He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Microsoft word - removal of pharmaceuticals_word2003.doc
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008 Removal of selected pharmaceuticals from sewage water by advanced treatment techniques
1TU Bergakademie Freiberg, Institut für Biowissenschaften, Leipziger Str. 29, 09599 Freiberg,
Abstract
The presence of pharmaceuticals as trace pollutants in natural surface water bodies, ground water and
drinking water has recently led to some concern. Since sewage is the main source of this type of
pollution, some attempts have been made to remove pharmaceuticals by advanced physical, chemical
and biological techniques which go further than the conventional treatment. A few of these methods
reported recently were discussed in this paper on the example of the selected pharmaceuticals
Diclofenac, Ibuprofen, Carbamazepine, Clofibric Acid, Sulfamethoxazole, Iopromide and Metoprolol.
The advanced methods improved the removal of several of these substances to some extent, while few
compounds like the contrast agent Iopromide or the antiepileptic drug Carbamazepine proved to be
extraordinary persistent in some treatment processes. None of the techniques could guarantee a
hundred percent removal and questions about possible toxic by-products and the behaviour of
Introduction
Water is not only the most important food source of human beings but also an important habitat. So,
one has to concern about the quality of surface and ground water and as well as about adverse effects
of effluents introduced there. The impact and removal of conventional pollutants, such as persistent
organic pollutants (POPs) was in focus for the last decades and so their behaviour is well understood
(Jones et al. 2005). On the other side very little is known about the behaviour of trace pollutants yet,
which are present in the environment in extremely low concentrations (Jones et al. 2005; Fent et al.
Pharmaceuticals are an example for the variety of man-made trace pollutants (like personal care
products, musk fragrances or pesticides) that are introduced in surface or subsurface water bodies.
They have been found in a number of sewage treatment plant (STP) effluents, surface waters,
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
seawaters, ground waters and even in drinking water (Fent et al. 2006; Jones et al. 2005). Following
the precautionary principle both some legal action and advanced water purification are needed, to deal
But are pharmaceuticals in natural and drinking water really a problem? Many authors indicate that
these compounds are found in effluents and natural waters only in traces in the µg/l- or even in the
ng/l-range, respectively (Jones et al. 2005; Wiegel et al. 2004; Ternes et al. 2003). There should be
only a minor probability of negative effects on human beings due to the concentrations far below the
effect concentrations of the pharmaceuticals. On the other hand, only little information is available
about possible effects on non-target organisms. In addition, one has to consider that STP effluents
contain a complex drug cocktail, by which additional or synergistic effects can not be excluded.
Moreover, the existence of occurring metabolites of some compounds has to be taken into account.
Finally, there is considerable concern about the favouritism of antibiotic resistance in natural strains of
bacteria which probably are able to enter drinking water distribution networks (Jones et al. 2005). So,
little knowledge about behaviour of pharmaceuticals in subtherapeutical concentrations and possible
risks for humans and environmental habitats stand against an increased usage of these compounds in
human and veterinary medicine. Some pharmaceuticals are consumed in the range of hundreds of tons
per year for Germany only (Fent et al. 2006).
The main path for pharmaceuticals after usage is the disposal (from different sources such as
hospitals, households, manufacturers or agriculture) via wastewater (Fent et al. 2006). Municipal STPs
have to deal with this wastewater, spiked with different trace pollutants and often enough some of
these pollutants leave the STP unaffected. Some advanced water clarification techniques, as ozonation,
membrane bioreactors or coagulation/flocculation and flotation, have been brought into discussion to
improve the removal of these trace pollutants (Jones et al. 2005).
The aim of this review is to introduce some of the techniques which could be used in order to
remove pharmaceuticals from wastewater or which are already in operation. For several selected
pharmaceuticals the removal efficiency will be discussed, taking into consideration their chemical and
Selected Pharmaceuticals
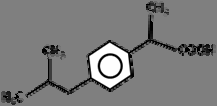
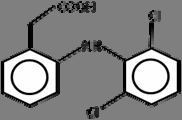
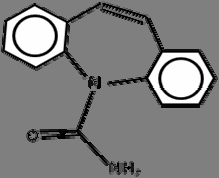
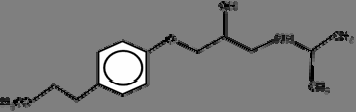
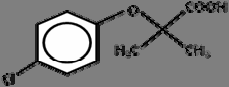
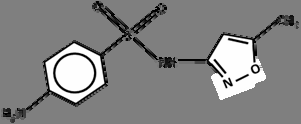
Seven substances representing the variety of chemicals used in health products were chosen for this
study. These substances are Diclofenac, Ibuprofen, Carbamazepin, Clofibric Acid, Sulfamethoxazole,
Iopromide and Metoprolol. Some characteristics and the chemical structure of each compound are
The pharmaceuticals were selected to take into consideration different substance classes within the
group of pharmaceuticals. Another criterion was the availability of recent reports about their removal
behaviour in wastewater. Finally, the selected chemicals had to have significant concentrations
in sewage effluents and natural waters.
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
Diclofenac and Ibuprofen are widely used non-steroidal anti-inflammatory drugs (NSAID),
consumed in high amounts in industrial countries (86 t and 345 t, respectively per year in Germany
2001; Fent 2006). These compounds are among the most abundant medicinal trace pollutants in rivers
(Fent et al. 2006; Wiegel et al. 2004). Carbamazepine is an anti-epileptic drug, which can also be
found in detectable concentrations in various surface waters (Wiegel et al. 2004 reported a maximum
value in the Elbe river of 1.2 µg/l). The relative high persistence of Carbamazepine makes its
degradation difficult. Relative high Carbamazepine concentrations in STP solids and in sediments are
also reported (Fent et al. 2006). Clofibric Acid stands as a representative for a metabolic product of a
pharmaceutical. It develops from the lipid lowering agents Clofibrate, Etofibrate and Etofyllin
clofibrate and is, like Carbamazepine, known for its persistence and widespread occurrence in
effluents and natural water bodies. Metoprolol is an example for a beta-blocker, a pharmaceutical
used to treat blood hypertension. It was detected in ranges of µg/l in wastewater and surface water.
Sotalol, a Metoprolol-relative compound, was found also in groundwater (Fent et al. 2006).
Sulfamethoxazole, a sulfonamide derivative, was selected because of its antibiotic action. Iopromide is
an iodinated X-ray contrast medium, which is just designed to be persistent. So, degradation of
wastewater, especially from hospitals can be problematic in occurrence of such compound.
Conventional wastewater treatment
The conventional treatment of wastewater in most municipal STPs consists of the steps mechanical
pre-treatment (homogenisation, removal of solids), preliminary treatment (e.g. addition of flocculation
agents), primary sedimentation and biological treatment (aerobic nitrification, anaerobic
denitrification, phosphate removal). As a by-product, sludge is produced which can be used to get
biogas from anaerobic digestion or as a fertilizer on agricultural areas (Radjenovic et al. 2007; Ternes
et al. 2007). The effluent is discharged into small rivers or streams. Jones, and coworkers (2005)
reported that several pharmaceuticals,a. o. Carbamazepine, pass conventional wastewater treatment
plants with little or without degradation.
A study from Wang , and coworkers (2008) showed that the pharmaceuticals Clofibric acid and
Carbamazepine have no effect on microbial growth in wastewater with high organic loading, but there
is a possibility that at least Carbamazepine (in concentrations of > 10 µg/l) can affect microbes in
STPs in wastewater with low organic loading. So, the inhibition of microbial growth by some
pharmaceuticals could be one reason for the incomplete removal of these substances in municipal
STPs. A concentration of Carbamazepine in the order of 10 µg/l is not likely in wastewater, but Wang,
and coworkers (2008) point out that effects on microbial growth possibly occur at lower
Some attempts have been made in order to degrade pharmaceuticals with higher efficiency which
will be introduced in the following sections. .
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008 Table 1 Chemical structure and some characteristics of the selected pharmaceuticals.
KOW: octanol-water distribution coefficient (the quotient between the concentration of the compound in an
organic octanol- and an aqueous water-phase);
Kd: solid-water distribution coefficient (the quotient between the concentration of a compound in a solid and the
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008 Coagulation-flocculation and flotation
One attempt to improve pharmaceutical removal in wastewater is to enhance the separation by
physical means. Coagulation-flocculation means the addition of metal salts like iron (III) chloride or
aluminum phosphate to the water in order to allow a precipitation or agglomeration of suspended
solids and colloids. Because lipophilic trace pollutants are likely to be found adsorbed on colloids, this
technique may be an option to remove certain non-polar pharmaceuticals from the wastewater, too
Flotation on the other hand stands for separating fine solid particles from the aqueous phase by
adhering them to the surface of upstreaming bubbles of air (Carballa et al. 2005). Again, non-polar
pharmaceuticals, sorbed onto these solids or lipophilic phases, can be removed this way.
Some positive results were gained for so-treated sewage effluent in the work of Carballa et al. 2005.
During coagulation-flocculation lipophilic compounds, as Diclofenac, were removed up to 70 %, due
to their significant sorption affinity. But, for Diclofenac one has to consider, that this substance is
partly ionized in neutral pH. So, a further removal through binding by cations of suspended solids is
resumed by the authors. More polar compounds were removed to a much lesser extent from the
wastewater. Contradictory to this behaviour the lipophilic substances Carbamazepine and Ibuprofen
were not affected by coagulant addition at all. This is possibly due to their poor sorption on solids and
therefore very low Kd values (see table 1).
Carballa et al. 2005 also investigated a flotation approach. In their study, Diclofenac,
Carbamazepine and Ibuprofen were removed up to 45%, 35% and 25%, respectively. The best results
were gained for the addition of fat as the hydrophobic phase.
Anaerobic digestion of sewage sludge
Sewage sludge that results from municipal sewage treatment contaminated with pharmaceuticals can
be subjected to an additional anaerobic treatment in order to improve its properties. Pharmaceuticals
being adsorbed to the sludge or dissolved in the high water content (>90%) can accumulate in the STP
during the sludge cycling or in the environment after disposal (Carballa et al. 2007b).
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
In this additional sludge digestion process organic matter is degraded anaerobically under mesophilic
(37.5°C*) or thermophilic (55.5°C*) conditions by a microbial community. The major metabolism
process in anaerobic sludge digestion, methanogenesis, is known not be affected by Carbamazepine
and Sulfamethoxazole in concentrations up to 400 mg/l. In contrast, Diclofenac inhibited this process
at high concentrations (Carballa et al. 2007b).
Nearly all pharmaceuticals investigated in the study of Carballa and coworkers (2007b) were
affected by the anaerobic digestion (average removal in brackets): Sulfamethoxazole (99%),
Diclofenac (69%), Ibuprofen (41%), Iopromide (25%). However, no Carbamazepine removal could be
* mean temperatures used by Carballa et al. 2007b
detected. This is similar to the behaviour of Carbamazepine in soil under anaerobic conditions. The
Iopromide removal is still in the range of the statistical error for Carballas experiment, so it is possible
that this substance is persistent under the given conditions, too.
Best results were obtained after prolonged adaptation of the micro flora to the sludge conditions,
like organic loading, temperature and solid content. So, a variation of sludge retention time had an
effect on the activity of the microbial population. Carballa and coworkers assume that an increase in
removal for some compounds (e.g. Diclofenac whose removal was increased to 80 % by extended
contact time) was due to an increase in biodiversity of the degraders. The temperature of the process
was found of minor influence to pharmaceutical removal instead.
Irrigation and soil passage
One option to handle liquid effluents from STPs is to irrigate these on agricultural land. Studies have
shown that some pharmaceuticals in the effluent are degraded during the soil passage, but others are
possibly able to reach the groundwater (Ternes et al. 2007; Yu et al. 2006). Aerobic microbial
degradation of disposed organics is thought to take place in soil above aquifers (Yu et al. 2006). While
Yu and coworkers reproduced this process as a batch experiment with activated sludge as an
inoculum, Ternes investigated a real wastewater treatment operation with long time irrigation on
Yu and coworkers (2006) demonstrated the key role of soil micro flora in the degradation of trace
amounts of organic compounds. Wastewater loaded with pharmaceuticals showed no decrease in these
substances in a sterile soil over the incubation period (50 days). In contrast, all pharmaceuticals
studied, except for Diclofenac, were degraded to an extent of over 60% in the inoculated soil within 50
days. But none of the “problem substances” Iopromide or Carbamazepepine were investigated. Also
the controlled conditions of the experiment have to be taken into account. Sorption seemed to be
insignificant as a removal mechanism because the abiotic control experiment exhibited relatively
constant pharmaceutical concentrations for the whole incubation period. Therefore a biotransformation
of the pharmaceuticals was assumed by the authors to explain the removal of these substances.
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
Ternes et al. 2007 gained ambivalent results in the field. A number of pharmaceuticals disposed
onto the soil with effluent and sludge never reached the groundwater, possibly due to their lipophilic
nature which hindered their mobility in the soil. This in contrast to the study mentioned before in
which abiotic processes like absorption played no significant role. Additionally, the soil microflora
had a long time to adapt to the inflow of anthropogenic compounds (45 years of irrigation history at
this site). Ibuprofen, Metoprolol and Iopromide were removed to a high extent during soil passage
(>80%). The authors made no differentiation between sorption and biodegradation there, but assumed
that biological degradation is the major removal mechanism in this case, based on the physical and
chemical properties of these compounds. Indeed, Carbamazepine and Sulfamethoxazole were detected
in the groundwater beneath the irrigation area in orders of µg/l. Especially Carbamazepine seemed to
accumulate under sites with long irrigation history, indicating a low biodegradation even through
adapted micro flora. In summary, Ternes et al. 2007 points out, that most pharmaceuticals are
biodegraded or sorbed during soil-aquifer passage. So, the relatively simple technique has a high
efficiency in removing pharmaceuticals. However, some substances remain unaffected to some extent
and reach the aquifer. This is especially the case for Carbamazepine and Sulfamethoxazole which
show their hydrophilic behaviour also during sand filtration (Nakada et al. 2007). Also the production
of toxic metabolic products in general by the micro flora can not be excluded (Ternes et al. 2007).
Membrane bioreactor
In order to remove pharmaceuticals from STP effluents membrane bioreactors (MBRs) were applied in
laboratory scale and for some compounds in pilot scale (Clara et al. 2005; Radjenovic et al. 2007).
They combine the physical separation of liquids and suspended solids with biological degradation. In
addition to the sorption of lipophilic substances bacteria are held back in the system, allowing their
enhanced adaptation to substances and conditions. In addition, molecules of high molecular weight are
held back by membranes due to size exclusion. Another advantage is the exclusion of pathogens, so
they are not able to enter drinking water distribution or natural water bodies (Clara et al. 2005).
Clara and coworkers (2005) found that Diclofenac removal by size exclusion failed, but a partial
removal could be obtained by rising the sludge retention time. Ibuprofen on the other hand was
removed to a high degree (> 90%). Carbamazepine was not removed at all. A comparison between
membrane bioreactor and conventional treatment led to similar effluent concentrations of the
investigated substances. Clara et al. 2005 concluded therefore that membrane bioreactors show no
additional pharmaceutical removal compared to conventional treatment. Especially size exclusion
seemed to be ineffective for the purpose.
To hold back pharmaceuticals with membranes, dense membranes as used in reverse osmosis or
nanofiltration would be required. Mainly economic reasons (e.g. high costs due to increased power
consumption) stand against it (Clara et al. 2005). One has also to think about the fact, that the
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
molecular size of the pharmaceuticals is at least 100 times smaller than the pore size of membranes.
So, only substances sorbed on particles are retained (Radjenovic et al. 2007).
In contrast to Clara et al. 2005 a study by Radjenovic et al. 2007 indicated a better pharmaceutical
removal in some cases (Diclofenac removal of 87.4% in MBR compared to 50.1% in conventional
treatment; Metoprolol removal 58.7% compared to 0%; Clofibric Acid removal 71.8% compared to
27.7%), compared to conventional treatment. But again, some treatment results were similar to
conventional treatment (e.g. for Ibuprofen, removal > 80%) and Carbamazepine passed both systems
without degradation or transformation. For Sulfamethoxazole a variation of removal rates were found.
Maybe there was some back conversion of the human metabolite N4-acetylsulfamethoxazole to the
initial compound during treatment. Interestingly, the membrane pore size of 0.4 µm decreased during
operation of the MBR to a size of 0.01 µm due to microbial fouling.
Ozonation
Ozonation is one of the advanced techniques for waste water treatment and subject of many recent
studies (Ternes et al. 2003; Huber et al. 2005; Carballa, Manterola et al. 2007; Nakada et al. 2007).
Ozonation was first introduced as a disinfection method beside UV- and H2O2-treatment. In some
STPs ozone, UV-radiation and hydrogen peroxide are combined to raise the cleaning and disinfection
effect (Ternes et al. 2003). The main mode of action in the ozonation process is the formation of OH
radicals due to ozone decay in the water, but there are also ozone molecules present for chemical
attack. This increases the oxidation capacity (Ternes et al. 2003, Huber et al. 2005). As an advantage,
no oxidant residues remain (Carballa et al. 2007a).
Disagreement exists for the ozone dose necessary for pharmaceutical removal. Ternes et al. 2003
reports of a nearly complete removal of pharmaceuticals with an ozone dose of 10 to 15 mg for every
litre wastewater (contact time 18 minutes) treated in a municipal STP. Only contrast media, like
Iopromide, remained to some extent. In contrary, Huber et al. 2005 pointed out, that only more than 2
mg/l ozone was needed to oxidize a range of pharmaceuticals (among them Diclofenac and
Sulfamethoxazole) to an extent of 90 to 99 %. But also in this study, X-ray contrast media remained
partly oxidized. In general, in both studies increased the pharmaceutical oxidation with increased
ozone levels. The differences in necessary ozone doses could be due to differences in organic loading
Carballa and coworkers (2007a) wanted to find out whether ozonation can be used for treatment of
sewage sludge, too. For 20 mg ozone per gram dry weight a removal of diverse pharmaceuticals of 20
to 99 % was achieved. The lowest removal was found for Iopromide whereas Sulfamethoxazole
showed very high removal. But it was also found that ozone pre-treatment of sewage sludge had only a
measurable effect compared to conventional sludge treatment for Carbamazepine (no removal in
conventional treatment, up to 60 % removal with additional ozonation). Ozone treatment also had
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
Besides the disinfection advantage of ozonation there is concern about possible by-products with
probable higher toxicity. Ternes et al. 2003 points out, that the products evolved during ozonation are
unknown. During ozonation hydrolysis and partial oxidation occurs while total oxidation of the
compounds is avoided (Carballa et al. 2007a). On the other hand one assumes an increasing number
of functional groups in the molecule together with a higher polarity. So it is the belief that during the
ozonation process the properties of the molecules responsible for their medicinal action should
The results of the previous studies indicate, that ozonation of pharmaceuticals depends on their
chemical structure. While compounds with a C=C bond or aromatic structures seem to be susceptible
to ozonation, compounds with amide structures are resistant to it (Nakada et al. 2007).
Another factor to consider is that the ozone consumption is not only due to pharmaceuticals but of
course by any other organic load, too. In waters with high DOC most ozone is consumed before
possible attack on trace pollutants. So there is a need for additional treatment (Ternes et al. 2003).
Conclusions
Attention on pharmaceutical trace pollution of sewage, surface and drinking waters has risen recently.
There are some attempts to eliminate these types of trace pollutants in laboratory or treatment plant
scale. Depending on the physical and chemical properties of the compounds the degradation of the
selected pharmaceuticals varied to some extent. Physical methods like sand filtration, irrigation or
coagulation/flocculation and flotation are limited for substances which show a hydrophobic nature, as
Carbamazepine or Sulfamethoxazole do. Anaerobic digestion seems to be a good tool for degradation
of a range of pharmaceuticals. Iopromide and again Carbamazepine are problematic in this case.
Operation of membrane bioreactor systems led to an improved degradation in some cases, but the
results are contradictory. A Carbamazepine removal could also not be reached. Ozonation had some
promising results for liquid wastes but could not handle with contrast media like Iopromide.
In general there is no method which is able to eliminate all pharmaceuticals from the water. All of
them can improve the water quality but this is paid with increased efforts. Economic concerns and the
technical feasibility limit the usage of the advanced techniques shown here. More investigations in
toxicity of pharmaceuticals and their metabolites are needed to understand the real risk for natural
References
Carballa M, Omil F, Lema JM (2005) Removal of cosmetic ingredients and pharmaceuticals in sewage primary
Carballa M, Manterola G, Larrea L, Ternes T, Omil F, Lema JM (2007a) Influence of ozone pre-treatment on
sludge anaerobic digestion: Removal of pharmaceutical and personal care products. Chemosphere 67: 1444-1452
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
Carballa M, Omil F, Ternes T, Lema JM (2007b) Fate of pharmaceutical and personal care products (PPCPs)
during anaerobic digestion of sewage sludge. Water Res 41: 2139-2150
Clara M, Strenn B, Gans O, Martinez E, Kreuzinger N, Kroiss H (2005) Removal of selected pharmaceuticals,
fragrances and endocrine disrupting compounds in a membrane bioreactor and conventional wastewater
treatment plants. Water Res 39: 4797-4807
Fent K, Weston AA, Caminada D (2006) Ecotoxicology of human pharmaceuticals. Aquat Toxicol 76: 122-159
Huber MM, Göbel A, Joss A, Hermann N, Löffler D, McArdell CS, Ried A, Siegrist H, Ternes T, von Gunten U
(2005) Oxidation of Pharmaceuticals during Ozonation of Municipal Wastewater Effluents: A Pilot Study.
Jones OA, Lester JN, Voulvoulis N (2005) Pharmaceuticals: a threat to drinking water?. TRENDS in
Nakada N, Shinohara H, Murata A, Kiri K, Managaki S, Sato N, Takada H (2007) Removal of selected
pharmaceuticals and personal care products (PPCPs) and endocrine-disrupting chemicals (EDCs) during sand
filtration and ozonation at a municipal sewage treatment plant. Water Res 41: 4373-4382
Radjenovic J, Petrovic M, Barceló D (2007) Analysis of pharmaceuticals in wastewater and removal using a
membrane bioreactor. Anal Bioanal Chem 387: 1365-1377
Ternes TA, Bonerz M, Herrmann N, Teiser B, Andersen HR (2007) Irrigation of treated wastewater in
Braunschweig, Germany: An option to remove pharmaceuticals and musk fragrances. Chemosphere 66: 894-904
Ternes TA, Stüber J, Herrmann N, McDowell D, Ried A, Kampmann M, Teiser B (2003) Ozonation: a tool for
removal of pharmaceuticals, contrast media and musk fragrances from wastewater?. Water Res 37: 1976-1982
Wang S, Holzem RM, Gunsch CK (2008) Effects of Pharmaceutically Active Compounds on a Mixed Microbial
Community Originating from a Municipal Wastewater Treatment Plant. Environ Sci Technol 42: 1091-1095
Wiegel S, Aulinger A, Brockmeyer R, Harms H, Löffler J, Reincke H, Schmidt R, Stachel B, von Tümpling W,
Wanke A (2004) Pharmaceuticals in the river Elbe and its tributaries. Chemosphere 57: 107-126
Yu JT, Bouwer EJ, Coelhan M (2006) Occurrence and biodegradability studies of selected pharmaceuticals and
personal care products in sewage effluent. Agricultural Water Management 86: 72-80
Published by Oxford University Press on behalf of the International Epidemiological AssociationInternational Journal of Epidemiology 2006;35:3–9 Ó The Author 2006; all rights reserved. Advance Access publication 5 January 2006Treatment and prevention of obesity—arethere critical periods for intervention?whether there is sufficient evidence relating critical/sensitiveperiods of developmen
Tretinoin – by mouth Description When taken by mouth, tretinoin (also called ATRA, all trans-retinoic acid, or Vesanoid®) is used to treat a type of leukemia known as acute promyelocytic leukemia (APL). Tretinoin is available as a 10mg two-tone (orange-yellow and reddish-brown) capsule taken by mouth. Important • Women who are pregnant should not take this medicine, because treti





 R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008 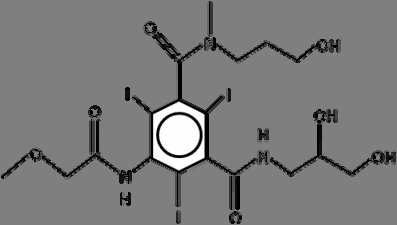
 R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008
R. Wetzig; Removal of selected pharmaceuticals from sewage water by advanced treatment 2008