the
Surgeon as soon as possible and will have their surgery
postponed until their chest is clear. Patients with a
• Healthy patients are admitted on the morning of their
history of asthma should bring their inhalers to hospital.
surgery. You should inform your Surgeon and Anaesthetist
of any medical conditions or previous medical treatment as
embolus: Although this complication is rare following
arthroscopic surgery, a combination of knee injury,
• It is extremely important that there are no cuts,
prolonged transport and immobilisation of the limb,
scratches, pimples or ulcers on your lower limb as this
smoking and the oral contraceptive pill or hormonal
greatly increases the risk of infection. Your surgery will be
replacement therapy all multiply to increase the risk. Any
postponed until the skin lesions have healed. You should
past history of thrombosis should be brought to the
not to shave or wax your legs for one week prior to surgery.
attention of the Surgeon prior to your operation. The
• After the operation you will be required to stay in
oral contraceptive pill, hormonal replacement therapy
hospital for the day. Overnight stay may be required due
and smoking should cease one week prior to surgery to
to the affects of the anaesthetic or an inability to manage
• Excessive bleeding resulting in a haematoma is
known to occur with patients taking aspirin or
operatively. A physiotherapist will supervise muscle
nonsteroidal anti-inflammatory drugs - such as Voltaren,
contractions, walking and weight bearing. Physiotherapy
Naprosyn or Indocid. They should be stopped at least
will continue on a daily basis following your surgery until
the dressings are removed 7-10 days following surgery.
• Surgery is carried out under strict germ free
Sedentary and office workers may return to work
conditions in an operating theatre. Antibiotics are
approximately 2-3 days following surgery. Most patients
administered intravenously at the time of your surgery.
should be walking normally 7 days following surgery
Any allergy to known antibiotics should be brought to the
although there is considerable patient to patient variation.
attention of your Surgeon or Anaesthetist. Despite these
• Should the left knee be involved then driving an
measures there is a less than 1 in 300 chance of
automatic car is possible as soon as pain allows. Should the
developing an infection within the joint. This may require
right knee be involved driving is permitted when you are
treatment with antibiotics or may require hospitalisation
able to walk without crutches. You must not drive a motor
and arthroscopic draining of the joint with intravenous
vehicle whilst taking severe pain killing medications.
antibiotics. Subsequent to such procedures prolonged
• Return to vigorous activities will be determined by the
periods of antibiotics are required and the post operative
extent of the damage to your meniscus and the amount of
meniscus that required removal. If minimal damage was
present then you may return to vigorous activities after 6 weeks. If significant damage was present then you may be
 North Sydney Orthopaedic and Sports Medicine Centre
Q. How long does it take for the swelling to go away?
A. After 8 weeks most of the swelling should be gone.
A. Sedentary and office workers may return to work
approximately 2-5 days following surgery.
A. Yes, unless advised otherwise by Dr Roe.
A. You can travel domestically after 3 days and
A. Yes. You will need to bring these with you on the day of
your surgery and they can be organised through your own
physiotherapist or through your local chemist. We advise
patients to bring crutches for added support on the day.
A. This will vary depending on your surgical outcome.
Q. When do I see a physiotherapist after the surgery?
A. Physiotherapy is commenced immediately. Your
Q. When do I need to see Dr Roe after the surgery?
physiotherapist will supervise strengthening and walking.
A. You will return for removal of the superficial dressings
and a wound check at 7-10 days from surgery, then at the
Q. What medications should I cease prior to the surgery?
A. Any blood thinning medication should be stopped.
A. Driving an automatic car is possible as soon as pain
allows after left knee surgery. Should the right knee be
involved driving is permitted when you can walk
For any questions please do not hesitate in conta cting our staff at NSOSMC on (02) 9409 0500
Yolanda Armstrong (Personal Assistant), Dr Lucy Salmo n (Physiotherapist), Alison Waller (Physiotherapist)
North Sydney Orthopaedic and Sports Medicine Centre
Q. How long does it take for the swelling to go away?
A. After 8 weeks most of the swelling should be gone.
A. Sedentary and office workers may return to work
approximately 2-5 days following surgery.
A. Yes, unless advised otherwise by Dr Roe.
A. You can travel domestically after 3 days and
A. Yes. You will need to bring these with you on the day of
your surgery and they can be organised through your own
physiotherapist or through your local chemist. We advise
patients to bring crutches for added support on the day.
A. This will vary depending on your surgical outcome.
Q. When do I see a physiotherapist after the surgery?
A. Physiotherapy is commenced immediately. Your
Q. When do I need to see Dr Roe after the surgery?
physiotherapist will supervise strengthening and walking.
A. You will return for removal of the superficial dressings
and a wound check at 7-10 days from surgery, then at the
Q. What medications should I cease prior to the surgery?
A. Any blood thinning medication should be stopped.
A. Driving an automatic car is possible as soon as pain
allows after left knee surgery. Should the right knee be
involved driving is permitted when you can walk
For any questions please do not hesitate in conta cting our staff at NSOSMC on (02) 9409 0500
Yolanda Armstrong (Personal Assistant), Dr Lucy Salmo n (Physiotherapist), Alison Waller (Physiotherapist)