He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Spe international symposium_86719_paper#3_12-10-03.pdf
Malaria Chemoprophylaxis Compliance Improvement: A New ApproachKelly J. Moynihan;a Jean-Marie M. Moreau;b Leba G. Shallenberger;b Kenneth C. Lindemann;b and Philippe Guibertc 1
Copyright 2004, Society of Petroleum Engineers Inc.
immune workers decreased fifty percent and the program has
This paper was prepared for presentation at The Seventh SPE International Conference on
been extended to other operating locations in Africa.
Health, Safety, and Environment in Oil and Gas Exploration and Production held in Calgary,Alberta, Canada, 29–31 March 2004. Introduction
This paper was selected for presentation by an SPE Program Committee following review ofinformation contained in a proposal submitted by the author(s). Contents of the paper, as
ExxonMobil conducts business in over 100 countries
presented, have not been reviewed by the Society of Petroleum Engineers and are subject tocorrection by the author(s). The material, as presented, does not necessarily reflect any
worldwide. In some of these countries (especially those in
position of the Society of Petroleum Engineers, its officers, or members. Papers presented at
sub-Saharan Africa, parts of south east Asia, and Latin
SPE meetings are subject to publication review by Editorial Committees of the Society ofPetroleum Engineers. Electronic reproduction, distribution, or storage of any part of this paper
America), one or more forms of malaria are endemic.2
for commercial purposes without the written consent of the Society of Petroleum Engineers is
In order to safeguard its employees from the ill effects of
prohibited. Permission to reproduce in print is restricted to a proposal of not more than 300words; illustrations may not be copied. The proposal must contain conspicuous
malaria, ExxonMobil developed and implemented a
acknowledgment of where and by whom the paper was presented. Write Librarian, SPE, P.O. Box 833836, Richardson, TX 75083-3836, U.S.A., fax 01-972-952-9435.
comprehensive Malaria Control Program (MCP) based on thefollowing "ABCD" strategy:3
Abstract
Awareness training, personal protection against mosquito
bites, and vector control measures are all important in helping
Chemoprophylaxis use by non-immune individuals.4
reduce Anopheles mosquito bites. However, these measures
cannot completely eliminate the risk of contracting malaria.
This paper discusses the Chad Export Project's5
The prevention of malaria in non-immune individuals in sub-
implementation of the MCP and in particular the development
Saharan Africa relies heavily on the proper use of effective
and implementation of a Malaria Chemoprophylaxis
chemoprophylaxis. Compliance with effective
Compliance Program (MCCP), a MCP enhancement aimed at
chemoprophylactic regimens is problematic, especially in
ensuring effective malaria chemoprophylaxis use by non-
long-term expatriates who believe they have acquired natural
immune individuals in order to achieve the MCP's goal of zero
immunity. In spite of implementing a comprehensive Malaria
Control Program (MCP), with a goal of zero cases of malariaamong non-immune individuals, the Chad Export Project
Chad Export Project - Background
experienced an increase in the number of malaria cases in thecontractor non-immune workforce as construction activities in
Project Description and Background Information. The
Chad and Cameroon accelerated. Several serious cases of
$US 3.5 billion Chad Export Project (the Project) is currently
Falciparum malaria were recorded, and four fatalities
the largest private sector investment in sub-Saharan Africa.
occurred. In response to this, a multidisciplinary team was
Over the Project's anticipated 25-30 year life, approximately
formed to identify opportunities to enhance the effectiveness
one billion barrels of crude oil will be produced from three
of the MCP. One of the team's key recommendations was to
oilfields in the Doba basin region of southern Chad for export
develop and implement a Malaria Chemoprophylaxis
to world markets, with peak production being 225,000 barrels
Compliance Program (MCCP) to address identified
informational and behavioral shortcomings regarding malaria
A map providing some geographic context for the Project
chemoprophylaxis use. The heart of the MCCP is awareness
and education but compliance with chemoprophylaxis is
further encouraged through collection of urine specimens from
There are four Anopheles mosquito-transmitted parasites that cause malaria:
Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, and
non-immune individuals for laboratory determination of
Plasmodium malariae. Malaria caused by the Plasmodium falciparum parasite
effective anti-malaria medication usage. Data collected during
is the most serious form of the disease and is the most prevalent type of
the first 15 months that the MCCP was implemented in Chad
and Cameroon show an overall low (i.e., <1%) rate of non-
ExxonMobil's Malaria Control Program is based on a Malaria Control
Program developed in 1998 for the ExxonMobil-led Chad Export Project. The
conforming specimens. After implementing the MCCP in
ExxonMobil program was implemented worldwide beginning in 2001.
Chad and Cameroon, the rate of malaria cases among non-
4 With regard to malaria, non-immune individuals are defined as thoseindividuals who were not born and raised in the malarious country/region in
1 aExxonMobil Development Company, Houston, Texas; bExxonMobil
5 ExxonMobil has a 40% interest in the Chad Export Project and is the
Medicine and Occupational Health, Houston, Texas; cInternational SOS
operator. Other Project Consortium members include Petronas (35% interest)
K.J. MOYNIHAN; J-M.M. MOREAU; L.G. SHALLENBERGER; K.C. LINDEMANN; AND P. GUIBERT
Figure 1. Geographic Context for the Chad Export Project
Planning for the Chad Export Project began in 1993, with
Key Project components in the oilfield development area
construction beginning in October 2000. The first crude oil
(from the Miandoum oilfield) was produced in July 2003, and
the first sale of oil to international markets occurred in
− Komé, Miandoum, and Bolobo oilfields -
October 2003. Completion of the Project's Central Treating
approximately 250 wells will be drilled to develop
Facility (CTF) in the oilfield development area is anticipated
and recover the hydrocarbon reserves in these
by year-end 2003, with full production commencing in 2004.
− Gathering system to collect and transport produced
Climatic Setting With Regard to Malaria. The climate in
the portions of Chad and Cameroon traversed by the Chad
− Central Treating Facility to produce export quality
Export Project's crude oil export pipeline can be characterized
as being semi-dry sub-tropical to moist tropical.
− Operations Center located in the Komé field,
Two seasons exist in the oilfield development area in
consisting of the CTF, an airstrip, housing for 200
southern Chad - a long dry season (October - May) and a short
individuals, and a 120 MW power plant to serve
rainy season (June - September). During an average rainy
season, approximately 1000-1100 mm of rainfall occurs.
Along the pipeline route from Komé, Chad to Kribi,
− 1070 kilometer long 760 mm diameter buried export
Cameroon, the rainy season progressively lengthens. For
pipeline from Komé, Chad to Kribi, Cameroon.
example, average annual rainfall near Meiganga, Cameroon
− Three pump stations - Pump Station #1 adjacent to
(~325 km southwest of Komé, Chad) is 1500-1600 mm, and at
the Central Treating Facility in the Komé oilfield,
Lolodorf, Cameroon, the mean annual rainfall is
Pump Station #2 near Dompta, Cameroon, and Pump
approximately 1700 mm. In the coastal area near Kribi,
Cameroon, two rainy seasons actually exist, resulting in a
− Pressure reducing station near Kribi, Cameroon.
mean annual rainfall in excess of 2500 mm.
Climate and rainfall, coupled with the remoteness of many
Floating Storage and Offloading vessel (the Komé
locales and the developing nation status of both Chad and
Kribi 1), a 2 million barrel converted tanker fixed in
Cameroon, result in a suitable environment for the malaria
place approximately 12 kilometers offshore via a
parasite's transmission vector, the Anopheles mosquito. The
MALARIA CHEMOPROPHYLAXIS COMPLIANCE IMPROVEMENT: A NEW APPROACH
map in Figure 2 reveals that conditions are favorable for the
was spread over a distance of >1000 kilometers, presented a
transmission of malaria throughout the Project area, from a
number of malaria prevention challenges.
minimum of 6 months each year in the oilfield developmentarea in southern Chad to year-round in southern Cameroon. Implementation of the Malaria Control Program and Initial Performance As part of their orientation training, all Project workers (both ExxonMobil and contractor employees) received a health briefing that included information about malaria and an overview of the Malaria Control Program's "ABCD" strategy for preventing malaria. Non-immune individuals were also reminded about the fitness-for-duty requirement for them to self-administer anti-malaria medication.
Overall, a relatively low number of malaria cases occurred
among the Project's semi-immune workforce (versus the rateof occurrence in the general Chadian and Cameroonianpopulation), and no deaths were recorded. This remarkablesituation can be attributed to education, the promotion and useof mosquito bite prevention measures and ready access to highquality medical care for diagnosis and treatment.
A relatively low number of malaria cases were recorded in
the Project's non-immune workforce in the early stages ofconstruction. However, as construction activities acceleratedin late 2001/early 2002 and the workforce grew accordingly,
Figure 2. Map of Africa showing the number of months each year
the number of malaria cases in non-immune workers began to
that are suitable for the transmission of malaria.
climb. At approximately the same time (i.e., second quarter of2002), two contractor employees who had been working on
In the Project area, Chloroquine-resistant Falciparum
the Project in Cameroon died from Falciparum malaria upon
malaria is the most prevalent form of the disease, although
their return to the United States.6 These two situations
Vivax malaria also (rarely) occurs.
prompted the Project to undertake an immediate, detailedevaluation of the MCP and its implementation. Personnel-Related Challenges Regarding Malaria and Its
Although this analysis revealed opportunities for
Prevention. The Chad Export Project's construction phase
improvement in all facets of the MCP, it was determined that
workforce peaked at over 13,000 individuals in November
issues associated with malaria chemoprophylaxis use in the
2002. Chadians and Cameroonians, who have a degree of
non-immune workforce (especially the contractor non-immune
natural immunity to malaria and are familiar with the disease,
workforce) warranted particular and urgent attention.
constituted 65-90% of the workforce during the constructionperiod. Based on epidemiological data from the countries of
Development and Implementation of the Malaria
Chad and Cameroon and absent an effective control program,
Chemoprophylaxis Compliance Program
a high rate of malaria among the semi-immune workforce may
A number of key learnings related to malaria
have occurred, with significant lost time and several deaths.
chemoprophylaxis use in the non-immune contractor
Key characteristics of the Project's several thousand-strong
workforce arose from the 2Q2002 evaluation of the Project's
non-immune construction phase workforce with regard to
implementation of the MCP, including the following:
• Some non-immune individuals were not taking any type
− Composed of three groups, with some individuals
• Some non-immune individuals were taking anti-malaria
having preconceived attitudes regarding malaria.
medications that are not effective in preventing
Residents of non-malarious countries (e.g.,
Europe, United States, Canada) with little or no
Chloroquine, Chloroquine + Proguanil combination
malaria-related knowledge/experience.
Residents of malarious countries where less
• Some non-immune individuals were taking anti-malaria
serious forms of malaria (versusFalciparum
medications that are known to be effective in preventing
Chloroquine-resistant Falciparum malaria (i.e., Malarone,
• Multi-lingual (most common languages = French,
Lariam, doxycycline), but were not taking the medication
• Geographically dispersed in locations where the risk of
These characteristics, taken together with the fact that the
6 During the third quarter of 2002 (i.e., during the time that the MCCP was
majority of the Project's construction phase workforce was
being developed and initially implemented), the Project experienced twoadditional contractor employee Falciparum malaria fatalities. As was the case
provided by nine prime contractors and that the work front
for the two fatalities in 2Q2002, the 3Q2002 malaria deaths occurred outsideof Africa after the individuals had returned to their home countries.
K.J. MOYNIHAN; J-M.M. MOREAU; L.G. SHALLENBERGER; K.C. LINDEMANN; AND P. GUIBERT
In view of these and other findings, a multidisciplinary
Malaria Chemoprophylaxis Compliance Program (MCCP) for
team7 (the MCCP team) was assembled to develop a strategy
to improve compliance with the Project's malariachemoprophylaxis use requirement for non-immune
Medical Review Process. Anticipating that some individuals
would produce urine specimens that do not contain a
The team determined that the use of effective malaria
detectable quantity of one of the three chemoprophylatic
chemoprophylaxis in the Project's non-immune workforce
agents known to be effective in preventing Falciparum
could be significantly improved if the following actions were
malaria (i.e., failed tests), a Medical Review Process was
developed and incorporated into the MCCP.
• Develop a new training program aimed at non-immune
The Medical Review Process is executed in a confidential
individuals (both ExxonMobil and contractor employees)
manner by a designated Medical Review Officer (MRO) and
to reinforce the Malaria Control Program and its "ABCD"
was designed to comply with applicable medical information
malaria prevention strategy, emphasizing bite prevention
("B"), effective malaria chemoprophylaxis use ("C"), and
The MRO conducts an in-person or telephone interview
early diagnosis and treatment ("D").
with each individual producing a non-conforming specimen
− Inform/remind non-immune individuals working
following a prescribed interview template. The consent of the
in/traveling to Chad and/or Cameroon about the
individual to conduct the interview is sought.10 Depending on
fitness-for-duty requirement to properly self-
the information obtained via the (consensual) telephone
administer an anti-malaria medication known to be
interview, the following actions are possible:
effective in preventing Chloroquine-resistant
• The individual is referred to a physician at the work
Falciparum malaria (i.e., Malarone, Lariam,
location to be further interviewed and re-tested after a
period of observed chemoprophylaxis use.
− Inform/remind non-immune individuals about the
− If the subsequent testing reveals a measurable
importance of seeking prompt medical attention for
quantity of the chemoprophylatic agent in the
any illness so that malaria could be ruled out or
individual's urine, the individual is declared to be fit-
properly treated, despite the use of an effective anti-
for-duty and he/she is placed in a Frequent Testing
• Develop and implement an anti-malaria medication use
− If the subsequent testing does not reveal a measurable
compliance assurance program aimed at non-immune
quantity of the chemoprophylatic agent in the
individuals and require individuals to attest that they will
individual's urine, the individual is given the option
participate in the program as a condition of their
of selecting one of the other two effective anti-
assignment to a malaria risk location (i.e., Chad and
malaria medications to self-administer, or to self-
declare that he/she is unfit-for-duty in the malarious
With regard to the anti-malaria medication use compliance
location. If the former option is selected, he/she is
assurance program, the team determined that for such a
placed in a Frequent Testing Pool after being re-
program to be effective, it should possess the following
chemoprophylaxis use. If the individual self-declares
• Random, unannounced collection of biological specimens
that he/she is unfit-for-duty, a process is initiated to
(i.e., urine) followed by laboratory analysis of the
remove the individual from the malarious location as
specimens to confirm the presence of a chemoprophylatic
agent known to be effective in preventing Chloroquine-
• If the individual is unable to take one of the three
resistant Falciparum malaria.
effective anti-malaria medications or he/she is unwilling
• Well-documented specimen handling procedures
to take one of these medications, he/she is declared to be
designed to ensure specimen stability/integrity and the
unfit-for-duty in the malarious location and a process is
initiated to remove the individual from the malarious
• Confidential medical review process for individuals
producing non-conforming specimens to determine theirgo-forward fitness-for-duty status. Enrollment in the MCCP. All individuals eligible for anti-
• Conformance of all program components with appropriate
malaria medication use compliance testing are required to sign
clinical and medical information privacy protection
a MCCP Attestation Form to document their understanding of
the program's requirements. By signing their Attestation Form,
With these attributes and requirements as the cornerstone,
individuals acknowledge/agree to the following:
the team proceeded expeditiously to develop and implement a
8 A medical ethics committee reviewed the procedural aspects of the MCCPduring its development. 9 Separate MROs were appointed for ExxonMobil and contractor employees. 10 If an individual refuses to be interviewed or terminates an interview before
it is completed, the MRO is instructed to conclude that the individual has self-
7 The MCCP team included representatives from the business line,
declared that he/she is unfit-for-duty in the malarious location. A process is
professionals from medicine and occupational health, law, and human
then initiated to remove the individual from the malarious location as quickly
resources groups, and experts in forensic drug and alcohol testing programs.
MALARIA CHEMOPROPHYLAXIS COMPLIANCE IMPROVEMENT: A NEW APPROACH
• It is a fitness-for-duty requirement for non-immune
reinforced the MCP's "ABCD" strategy. A multimedia
individuals to properly self-administer an anti-malaria
presentation that was developed and produced in VCR and
medication known to be effective in preventing
CD-ROM formats was particularly effective in this program.
Chloroquine-resistant Falciparum malaria (i.e., Malarone,
Presentations were given in French, English, Filipino, Spanish,
Lariam, doxycycline) when working in/traveling to a
and Malay so as to optimize their effectiveness with the
Project's multi-lingual non-immune workers. Many sessions
• On a random, unannounced basis, they will be instructed
were also culturally adapted to increase their impact. In
to produce a urine specimen at a designated time and
addition to discussing malaria chemoprophylaxis-related
place for the purposes of determining their compliance
issues and the "mechanics" of the MCCP, the sessions
with the MCP's effective malaria chemoprophylaxis use
focussed heavily on the bite prevention ("B") and diagnose
and treat early ("D") components of the MCP.
Based on the success of the enhanced MCP in Chad and
Individuals producing non-conforming specimens will beasked to participate in a confidential medical review
Cameroon (including the MCCP), the program has been
process to determine their go-forward fitness-for-duty
extended to other locations based on malaria risk and
status. Individuals determined to be unfit-for-duty will be
removed from the malarious location (i.e., repatriated) asquickly as possible. Acknowledgements The authors of this paper would like to acknowledge the
efforts of the members of the MCCP Team, including David
Over the first 15 months (i.e., July 2002 - September 2003) of
Batey, Lea Conner, Adel Girgis, Alain Gonthier, Chuck
the MCCP's implementation in Chad and Cameroon,
Kearney, Dave Lofquist, and Jennifer McPhail. In addition,
approximately 2500 urine specimens were collected for anti-
we are grateful for the efforts of the Project's in-country
malaria medication use compliance testing. The percentage of
Medicine and Occupational Health Team, including Malik
individuals producing non-conforming specimens was very
Douga, Paul Essomba, Jacques LeMire, and Berthe Nseke as
low (<1%). The small number of individuals who have
well as the many International SOS healthcare professionals
produced non-conforming specimens participated in the
dedicated to the Project's camp clinics.
Medical Review with the following outcomes:
• 43% were entered into the Frequent Testing Pool (i.e.,
conditionally determined to be fit-for-duty).
• 57% demobilized from the Project or were declared unfit-
for-duty and were instructed to leave Chad or Cameroonas quickly as possible.
The implementation of the enhanced Malaria Control
Program, including its (new) Malaria ChemoprophylaxisCompliance Program component, has been effective inreducing malaria rates in the Project's non-immune population. This is evident in the data presented in the table below:
No. Falciparum Malaria Cases per 200,000 Work Hours (Non-Immune Workers)
As can be seen, the rate of Falciparum malaria in the
Project's non-immune workforce is markedly lower during thepeak exposure (i.e., rainy season) months in 2003 versus 2002. Discussion The data presented above indicate that the implementation of an enhanced Malaria Control Program (MCP) featuring a Malaria Chemoprophylaxis Compliance Program (MCCP) can successfully reduce the rate of Falciparum malaria in non- immune individuals working in a malarious area.
The MCCP was introduced to Project workers as part of an
effort aimed at improving the overall effectiveness of theMCP. This was accomplished by developing an aggressivemalaria awareness and prevention training program that
De Elektrische Sigaret; Dé ultieme oplossing als tabaksvervanger voor de roker én de doorn in het oog van farmacie, tabaksindustrie, gezondheidsclubjes en overheden. Wiens belang? “Als we geen accijnzen op sigaretten binnen krijgen, moet de veroorzaker van die derving worden verboden” (belang van de staat) “Als er een beter tabaksalternatief is dan pleisters en
 Malaria Chemoprophylaxis Compliance Improvement: A New ApproachKelly J. Moynihan;a Jean-Marie M. Moreau;b Leba G. Shallenberger;b Kenneth C. Lindemann;b and Philippe Guibertc 1
Copyright 2004, Society of Petroleum Engineers Inc.
Malaria Chemoprophylaxis Compliance Improvement: A New ApproachKelly J. Moynihan;a Jean-Marie M. Moreau;b Leba G. Shallenberger;b Kenneth C. Lindemann;b and Philippe Guibertc 1
Copyright 2004, Society of Petroleum Engineers Inc. K.J. MOYNIHAN; J-M.M. MOREAU; L.G. SHALLENBERGER; K.C. LINDEMANN; AND P. GUIBERT
Figure 1. Geographic Context for the Chad Export Project
K.J. MOYNIHAN; J-M.M. MOREAU; L.G. SHALLENBERGER; K.C. LINDEMANN; AND P. GUIBERT
Figure 1. Geographic Context for the Chad Export Project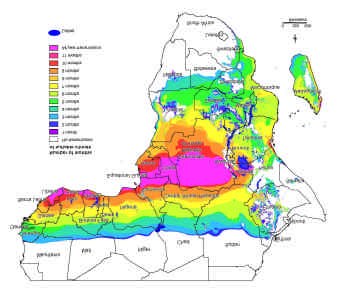 MALARIA CHEMOPROPHYLAXIS COMPLIANCE IMPROVEMENT: A NEW APPROACH
map in Figure 2 reveals that conditions are favorable for the
was spread over a distance of >1000 kilometers, presented a
transmission of malaria throughout the Project area, from a
number of malaria prevention challenges.
MALARIA CHEMOPROPHYLAXIS COMPLIANCE IMPROVEMENT: A NEW APPROACH
map in Figure 2 reveals that conditions are favorable for the
was spread over a distance of >1000 kilometers, presented a
transmission of malaria throughout the Project area, from a
number of malaria prevention challenges.