He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Graftonlitho.ie
Wound dressings
Vanessa Jones, Joseph E Grey and Keith G Harding
Updated information and services can be found at:
References
1 online articles that cite this article can be accessed at:
Rapid responses
One rapid response has been posted to this article, which you can access forfree at: You can respond to this article at:
Email alerting
Receive free email alerts when new articles cite this article - sign up in the
box at the top right corner of the article
Topic collections
Articles on similar topics can be found in the following collections
To order reprints of this article go to:
This is the ninth in a series of 12 articles Wound dressings Vanessa Jones, Joseph E Grey, Keith G Harding
Traditionally wet-to-dry gauze has been used to dress wounds. Modern dressing technology is based on the principle of
Dressings that create and maintain a moist environment,
creating and maintaining a moist wound environment
however, are now considered to provide the optimal conditionsfor wound healing. Moisture under occlusive dressings not onlyincreases the rate of epithelialisation but also promotes healing
Characteristics of the ideal dressing
through moisture itself and the presence initially of a lowoxygen tension (promoting the inflammatory phase). Gauze
x Capable of maintaining a high humidity at the wound site while
does not exhibit these properties; it may be disruptive to the
x Free of particles and toxic wound contaminants
healing wound as it dries and cause tissue damage when it is
removed. It is not now widely used in the United Kingdom.
x Capable of protecting the wound from further trauma
Occlusive dressings are thought to increase cell proliferation
x Can be removed without causing trauma to the wound
and activity by retaining an optimum level of wound exudate,
which contains vital proteins and cytokines produced in
response to injury. These facilitate autolytic debridement of the
wound and promote healing. Concerns of increased risk of
infection under occlusive dressings have not been substantiated
in clinical trials. This article describes wound dressings currently
Low adherent dressings—suitable for use on flat, shallow Low adherent dressings wounds with low exudates
Low adherent dressings are cheap and widely available. Their
Tulles—Bactigras, Jelonet, Paranet, Paratulle, Tullegras, Unitulle,
major function is to allow exudate to pass through into a
Textiles—Atrauman, Mepilex, Mepitel, NA Dressing, NA Ultra,
secondary dressing while maintaining a moist wound bed.
Most are manufactured in the form of tulles, which are open
weave cloth soaked in soft paraffin or chlorhexidine; textiles; ormultilayered or perforated plastic films.
They are designed to reduce adherence at the wound bed
and are particularly useful for patients with sensitive or fragileskin. Semipermeable films
Semipermeable films were one of the first major advances in
Left: Healthy venous leg ulcer suitable for dressing with low adherent
wound management and heralded a major change in the way
dressing. Right: Wound suitable for dressing with semipermeable film
wounds were managed. They consist of sterile plastic sheets ofpolyurethane coated with hypoallergenic acrylic adhesive and
Semipermeable films
are used mainly as a transparent primary wound cover.
Examples include Bioclusive, Mefilm, OpSite Flexigrid,* OpSite Plus,
Although they are impermeable to fluids and bacteria, they
are permeable to air and water vapour, the control of which is
x Suitable for flat, shallow wounds with low to medium exudates
dependent on the moisture and vapour transmission rate, which
varies depending on the brand. It is through this mechanism
x Adhere to healthy skin but not to wound
that this dressing creates a moist wound environment.
Films are very flexible and are good for wounds on
“difficult” anatomical sites—for example, over joints. They are
unable to cope with large amounts of exudate, however, and
x Not for infected or heavily exuding wounds
may cause maceration of the skin surrounding the wound bed if
*Not available on prescription in UK primary care. Hydrocolloids
Sodium carboxymethylcellulose, gelatin, pectin, elastomers, andadhesives are bonded to a carrier of semipermeable film or afoam sheet to produce a flat, occlusive, adhesive dressing thatforms a gel on the wound surface, promoting moist woundhealing. Cross linkage of the materials used influences the
Venous leg ulcer suitable
viscosity of the gel under the dressing. This gel, which may be
for dressing with
yellow and malodorous, may be mistaken for infection by the
hydrocolloid BMJ VOLUME 332 1 APRIL 2006
unwary. Hydrocolloids are virtually impermeable to water
Hydrocolloid dressings (including hydrofibres)
vapour and air and can be used to rehydrate dry necrotic escharand promote autolytic debridement. They are reported to
Type of dressing
reduce wound pain, and their barrier properties allow the
patient to bathe or shower and continue with normal daily
activities without disturbing or risking contamination of the
wound. Caution should be exercised when using hydrocolloids
for wounds that require frequent inspection—for example, for
Hydrocolloid fibres are now available in the form of a
hydrophilic, non-woven flat sheet, referred to as hydrofibre
dressings. On contact with exudate, fibres are converted from a
Useful in flat wounds, cavities, sinuses,
dry dressing to a soft coherent gel sheet, making them suitable
for wounds with a large amount of exudate.
high exudate wounds; highlyabsorbent; non-adherent; may be leftin place for several days; needssecondary dressing
*Not available on prescription in UK primary care. Foot wound complicated by Hydrocolloid fibres (hydrofibres) are often used on heterotopic calcification wounds where, traditionally, alginates have been used suitable for dressing with hydrofibres Hydrogels Hydrogels
Hydrogels consist of a matrix of insoluble polymers with up to
Examples include Aquaform, Intrasite, GranuGel, Nu-Gel, Purilon,
96% water content enabling them to donate water molecules to
the wound surface and to maintain a moist environment at the
x Supply moisture to wounds with low to medium exudate
x Suitable for sloughy or necrotic wounds
wound bed. As the polymers are only partially hydrated,
x Useful in flat wounds, cavities, and sinuses
hydrogels have the ability to absorb a degree of wound exudate,
the amount varying between different brands. They transmit
moisture vapour and oxygen, but their bacterial and fluid
permeability is dependent on the type of secondary dressingused.
Hydrogels promote wound debridement by rehydration of
non-viable tissue, thus facilitating the process of naturalautolysis. Amorphous hydrogels are the most commonly usedand are thick, viscous gels.
Hydrogels are considered to be a standard form of
management for sloughy or necrotic wounds. They are notindicated for wounds producing high levels of exudate or wherethere is evidence of gangrenous tissue, which should be kept
Dry, sloughy leg wound
dry to reduce the risk of infection. suitable for dressing with hydrogel Alginates Alginates
Alginates are produced from the naturally occurring calcium
Examples include Algisite, Algosteril, Kaltostat,* Melgisorb, SeaSorb,
and sodium salts of alginic acid found in a family of brown
seaweed (Phaeophyceae). They generally fall into one of two
x Useful in cavities and sinuses, and for undermining wounds
kinds: those containing 100% calcium alginate or those that
contain a combination of calcium with sodium alginate, usually
Alginates are rich in either mannuronic acid or guluronic
*Not available on prescription in UK primary care
acid, the relative amount of each influencing the amount ofexudate absorbed and the shape the dressing will retain. Alginates partly dissolve on contact with wound fluid to form ahydrophilic gel as a result of the exchange of sodium ions inwound fluid for calcium ions in the dressing. Those high inmannuronic acid (such as Kaltostat) can be washed off thewound easily with saline, but those high in guluronic acid (suchas Sorbsan) tend to retain their basic structure and should beremoved from the wound bed in one piece. Diabetic foot ulcer with maceration to
Alginates can absorb 15 to 20 times their weight of fluid,
surrounding skin suitable
making them suitable for highly exuding wounds. They should
for dressing with alginate BMJ VOLUME 332 1 APRIL 2006
not be used, however, on wounds with little or no exudate as
The ion exchange properties of some alginates make
they will adhere to the healing wound surface, causing pain and
them useful haemostatic agents, and as such they are particularly useful for postoperative wound packing Foam dressings Foam dressings
Foam dressings are manufactured as either a polyurethane or
Type of dressing
silicone foam. They transmit moisture vapour and oxygen and
Adhesive sheets: Allevyn Adhesive,
provide thermal insulation to the wound bed. Polyurethane
foams consist of two or three layers, including a hydrophilic
wound contact surface and a hydrophobic backing, making
them highly absorbent. They facilitate uniform dispersion of
exudate throughout the absorbent layer and prevent exterior
leakage (strike-through) due to the presence of a
Non-adherent sheets: Allevyn,* Allevyn
Polyurethane foam dressings are also available as a cavity
dressing—small chips of hydrophilic polyurethane foamenclosed in a membrane of perforated polymeric film, giving a
*Not available on prescription in UK primary care.
Silicone foams consist of a polymer of silicone elastomer
derived from two liquids, which, when mixed together, form afoam while expanding to fit the wound shape forming a softopen-cell foam dressing. The major advantage of foam is theability to contain exudate. In addition, silicone foam dressingsprotect the area around the wound from further damage. Venous leg ulceration in background of chronic oedema Antimicrobial dressings suitable for dressing with foam
Silver, in ionic or nanocrystalline form, has for many years beenused as an antimicrobial agent particularly in the treatment ofburns (in the form of silver sulfadiazine cream). The recentdevelopment of dressings impregnated with silver has widenedits use for many other wound types that are either colonised orinfected.
Iodine also has the ability to lower the microbiological load
in chronic wounds. Clinically it is mainly used in one of twoformats: (a) as povidone-iodine (polyvinylpyrrolidone-iodinecomplex), an iodophor (a compound of iodine linked to anon-ionic surfactant), which is produced as an impregnated
Top left: Sloughy, infected
tulle; and (b) as cadexomer iodine (a three dimensional starch
arterial ulcer suitable for
lattice containing 0.9% iodine). Cadexomer iodine has good
dressing with compound
absorptive properties: 1 g of cadexomer iodine can absorb up
antimicrobial dressing (silver
to 7 ml of fluid. As fluid is absorbed, iodine is slowly released,
or iodine based). Top right: Gangrenous foot suitable for
reducing the bacterial load and also debriding the wound of
dressing with antimicrobial
debris. This mode of action facilitates the delivery of iodine over
iodine impregnated dressing.
a prolonged period of time—thus, in theory, maintaining a
Left: Malodorous malignant melanoma ulcer suitable for
constant level of iodine in the wound bed. treatment with topical
Caution is required in patients with a thyroid disease owing
metronidazole
to possible systemic uptake of iodine. For this reason, thyroidfunction should be monitored in patients who are treated withiodine dressings. Antimicrobial dressings
Metronidazole gel is often used for the control of odour
caused by anaerobic bacteria. This is particularly useful in the
management of fungating malignant wounds. It may be used
alone or as an adjunct to other dressings. Unwanted effects of dressings
Maceration of the skin surrounding a wound may occur if a
dressing with a low absorptive capacity is used on a heavilyexuding wound. If the dressing is highly absorptive then morefrequent dressing changes may be needed, in addition to
Inappropriate use of dressings may lead to
investigation and management of the cause of the exudate
unwanted effects BMJ VOLUME 332 1 APRIL 2006
The skin surrounding a highly exuding wound may be
further protected through the use of emollients (such as 50:50mix of white soft paraffin and liquid paraffin) or the applicationof barrier films (such as Cavilon). Conversely, use of a highlyabsorptive dressing on a dry wound may lead to disruption ofhealthy tissue on the wound surface and cause pain whenremoved.
Allergic reactions are not uncommon: the dressing should
be avoided, and the allergy may need to be treated with potenttopical steroids. Tapes used to keep dressings in place arecommon causes of allergy. Many dressings require secondarydressings—for example, padding on highly exuding
Abdominoperineal resection wound treated with vacuum
wounds—which may make them bulky. Secondary dressings
assisted closure. The skin edges are protected with a barrier
should not be too tight, especially on patients with peripheral
cream to prevent maceration Further reading
x Choucair M, Phillips T. A review of wound healing and dressings
material. Skin and Aging 1998;6:(suppl):37-43.
x Hermans MH, Bolton LL. Air exposure versus occlusion: merits
and disadvantages of different dressings. J Wound Care1993;2:362-5.
x Morgan DA. Wound management products in the drug tariff. Pharmaceutical Journal 1999;263:820-5. Left: Allergy to dressing used to treat arterial leg ulceration. Note
x Thomas S, Leigh IM. Wound dressings. In: Leaper DJ, Harding KG,
erythematous skin with sharply demarcated edges corresponding to the
eds. Wounds: biology and management. Oxford: Oxford University
shape of the offending dressing. Right: Ulceration over the anterior aspect of the ankle caused by inappropriately tight bandage
x Turner TD. Development of wound management products in
chronic wound care. In: Krasner D, Rodeheaver G, Sibbald RG, eds. Chronic wound care: a clinical source book for healthcare professionals. 3rd ed. Wayne, PA: HMP Communications, 2001.
x Winter G. Formation of scab and the rate of epithelialisation of
Vanessa Jones is senior lecturer at the Wound Healing Research Unit,
superficial wounds in the skin of the young domestic pig. Nature
The ABC of wound healing is edited by Joseph E Grey
x Vermeulen H, Ubbink D, Goossens A, de Vos R, Legemate D.
([email protected]), consultant physician,
Dressings and topical agents for surgical wounds healing by
University Hospital of Wales, Cardiff and Vale NHS Trust, Cardiff, and
secondary intention. Cochrane Database Syst Rev
honorary consultant in wound healing at the Wound Healing
Research Unit, Cardiff University, and by Keith G Harding, director ofthe Wound Healing Research Unit, Cardiff University, and professorof rehabilitation medicine (wound healing) at Cardiff and Vale NHSTrust. The series will be published as a book in summer 2006.
Competing interests: For series editors’ competing interests, see the firstarticle in this series. “Seeing” is believing
“Your next batch of students arrive tomorrow,” the administrator
positive and inspirational impact on the team, and “the trio”
told me, “and one of them has a visual impairment.”
became instantly recognisable in the hospital.
It turned out that 20 years previously he had had retinitis
He relied on innovative ways to overcome his disability. For his
pigmentosa diagnosed, and by the time he joined medical school
medical boards (equivalent to MRCP), he used a reader and
he was registered blind. My colleagues were sceptical about his
scribe. During the anatomy exam, his palpation skills helped him
choice of profession, and we pondered how best to deal with this
to identify various parts on the cadaver. Since he had become
situation and what impact his presence would have on the rest of
blind in adulthood, he did not read Braille and instead consulted
audiobooks and e-text. The most amazing development has been
I met him the next day. Tall and elegant, he radiated a calm
JAWS, a computer program that allows him to “write” case notes,
confidence. Accompanying him every step of the way was his
search the internet, and respond to emails.
guide dog, and a fellow medical student relayed the case notes to
I had great respect and admiration for this remarkable medical
him (forming “the trio,” as I soon called them). His history taking
student and indicated that to him at our last meeting. To
skills turned out to be excellent, and he was able to extract
overcome such personal hardship and, against all odds, choose to
important information that had been missed by earlier students.
study medicine required strength of character and conviction that
He picked up all the findings on palpation and auscultation. The
many of us lack. He graduated recently and is now training to be
hepatic bruit is a specific sign of alcoholic hepatitis but can be
a psychiatrist. Before I met him, if someone had asked my
difficult to hear even for experienced hepatologists—but he never
opinion about a blind student training to be a doctor, I would nothave been optimistic. I guess “seeing” is believing.
missed one. During ward rounds, I was impressed by how well heconnected with his patients and how comfortable they seemed
Sumita Verma locum consultant, liver and antiviral unit, St Mary’s
with him. It was soon apparent that his presence was having a
Hospital NHS Trust, London ([email protected])BMJ VOLUME 332 1 APRIL 2006
 Wound dressings
Wound dressings 

 This is the ninth in a series of 12 articles
This is the ninth in a series of 12 articles

 unwary. Hydrocolloids are virtually impermeable to water
Hydrocolloid dressings (including hydrofibres)
unwary. Hydrocolloids are virtually impermeable to water
Hydrocolloid dressings (including hydrofibres)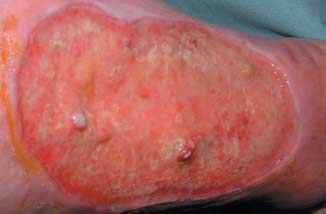


 not be used, however, on wounds with little or no exudate as
The ion exchange properties of some alginates make
not be used, however, on wounds with little or no exudate as
The ion exchange properties of some alginates make

 The skin surrounding a highly exuding wound may be
further protected through the use of emollients (such as 50:50mix of white soft paraffin and liquid paraffin) or the applicationof barrier films (such as Cavilon). Conversely, use of a highlyabsorptive dressing on a dry wound may lead to disruption ofhealthy tissue on the wound surface and cause pain whenremoved.
The skin surrounding a highly exuding wound may be
further protected through the use of emollients (such as 50:50mix of white soft paraffin and liquid paraffin) or the applicationof barrier films (such as Cavilon). Conversely, use of a highlyabsorptive dressing on a dry wound may lead to disruption ofhealthy tissue on the wound surface and cause pain whenremoved.