He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Jem50w.indd
Elmer Press
Which Is the Best Treatment for Diabetes Complicated With
Severe Obesity, Intensive Insulin Therapy or Basal
Sumie Moriyamaa, c, Hidekatsu Yanaia, b, c, d
mg/day, and insulin glargine 24 units/day) reduced body
Letter to the Editor:
weight (from 92.1 to 86.0 kg) and HbA (from 10.3 to 9.2%)
after 9 months (Fig. 1). However, we decided to change the
Type 2 diabetes is commonly complicated with obesity. Al-
treatment from BOT to the GLP-1 analog (liraglutide) use,
though achieving a healthy weight and preventing weight
because her HbA level was still high. At this time, her body
gain are integral components of optimal diabetes manage-
weight was 86 kg and height 149 cm (BMI 38.7 kg/m2).
ment, an improvement of glycemic control with the treat-
As a result of the measurement using abdominal computed
ment usually induces weight gain [1]. Until now, we do not
tomography, abdominal circumference was 121.0 cm, while
exactly understand which treatment is the best for diabetes
subcutaneous fat area and visceral fat area were 374.5 and
complicated with severe obesity. We will show the changes
362.6 cm2 (Fig. 2), respectively, showing severe obesity. To
in body weight and glycemic control in a type 2 diabetic pa-
understand her insulin-dependence, a glucagon loading test
tient complicated with severe obesity, by the intensive insu-
and the measurement of daily urinary C-peptide (CPR) level
lin therapy (IIT), basal supported oral therapy (BOT), and
were performed. Serum fasting CPR level and serum CPR
level at 6 minutes after a glucagon loading were 1.28 and
A 60-year-old woman was referred and admitted to our
3.31 ng/ml, respectively, and urinary CPR level was 40.6 μg/
hospital due to poor blood glucose control in spite of the
day, which indicated that she has a suffi cient insulin secretion
treatment by IIT. At the age of 47 she was diagnosed as type
capacity. Therefore, we switched from BOT to the GLP-1
2 diabetes. For the last one year, she was treated with four
analog use. Switching to the GLP-1 analog (liraglutide 0.9
daily insulin injections: three injections of insulin aspart
mg/day) as monotherapy signifi cantly reduced body weight
before breakfast (14 units), lunch (14 units), and dinner (14
(from 86.0 to 77.0 kg) after fi ve months, and the addition of
units) and one of insulin detemir (18 units) at bedtime. Her
daily 1 mg of glimepiride to the GLP-1 analog signifi cantly
body weight was 92.1 kg and height 149 cm (BMI 41.5 kg/
reduced HbA (from 9.0 to 7.9%) (Fig. 1).
m2). Fasting plasma glucose (284 mg/dl) and HbA (NGSP
Therapeutic strategies to prevent or minimize weight
value, 10.3%) levels were signifi cantly elevated. Switching
gain, especially in obese diabetic patients, are very impor-
from IIT to BOT (glimepiride 1 mg/day, metformin 1,000
tant to help diabetic patients manage their glycemic control and keep or improve their quality of life. However, an in-tensive therapy is likely to induce weight gain. Weight gain was identifi ed as a sequela of IIT in the Diabetes Control and Complications Trial (DCCT), which is a multicenter controlled clinical trial designated to determine the effects of two different diabetes treatment regimens on complications
Manuscript accepted for publication October 12, 2011
of type 1 diabetic patients [2]. Higher baseline HbA levels
and greater decrements in HbA during intensive therapy
Department of Internal Medicine, National Center for Global Health
were both associated with greater weight gain in the DCCT.
and Medicine, Kohnodai Hospital, Ichikawa, Japan
In our patients, switching from IIT to BOT decreased daily
Clinical Research Center, National Center for Global Health and
Medicine, Kohnodai Hospital, Ichikawa, Japan
insulin use from 60 units to 24 units, which may be associ-
cSumie Moriyama and Hidekatsu Yanai contributed equally to this
ated with weight loss. BOT has been reported to minimize
weight gain compared with premixed insulin and prandial
insulin regimens [1], supporting our result.
The effects of liraglutide have been studied in the Lira-
glutide Effect and Action in Diabetes (LEAD). In the LEAD-5 study, liraglutide added to metformin and sulfonylurea
Articles The authors | Journal compilation J Endocrinol Metab and Elmer Press™ | www.jofem.org
Figure 1. The changes in body weight and HbA1c levels by the intensive insulin therapy (IIT), the basal supported oral therapy (BOT), and the glucagon-like peptide-1 (GLP-1) analog.
produced signifi cant improvements in glycemic control and
In conclusion, the GLP-1 analog use may be an excellent
body weight compared with placebo and insulin glargine [3].
therapeutic strategy for the diabetes management of type 2
In our patient, switching from BOT using insulin glargine to
diabetic patients who have suffi cient insulin secretion capac-
the GLP-1 analog use signifi cantly reduced body weight and
ity, complicated with severe obesity.
HbA level, showing an agreement with the result of LEAD-
5 study. GLP-1 is released into the blood from intestinal L-cells in response to meal ingestion. GLP-1 stimulates insu-
Acknowledgment
lin secretion from pancreatic ß-cells in a glucose-dependent manner, and slows gastric emptying, which may aid weight
This work was supported by the Grant of National Center for
loss and resulting amelioration in glycemic control [4].
Global Health and Medicine (22-120). Figure 2. Abdominal computed tomography. Red and blue areas indicate visceral fat and subcutaneous fat area, respectively.
Articles The authors | Journal compilation J Endocrinol Metab and Elmer Press™ | www.jofem.org
Best Treatment for Diabetes With Obesity
References
N, Antic S, Zdravkovic M, et al. Liraglutide vs insulin glargine and placebo in combination with metformin and
1. Davies M, Khunti K. Insulin management in overweight
sulfonylurea therapy in type 2 diabetes mellitus (LEAD-
or obese type 2 diabetes patients: the role of insulin
5 met+SU): a randomised controlled trial. Diabetologia.
glargine. Diabetes Obes Metab. 2008;10 Suppl 2:42-49.
2. Weight gain associated with intensive therapy in the
4. Kjems LL, Holst JJ, Volund A, Madsbad S. The infl u-
diabetes control and complications trial. The DCCT Re-
ence of GLP-1 on glucose-stimulated insulin secretion:
search Group. Diabetes Care. 1988;11(7):567-573.
effects on beta-cell sensitivity in type 2 and nondiabetic
3. Russell-Jones D, Vaag A, Schmitz O, Sethi BK, Lalic
subjects. Diabetes. 2003;52(2):380-386.
Articles The authors | Journal compilation J Endocrinol Metab and Elmer Press™ | www.jofem.org
Clinical Review Complementary and alternative medicine for the treatment of type 2 diabetes Richard Nahas MD CCFP Matthew Moher Abstract the most prevalent and fastest grow-ing diseases in Canada, responsible OBJECTIVE To review clinical evidence supporting complementary and for expenditures of 9 billion dollars per alternative medicine interventions for improving glycemic co
Beeld; 26 May 2009 (English translation) ‘Box’ just might be nicotine’s killer, Say farewell to cigarettes A new machine that helps relieve the withdrawal symptoms of addicts is being tested. Sonja van Buul experienced it in person. I am fed up. I’m a cigarette smoker and I’ve decided to quit smoking, right now whilst testing a new “wonder machine”. Because I know how bad sm
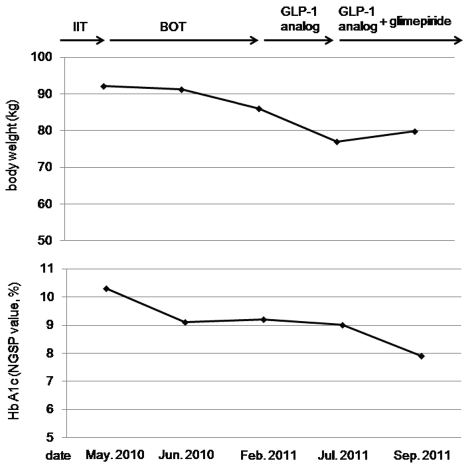
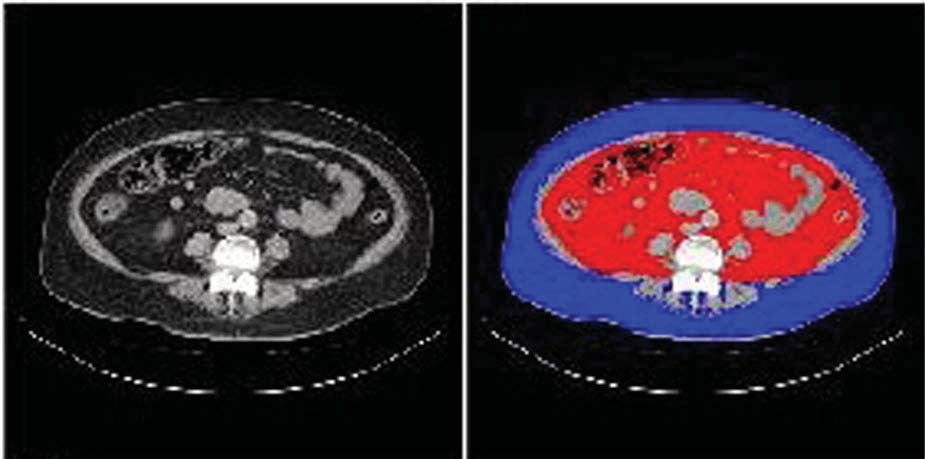 Figure 1. The changes in body weight and HbA1c levels by the intensive insulin therapy
Figure 1. The changes in body weight and HbA1c levels by the intensive insulin therapy