He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Efficacy
A Review of the Efficacy and Side Effects of
Introduction…………………………………………………………………….…………3 Methodology………………………………………………………………………………4 Results…………………………………………………………………………………….5 Efficacy……………………………………………………………………………5 Increase
Mineral Density (BMD)……………………………….5
Therapy………………………………….5
Raloxifene…………………………………………………………6 Alendronate……………………………………………………….8 Risedronate……………………………………………………….9 Decrease
Markers…………………………………….10
Therapy…………………………………10
Raloxifene……………………………………………………….10 Alendronate………………………………………………………10 Risedronate………………………………………………………11 Decreased
Risk…………………………………………………11
Therapy…………………………………11
Raloxifene……………………………………………………….12 Alendronate………………………………………………………12 Risedronate………………………………………………………14 Side
Effects………………………………………………………………………14
Hormone Replacement Therapy versus Raloxifene…………………….14
Cancer……………………………………………………………14 Pulmonary
Cardiovascular Disease and Serum Levels………………………15
Risedronate…………………………………………16
Comments……………………………………………………………………………….19 References……………………………………………………………………………….24
INTRODUCTION
Currently in the United States, over 10 million people are affected by
osteoporosis, while an estimated 34 million are believed to be at high risk for this
crippling bone disease. Postmenopausal women, whose estrogen levels have declined,
compose one of the highest-risk groups for this disease. Due to the heightened activity of
osteoclasts, osteoporosis sufferers are likely to experience a bone fracture later on in life.
Approximately 1 in every 2 women over the age of 50 develops an osteoporosis-related
bone fracture. Women represent a substantial portion of the 1.5 million fractures endured
Two types of drugs effectively treat and prevent osteoporosis.2 Bone formation
medications stimulate osteoblast activity, while antiresorptive drugs inhibit osteoclast
uptake and degradation of the calcified matrix.2,3 Antiresorptive drugs appear to
generate more promising results for osteoporosis sufferers and have already received
FDA approval.4 Four types of antiresorptive drugs are commonly used to treat
osteoporosis and prevent the degradation of bone: bisphosphonates, which include
alendronate and risedronate sodium; hormone replacement therapy (HRT), and the
second-generation SERM, raloxifene.2 Although these drugs vary slightly in their modes
of action, they all aim to increase bone mineral density (BMD) and halt bone resorption.
Since each of the antiresorptive drugs regulates osteoclast activity differently, it is
uncertain which drug most effectively targets and minimizes the degradative effect of the
osteoclasts. In addition, it has been shown that raloxifene, HRT, alendronate, and
risedronate serve as both agonists and antagonists in other tissues in the body. This
ability to target other tissues might lead to unwanted side effects, including
gastrointestinal adverse effects,5 breast cancer,6 and deep venous thromboembolic (VTE)
disease.6 Potential health benefits unrelated to bone functioning have been shown to
accompany raloxifene and HRT.6 Such benefits include an increase in high density
lipoproteins (HDL), a reduction of low density lipoproteins (LDL), and a decreased risk
of colorectal cancer.6 In order to fully evaluate the usefulness of each antiresorptive drug
for osteoporosis sufferers, it is imperative that research on these potential side effects also
be examined. This review will investigate recent research on the efficacy of each
antiresorptive drug not only in terms of its direct effect on BMD, bone turnover markers,
and fracture risk, but also in terms of its inadvertent health risks and benefits.
METHODOLOGY
Through the use of various medical and scientific journals, this review analyzed
and evaluated the various antiresorptive drugs. In order to obtain appropriate studies, the
databases, Pubmed, Ebsco, and Lexis Nexus were used. The following terms were
initially searched for in each of the databases: alendronate and osteoporosis, risedronate and osteoporosis, hormone replacement therapy and osteoporosis, and raloxifene and osteoporosis. Due to the large number of studies generated from these search terms, the
search terms had to be refined to be more specific. Depending on which efficacy
parameter was being examined, an additional search term of BMD, bone turnover markers, fracture risk, or side effects was added to each of the search terms previously
mentioned. To further limit the number of studies reviewed, a cohort restriction and date
restriction were imposed on the studies. Whenever possible, only studies displaying the
effects of antiresorptive drugs on postmenopausal women were used. Only double-blind
experiments conducted on a large population over an extended period of time were
reviewed. Furthermore, reviewed studies were limited to those that have been published
within the last five years, so that the most up-to-date data was presented. The figures
included in this review were used to give a graphical representation of the results. In
most cases, the study failed to supply the observed results in numerical form and instead
opted to present the results in a figure. In order to ensure the most accurate presentation
of such data, the original figures and tables were included in the review.
Efficacy
Increase in Bone Mineral Density (BMD)
Hormone Replacement Therapy (HRT)
Villareal et al7 analyzed the effect of HRT on BMD as well as on bone turnover
markers in women aged 75 or older in a randomized controlled trial (RCT). In this
double-blind, placebo-controlled trial lasting from September 1995 to August 2001, 67
women with mild to moderate physical frailty were examined. Patients exhibiting 2 of
the 3 following parameters were considered to display mild to moderate physical frailty:
(1) 11-18mL/min per kg of body weight for low peak aerobic power, (2) self-admitted
need for assistance with 2 necessary activities of daily living (ADLs) or 1 basic ADL, and
(3) a test score of 18 to 22 on a range of 0-36 on the modified physical performance test.
Patients either received 0.625mg/d of conjugated estrogen combined with 5mg/d of
medroxyprogesterone for 13 days every three months (n=45) or a placebo (n=22). After
9 months, patients receiving conjugated estrogen and medroxyprogesterone displayed a
4.3% increase in lumbar spine BMD compared to 0.4% (95% CI) increase exhibited by
the placebo patients. An increase of 1.7% in total hip BMD was observed in patients
taking the HRT, while a decrease of 0.1% from the baseline was observed in the placebo
In a randomized double-blind, placebo controlled study, Recker and colleagues8
examined 128 women who were older than 65. Eligible patients displayed a spinal BMD
less than or equal to 0.90g/cm2 at baseline. Patients either received 0.3mg/d of
conjugated equine estrogen (CEE) and 2.5mg/d medroxyprogesterone (n=53) or a
placebo (n=54). After 3 years, patients treated with HRT demonstrated a 4.0% increase
in spinal BMD, while the placebo group demonstrated a 0.35 decrease in spinal BMD.
Studies performed by Ettinger et al9 and Prestwood et al10 suggested that
raloxifene increased overall BMD significantly when compared to the placebo. Ettinger
et al9 examined 7705 postmenopausal women with osteoporosis from 25 countries to
determine the effect of raloxifene on femoral neck and spine BMD. The patients were
separated into 1 of 2 subgroups. If the subject displayed a femoral neck or lumbar spine
BMD t score of less than -2.5, then they were grouped into the first study group (n=
5064). The second study group (n=2641) similarly exhibited low BMD t scores, but also
had suffered at least one fracture prior to the start of the study. Within each of these
subgroups, patients were randomized to receive either 60mg/d of raloxifene, 120mg/d of
raloxifene, or the placebo. Each patient also received daily calcium (500mg) and
cholecalciferol (400 to 600IU) supplements. At the end of the 3-year trial, the patients
receiving 60mg/d demonstrated a 2.1% increase in femoral neck BMD compared to the
placebo; patients receiving 120mg/d exhibited an increase of 2.4% when compared to the
placebo group. The spinal BMD of patients being administered 60mg/d increased by
2.6% when compared to the placebo, while the spinal BMD of patients receiving
120mg/d increased by 2.7% when compared to the placebo group.
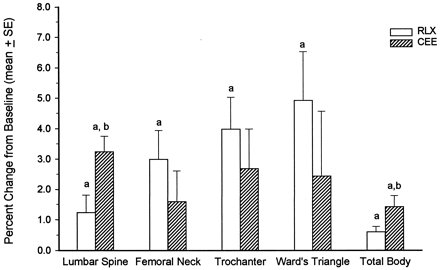
Prestwood et al10 demonstrated the effects of raloxifene and CEE on BMD when
taken separately in a phase II randomized, double-blind study. Over the course of 6
months, 51 Caucasian women who had been postmenopausal for at least 5 years prior to
the start of the study were examined. Eligible patients were between 55 and 85 years of
age and exhibited a baseline lumbar spine BMD score between 1 SD above and 3 SD
below peak bone mass. Patients received either 0.625 CEE (n=26) or 60mg raloxifene
(n=25) daily. The study showed a substantial increase in lumbar spine, femoral neck,
trochanter, and total body BMD. Theses increases can be seen in Figure 1.
Figure 1. BMD changes from baseline of patients receiving 60mg/d raloxifene (RLX) or 0.625mg/d CEE for 6 months. From: J Clin Endocrinol Metab. 2000;85:2197-2202.
Bone and colleagues11 researched the efficacy of alendronate, CEE, alendronate
and CEE, and a placebo in elevating BMD. A 2-year study including 425
postmenopausal women showed that alendronate when administered daily in amounts of
10mg increased lumbar spine BMD by 6.0%. The lumbar spine BMD decreased by 0.6%
in the placebo group. Downs et al12 performed a randomized study of 299 women ranging
in age from 45 to 84 who had been postmenopausal for at least 5 years and had been
diagnosed with osteoporosis. Researchers administered either 10mg/d of alendronate,
200mg IU/d calcitonin, or a placebo to patients in 24 centers across the United States.
BMD increases were observed in patients receiving either alendronate or calcitonin.
Patients receiving calcitonin experienced an increase in BMD of 1.18% in the lumbar
spine, 0.47% in the trochanter, and 0.58% in the femoral neck. However, more
substantial increases were noted in the alendronate group with BMD increases of 5.16%,
4.73%, and 2.78% in the spine, trochanter, and neck respectively.
Greenspan and colleagues13 examined the effects of a weekly alendronate dosing
on BMD in a 2-year double-blind study. Patients (n=1258) were postmenopausal women
between the ages of 42 and 95 and exhibited a lumbar spine or femoral neck BMD t score
of -2.5, which is characteristic of osteoporosis sufferers. Patients were randomized to
receive 70mg alendronate once a week (n=519), 35mg alendronate twice a week (n=369),
or 10mg alendronate every day (n=370). Results indicated that lumbar spine BMD
increased by 6.8%, 7.0%, and 7.4% in the group receiving alendronate once a week,
twice a week, and everyday respectively. Increases of 4.1%, 4.3%, and 4.3% in total hip
BMD were seen in the once-weekly, twice-weekly, and daily treatment groups
In a study14 of 36 patients receiving 30mg weekly risedronate, BMD increases of
1.9% and 2.1% were observed in the trochanter and hip respectively. Patients between
the ages of 46 and 86 also received daily supplements of 400IU/d of vitamin D and
1200mg/d of calcium. Similar results were noted in a 3-year randomized double-blind
study conducted by Harris and colleagues15 of 2458 ambulatory postmenopausal women.
Eligible subjects were younger than 85 and had sustained 2 or more radiographically
identified vertebral fractures (T4-L4, inclusive) or 1 vertebral fracture and low lumbar-
spine (L1-L4) BMD (defined as 0.83 g/cm2 [Hologic instrument] or 0.94 g/cm2 [Lunar
instrument]). Eligible patients were postmenopausal for at least 5 years prior to the start
of the study. Patients were randomized to receive 2.5mg/d risedronate, 5.0mg/d
risderonate, or a placebo. After the first year, the 2.5mg/d risedronate group was dropped
from the study due to an amendment to the protocol that was not further explained in the
study. Those patients receiving 5mg of risedronate a day exhibited an increase in lumbar
spine BMD of 5.4% compared to the 1.1% increase observed in placebo patients.
Femoral neck BMD increased by 1.6% in risedronate-receiving patients and decreased by
1.2% in placebo-receiving patients. Femoral trochanter BMD increased by 3.3% in the
risedronate group and decreased by 0.7% in the placebo group.
Decrease in Bone Turnover Markers
The Villareal et al7 study of 67 women with mild to moderate physical frailty
observed the alterations in such bone turnover markers as bone-specific alkaline
phosphatase (BSAP) and urine N-telopeptide (NTx). Patients in this study either
received 0.625mg/d of conjugated estrogen with 5mg/d of medroxyprogesterone for 13
days every 3 months or a placebo. Results of the study indicated that HRT reduced
BSAP levels by 24%. Urine N-telopeptide levels decreased by 48% in patients
Levels of urinary cross-linked N- and C- telopeptides of type I collagen (NTx and
CTx respectively) and deoxypyridinoline cross-links (DPYr) were observed by
Prestwood and colleagues.10 In this study, 51 women with a baseline lumbar spine BMD
score between 1 SD above and 3 SDs below peak bone mass were followed for 3 years.
Patients received either 0.625mg/d of CEE or 60mg/d of raloxifene. CTx levels
decreased by 23% in the raloxifene group. Similarly, NTx levels decreased by 22% with
raloxifene. Raloxifene demonstrated a potential to decrease DPYr by 16%.
Alendronate’s efficacy in abating bone turnover markers was researched by
Downs et al.12 In this study of 299 postmenopausal women, patients either received
10mg/d of alendronate, 200mg IU/d calcitonin, or a placebo. A 43% decrease of BSAP
levels in the alendronate group was observed compared to a 2% reduction in the placebo
group. Furthermore, alendronate reduced urinary NTx by 62%.
Raisz and colleagues16 investigated the short-term effects of risedronate on
biochemical markers of bone turnover, including DPYr, NTx, and CTx, in
postmenopausal women. An overall decrease in the resorption markers was observed.
DPYr decreased by 28%, NTx by 61%, and CTx by 73% after 2 weeks of treatment.
Decreased Fracture Risk
study17 conducted by the Women’s Health Initiative (WHI) monitored 16 608
postmenopausal women with intact uteruses aged 50-79 to determine the effects of HRT
on fracture risk. The study lasted from 1997-2002. A woman was considered
postmenopausal if she had failed to experience vaginal bleeding for 6 months prior to the
start of the study, had undergone a hysterectomy, or had ever used postmenopausal
medication, including HRT, raloxifene, alendronate, and risedronate. Patients either
received CEE, 0.625 mg/d, plus medroxyprogesterone acetate, 2.5 mg/d, in 1 tablet or a
placebo. Those patients that received HRT (n=8506) suffered from one third fewer hip
and clinical vertebral fractures than the patients receiving placebo (n=8102). An overall
decrease of 24% in total fractures was observed in the HRT group.
The Ettinger et al9 study of 7705 women separated into 2 different groups based
on the presence or absence of previous vertebral fractures (n=2641 and n=5064,
respectively) illustrated a reduced relative risk (RR) of 0.7 for vertebral fracture in those
patients receiving raloxifene versus those who received the placebo. The study groups
received either 60mg/d (group 1) or 120mg/d (group 2) of raloxifene. Both groups
displayed a decreased incidence of new vertebral fractures. No difference between the
preventative effects of 60mg/d raloxifene or 120mg/d raloxifene was observed when the
data from group 1 and 2 were combined. However, when the data from group 2 was
analyzed by itself, a difference in raloxifene’s preventative effects was found. Women in
study group 2 receiving 120mg/d raloxifene displayed a lower incidence of vertebral
fractures (10.7%) than the women in study group 1 receiving 60mg/d raloxifene (14.7%).
The incidence of nonvertebral fractures, including wrist and hip fractures, was not
Over a period of 4 years, the effects of alendronate on fracture risk in low BMD
women were researched by Cummings and colleagues.18 Limitations restricted the
eligible test population to women with less than 0.68g/cm2 in femoral neck BMD and
without a previous vertebral fracture. A cohort of 4432 women, ranging in age from 54
to 81, participated in this 2-year randomized, blinded, and placebo-controlled study in
which patients received alendronate (n=2214) or a placebo (n=2218). During the first 2
years, alendronate patients received 5mg/d. However, after 2 years, the dosage was
increased to 10mg/d due to other research which suggested that more substantial
increases in BMD could be seen with 10mg/d. In alendronate patients, results indicated a
36% decrease in clinical fractures (RH=0.64, 95% CI) in women with baseline femoral
neck BMD t scores of less than -2.5. Women with baseline femoral neck BMD t scores
greater than -2.0 SDs demonstrated a 22% decrease in the risk for clinical fractures. A
44% decrease in vertebral fracture risk was observed in women with baseline femoral
Black et al19 generated similar fracture reduction results in an approximately 3-
year study of 3658 women who had been postmenopausal for at least 2 years prior to the
start of the study. Eligible women had to exhibit baseline femoral neck BMD equal to or
less than 0.68 g/cm2 and were separated into 1 of 2 study groups. The vertebral fracture
arm (n=2027) contained women who had previously suffered from a vertebral fracture,
while the clinical fracture arm (n=1631) included women without previous histories of
vertebral fractures. All women were given alendronate, and only those women whose
baseline calcium intake was below 1000mg/d were given daily supplements of 500mg
elemental calcium and 250IU of vitamin D. The original 5mg/d dosage of alendronate
was changed to 10mg/d 2 years into the study due to other research which suggested that
more substantial increases in BMD could be seen with 10mg/d. An overall decrease of
48% (RR=0.52, 95% CI) in radiological vertebral fractures was observed when the data
from study group 1 and 2 were combined. In the 2 alendronate groups combined, the risk
for multiple vertebral fractures was reduced by 87% (RR=0.13), for clinical vertebral
fractures by 45% (RR=0.55), and for hip fractures by 53% (RR=0.47).
The ability of risedronate to reduce the risk of fractures was investigated by
Harris et al.15 A cohort of 2458 ambulatory postmenopausal women were examined in
this 3-year randomized double-blind study in which patients either received 2.5mg/d
risedronate, 5mg/d risedronate, or a placebo. After the first year, the 2.5mg/d risedronate
group was dropped from the study due to an amendment of the protocol that was not
further explained in the study. After 1 year, the vertebral fracture risk was decreased by
65% in those patients taking 5mg/d risedronate. The chance of vertebral fractures was
decreased by 41% in the 5mg/d risedronate group following 3 years of treatment. After 3
years of treatment, women taking 5mg/d risedronate illustrated a 39% decrease in non-
vertebral fracture risk compared to the placebo.
Side Effects Hormone Replacement Therapy versus Raloxifene
An increased risk for breast cancer was noted in patients using HRT to treat
osteoporosis,17 while a decreased risk was associated with raloxifene.9 The WHI17 study
lasted 5 years and included 16 608 postmenopausal women with intact uteruses. Results
revealed a 26% increase in breast cancer risk in HRT patients. The Ettinger9 study of
7705 postmenopausal women with osteoporosis found a RR of 0.3 for raloxifene patients.
Several studies9,17 examined the probability of incurring other cancers, including
colorectal and endometrial. HRT reduced the risk for colorectal cancer by 37%.17 A
raloxifene trial9 discovered endometrial cancer in 4 women out of 2557 women in the
60mg/d group, in 2 women out of 2572 women in the 120mg/d group, and in 4 women
Pulmonary embolism/deep vein thrombophlebitis
When used separately, HRT and raloxifene exhibit similar effects on the risk for
pulmonary embolism or deep vein thrombophlebitis.9,17 WHI noted that the risk for
pulmonary embolism and deep vein thrombophlebitis individually was twofold greater
for patients taking HRT than those not taking it.17 Studies executed by Ettinger et al9
indicate that during the study 8 patients receiving the placebo experienced either
pulmonary embolism or deep vein thrombophlebitis compared to 25 and 24 patients in
the 60mg/d and 120mg/d raloxifene groups respectively. Raloxifene, regardless of dose,
imposes a RR for deep vein thrombophlebitis of 3.1 (95% CI) on its users.
Cardiovascular Disease and Serum Levels
In the WHI study,17 HRT was shown to elevate the risk for any CHD by 22%.
However, in a double-blind randomized, parallel trial in which Walsh et al20 examined
390 postmenopausal women, HRT and raloxifene seemed to decrease the risk of CHD.
Patients received 60mg/d raloxifene, 120mg/d raloxifene, HRT (conjugated equine
estrogen, 0.625 mg/d, and medroxyprogesterone acetate, 2.5 mg/d), or a placebo. HRT
was found to reduce LDL-C by 14%. Furthermore, it increased HDL2-cholesterol by
33% and HDL-C by 11%. Triglyceride levels increased by 22% as a result of HRT
treatment. This study also suggested that both doses of raloxifene demonstrated a less
substantial increase in these factors than HRT. Raloxifene reduced LDL-C levels by
12%, increased HDL2-cholesterol levels by 15%, and exhibited no statistically significant
effect on HDL-C or triglyceride levels when compared to placebo.
Alendronate versus Risedronate
Bisphosphonates seem to induce limited adverse side effects, among which are
upper gastrointestinal ulcers and upper GI mucosal changes. A study conducted by
Lanza and colleagues5 suggested that gastric ulcers occurred in 13.2% of the group
receiving alendronate. The Lanza et al5 study examined 515 postmenopausal women who
were randomized to receive 5mg/d risedronate, or 10mg/d alendronate for 2 weeks.
While reviewing the effects of alendronate and risedronate on the upper gastrointestinal
tract, Lanza and colleagues5 observed 3 alendronate patients with esophageal ulcers, 1
alendronate patient with a duodenal ulcer, no esophageal ulcers in risedronate patients,
and 2 duodenal ulcers in risedronate patients. The Lanza et al21 study included men and
postmenopausal women who received either 40 mg/d alendronate (n=90), 30 mg/d
risedronate (n = 89), or placebo with aspirin 650 mg for the last 7 days (n = 20). Both the
alendronate and risedronate group demonstrated decreased gastroduodenal irritation when
compared to the group receiving a placebo and aspirin.
In the study by Harris et al,15 4.2% of the women in the 5mg/d risedronate group
complained of gastrointestinal adverse effects and decided to undergo gastrointestinal
tract endoscopy. Similarly, 3.7% of the placebo group complained of the same
gastrointestinal adverse effects and underwent gastrointestinal tract endoscopy. Nine
cases of duodenitis in risedronate patients compared to 2 in the placebo group were
noted. Duodenal ulcers appeared in 1 patient undergoing risedronate treatment, while
they appeared in 3 placebo-receiving patients.
In a 10 week study conducted by Lanza and colleagues22, the tolerability of a
weekly alendronate dose was examined. A cohort of 277 men (n=90) and women
(n=187) participated in this parallel, double-blind, placebo-controlled study. Subjects
were between the ages of 45 and 80 and had suffered no recent gastrointestinal diseases
prior to the start of the study. Each patient was randomly assigned to receive 70mg of
alendronate once a week (n=126), a placebo once a week (n=126), or a weekly placebo
for the first 9 weeks and a weekly placebo followed by 650mg of aspirin during the last
week (n=25) in order to generate a positive control and to actually observe lesions. In
order to ensure blinding, patients not receiving aspirin during the last week were given
placebos that were similar in appearance to aspirin. As part of the methodology, patients
took their medication in the morning before eating or drinking anything. Additionally,
patients drank a full glass of water with the medication and remained upright for at least
30 minutes after the medication and before eating or drinking anything. Various scales
were followed in order to evaluate patients’ endoscopic condition following treatment.
Table 1. Endoscopic scale used to evaluate patients’ conditions following treatment. From: Am J Gastroenterol. 2002; 97(1):58-64.
Results obtained from the alendronate and placebo group displayed similar mean gastric
erosion scores with the alendronate group exhibiting a mean score of 0.32 and the
placebo group illustrating a mean score of 0.35. Figure 2 and 3 respectively display the
gastric erosion and duodenal erosion scores of patients in each of the treatment groups.
Figure 2. Distribution of gastric erosion scores at the final endoscopy. From: Am J Gastroenterol. 2002; 97(1):58-64.
Figure 3. Distribution of duodenal erosion scores at the final endoscopy. From: Am J Gastroenterol. 2002; 97(1):58-64.
Lanza and colleagues22 concluded that a weekly dose of 70mg is well tolerated and would
increase patient compliance. The lack of gastric or duodenal adverse side effects was
attributed to the patients’ adherence to the dosing instructions of alendronate.
COMMENTS
The efficacy of each drug was evaluated in terms of its ability to increase BMD,
decrease bone turnover markers, reduce fracture risk, and impart minimal side effects on
its user. Highly efficacious agents are those that accomplish all 4 of these tasks. Studies
conducted by Villareal et al7 and Recker et al8 noted an increase in lumbar spine and total
hip BMD in those patients treated with hormone replacement therapy. Not only do the
studies agree on the ability of hormone replacement therapy to increase BMD, but also on
the magnitude of HRT’s ability to increase lumbar spine BMD with Villareal et al7
documenting a 4.3% increase and Recker et al8 noting a 4.0% increase. Raloxifene’s
ability to increase femoral neck, lumbar spine, trochanter, and total BMD was proven by
Ettinger et al9 and Prestwood et al.10 Bone and colleagues,11 Downs et al,12 and
Greenspan13 found alendronate to be an efficacious agent in terms of its ability to
increase lumbar spine, trochanter, and femoral neck BMD. Risedronate’s ability to
elevate trochanter, hip, lumbar spine, and femoral neck BMD was documented by
Delaney et al14 and Harris et al.15 All of the drugs exhibited similar effects on BMD with
no drug displaying substantially higher BMD increases than another. Furthermore, each
of the drugs only exhibited a minimal increase in BMD with the greatest increase being
6.0%.11 These minimal increases can be attributed to the focus of antiresorptive drugs on
inhibiting osteoclast activity, not stimulating osteoblasts to reform bone.
studies7,10,12,16 noted a decrease in bone turnover markers in patients taking
hormone replacement therapy, raloxifene, alendronate, or risedronate. Since all the
studies7,10,12,16 on bone turnover markers examined the change in urine N-telopeptide, the
ability of each drug to decrease the concentration of this marker was used to evaluate the
efficacy of each drug. Villareal et al7 found a 48% decrease of urine N-telopeptide in
patients taking hormone replacement therapy, while Prestwood et al10 only documented a
22% decrease of urine N-telopeptide in those patients taking raloxifene. The drastic
difference between these percentages suggests that hormone replacement therapy is more
effective than raloxifene at reducing bone turnover markers. Alendronate was shown by
Downs et al12 to decrease urine N-telopeptide by 62%. Similarly, risedronate was found
to decerease urine N-telopeptide by 61%.16 Alendronate and risedronate seem to be
comparable and better than hormone replacement therapy and raloxifene in their ability to
Each drug was shown to decrease the risk of fractures.9,15,17-19 However, hormone
replacement therapy, alendronate, and risedronate all appear to have a heightened effect
on fracture risk when compared to raloxifene. Hormone replacement therapy reduced the
risk of vertebral fractures by one third,17 while alendronate was shown to decrease
vertebral fracture risk by 44%18 and 45%.19 Risedronate decreased fracture risk by 41%.15
Raloxifene was only shown to reduce the risk of vertebral fractures by 14.7%.9 The
disparity in these percentages suggests that when used separately, hormone replacement
therapy, alendronate, or risedronate demonstrate a greater reduction in fracture risk than
raloxifene. In order to more effectively compare these drugs in terms of their ability to
decrease fracture risk, a study involving and comparing all 4 drugs would need to be
The most drastic differences between the drugs were seen in their potential side
effects. Hormone replacement therapy was found to increase the risk of breast cancer by
26%17, while raloxifene was shown to impart a RR of 0.3 on its users.9 In studies9,17
examining the incidence of pulmonary embolism or deep vein thrombophlebitis, it was
found that when used separately, both hormone replacement therapy and raloxifene
drastically increased the risk for these conditions. The effect of hormone replacement
therapy on cardiovascular disease is inconclusive due to the variable results obtained
from two studies.17,20 While the WHI study17 found an elevated risk of 22% for any CHD
in those patients taking hormone replacement therapy, Walsh et al20 noted a favorable
change in serum levels and subsequently a preventative effect of HRT on cardiovascular
disease. The cohort size of the WHI study17 was 16 608 postmenopausal women, while
the Walsh et al study20 only included 390 postmenopausal women. The larger cohort size
in the WHI study17 suggests more accurate results. Furthermore, the WHI study17 lasted
for 5 years as opposed to the Walsh et al study20 which terminated after 6 months. Walsh
et al20 similarly observed a substantial decrease in the serum levels of patients taking
Alendronate and risedronate, individually, failed to demonstrate any adverse or
beneficial side effects. Although one study conducted by Lanza and colleagues5
observed gastric ulcers in 13.2% of the group taking 10mg/d alendronate, this study was
only conducted for 2 weeks, which may explain the prevalence of these gastric ulcers.
Other studies15,21,22 have shown that no substantial difference exists between the
prevalence of gastrointestinal adverse effects in the placebo and in either the alendronate
or risedronate group. The lack of adverse side effects in patients taking alendronate or
risedronate suggests that they may be more tolerable and suitable than hormone
replacement therapy and raloxifene for patients suffering from osteoporosis.
In order to prescribe the most suitable medication, practitioners must examine the
patient’s medical history. Those patients that demonstrate a predisposition for breast
cancer or high blood pressure should abstain from taking hormone replacement therapy
or raloxifene and instead try alendronate or risedronate. For those patients who suffer
from gastrointestinal problems, hormone replacement therapy or raloxifene may be the
best option, although it is possible to take risedronate or alendronate if the patient
complies with the strict dosing instructions. In order to ensure that gastrointestinal side
effects do not arise in patients taking either alendronate or risedronate, it is imperative
that patients take the medication in the morning before eating or drinking anything.
Furthermore, patients must drink a full glass of water with the medication and remain
upright for at least 30 minutes after the medication and before eating or drinking
anything.22 These strict dosing instructions may affect patient compliance. Due to
alendronate’s and risedronate’s mode of action, those patients with renal insufficiencies
should not take alendronate or risedronate to treat their osteoporosis. Patients whose
kidneys filter CrCl at a rate lower than 35ml/min or CrCl at rate lower than 30mL/min
should not take alenronate or risedronate respectively.23
Although a patient’s medical history should be the determining factor when
deciding which antiresorptive drug to use to treat their osteoporosis, alendronate seems to
be the most efficacious agent. When administered on a weekly basis, alendronate has
been proven to be as effective as daily alendronate doses.13 Furthermore, Lanza and
colleagues22 have found once-weekly alendronate to be tolerable. Since alendronate
increases BMD, decreases bone turnover markers, reduces fracture risk, imparts limited if
any side effects on its users, and is convenient, weekly alendronate seems to be the most
efficacious antiresorptive agent for the treatment of osteoporosis.
In order to identify the most efficacious antiresorptive drug, further studies need
to be conducted to examine the effect of hormone replacement therapy and raloxifene
when taken separately on the risk for cardiovascular disease. Furthermore, studies
evaluating the efficacy and tolerability of weekly risedronate samples may provide
patients with an alternative to weekly alendronate.
REFERENCES
1. Fast Facts on Osteoporosis. National Institutes of Health Osteoporosis and
Related Bone Diseases-National Resource Center. Available at: http://www.osteo.org/newfile.asp?doc=fast&doctitle=Fast+Facts+on+Osteoporosis&doctype=HTML+Fact+Sheet. Accessed March 16, 2003.
2. Medications to Prevent and Treat Osteoporosis. National Osteoporosis
Foundation. Available at: http://www.nof.org/patientinfo/medications.htm. Accessed March 18, 2003.
3. Silverthorn DU, Ober WC, Garrison CW, Silverthorn AC. Energy balance,
metabolism, and growth. In: Human Physiology: An Integrated Approach. 2nd ed. Upper Saddle River, NJ: Prentice Hall; 2001:672-680.
4. Smith EL, Rose D. Selected Annotated Bibliography. Southern Medical Journal.
5. Lanza FL, Hunt RH, Alan B, et al. Endoscopic comparison of esophageal and
gastroduodenal effects of risedronate and alendronate in postmenopausal women. Gastroenterology. 2000;119:631-638.
6. Anthony M, Williams JK, Dunn BK. What would be the properties of an Ideal
SERM? Annals of the New York Academy of Sciences.2001;949:261-278.
7. Villareal DT, Binder EF, Williams DB, Schechtman KB, Yarasheski KE, Kohrt
WM: Bone mineral density response to estrogen replacement in frail elderly women: A randomized controlled trial. JAMA. 2001;286:815-820.
8. Recker RR, Davies KM, Dowd RM, Heaney RP. The effect of low-dose
continuous estrogen and progesterone therapy with calcium and vitamin D on bone in elderly women: A randomized, controlled trial. Ann Intern Med. 1999;130:897-904.
9. Ettinger, B, Black BH, Mitlak, et al: Reduction of vertebral fracture risk in
postmenopausal women with osteoporosis treated with raloxifene. Results from a 3-year randomized clinical trial. JAMA. 1999;282: 637-645.
10. Prestwood KM, Gunness M, Muchmore DB, et al: A comparison of the effects of
raloxifene and estrogen on bone in postmenopausal women. J Clin Endocrinol Metab. 2000;85:2197-2202.
11. Bone HG, Greenspan SL, McKeever C, et al : Alendronate and estrogen effects in
postmenopausal women with low bone mineral density. J Clin Endocrinol Metab. 2000;85:720-726.
12. Downs RW Jr. Bell NH, Ettinger MP, et al : Comparison of alendronate and
intranasal calcitonin for treatment of osteoporosis in postmenopausal women. J Clin Endocrinol Metab. 2000;85:1783-1788.
13. Greenspan SL, Bone G 3rd, Schnitzer TJ, Watts NB, Adami S, Foldes AJ, Roux
C, Levine MA, Uebelhart B, Santora AC 2nd, Kaur A, Peverly CA, Orloff JJ, Rizzoli R; Alendronate Once-Weekly Study Group: Two-year results of once-weekly administration of alendronate 70 mg for the treatment of postmenopausal osteoporosis. J Bone Miner Res 2002;17(11):1988-96.
14. Delaney MF, Hurwitz S, Shaw J, LeBoff MS: Bone Density with once weekly
risedronate in postmenopausal women. J Clin Densitom. 2003;6(1):45-50.
15. Harris ST, Watts NB, Genant HK, et al for the Vertebral Efficacy With
Risedronate Therapy (VERT) Study Group. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. JAMA. 1999;282:1344-1352.
16. Raisz L, Smith JA, Trahiotis M, Fall P, Shoukri K, Digennaro J, Sacco-Gibson N:
Short-term risedronate treatment in postmenopausal women: effects on biochemical markers of bone turnover. Osteoporos Int 2000;11(7):615-620.
17. Writing Group for the Women’s Health Initiative: Risks and benefits of estrogen
plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321-33.
18. Cummings SR, Eckert S, Krueger KA, et al for the Multiple Outcomes of
Raloxifene Evaluation trial. The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. JAMA. 1999;281:2189-2197.
19. Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC,
Nevitt MC, Suryawanshi S, Cummings SR, and for the FIT research group: Fracture risk reduction with alendronate in women with osteoporosis: The fracture intervention trial. J Clin Endocrinol Metab. 2000;85(11):4118-4124.
20. Walsh BW MD, Kuller LH MD, Wild RA MD, Paul S PhD, Farmer M MD,
Lawrence JB MD, Shah AS PhD, Anderson PW MD: Effects of raloxifene on serum lipids and coagulation factors in healthy postmenopausal women. JAMA. 1998; 279:1445-1451.
21. Lanza F, Schwartz H, Sahba B, et al : An endoscopic comparison of the effects of
alendronate and risedronate on upper gastrointestinal mucosae. Am J Gastroenterol. 2000; 95:634-640.
22. Lanza F, Sahba B, Schwartz H, Winograd S, Torosis J, Quan H, Reyes R,
Musliner T, Daifotis A, Leung A: The upper GI safety and tolerability of oral alendronate at a dose of 70 milligrams once weekly: a placebo-controlled endoscopy study. Am J Gastroenterol. 2002; 97(1):58-64.
23. Espirito J: Bisphosphonates for the Prevention and Treatment of Postmenopausal
Osteoporosis. Drug Therapy Topics. 2002;31(5):25-30.
plasma lev els (usu ally fol low ing rapid IV bolus) (MW 225.2; as sodium salt for IV infusion MW 247.2)and pre-ex ist ing re nal dis ease. Note: Crys tal li - Syn onyms: Acyclovir, Acycloguanosine. za tion oc curs ex clu sively af ter (rapid) IV ad - Usual dos age: Size of dose and dos age in ter -min is tra tion (re nal ac cu mu la tion of the drug). val de pend on route of ad min is tr
Univ.-Prof. Doz. (ETH) Dr. Anton Amann “FEM_PERS bietet Schülerinnen und Schülern die phantastische Chance, mit WissenschafterInnen der Österreichischen Akademie der Wissenschaften aktiv an einem medizinischen Forschungsprojekt mitzuarbeiten. Somit werden durch Sparkling Science die Karrierewege in naturwissenschaftliche und medizinische Studien geebnet.” FEM_PERS Entwicklun
 placebo; patients receiving 120mg/d exhibited an increase of 2.4% when compared to the
placebo group. The spinal BMD of patients being administered 60mg/d increased by
2.6% when compared to the placebo, while the spinal BMD of patients receiving
120mg/d increased by 2.7% when compared to the placebo group.
Prestwood et al10 demonstrated the effects of raloxifene and CEE on BMD when
taken separately in a phase II randomized, double-blind study. Over the course of 6
months, 51 Caucasian women who had been postmenopausal for at least 5 years prior to
the start of the study were examined. Eligible patients were between 55 and 85 years of
age and exhibited a baseline lumbar spine BMD score between 1 SD above and 3 SD
below peak bone mass. Patients received either 0.625 CEE (n=26) or 60mg raloxifene
(n=25) daily. The study showed a substantial increase in lumbar spine, femoral neck,
trochanter, and total body BMD. Theses increases can be seen in Figure 1.
Figure 1. BMD changes from baseline of patients receiving 60mg/d raloxifene (RLX) or 0.625mg/d CEE for 6 months. From: J Clin Endocrinol Metab. 2000;85:2197-2202.
Bone and colleagues11 researched the efficacy of alendronate, CEE, alendronate
and CEE, and a placebo in elevating BMD. A 2-year study including 425
postmenopausal women showed that alendronate when administered daily in amounts of
10mg increased lumbar spine BMD by 6.0%. The lumbar spine BMD decreased by 0.6%
in the placebo group. Downs et al12 performed a randomized study of 299 women ranging
in age from 45 to 84 who had been postmenopausal for at least 5 years and had been
diagnosed with osteoporosis. Researchers administered either 10mg/d of alendronate,
200mg IU/d calcitonin, or a placebo to patients in 24 centers across the United States.
BMD increases were observed in patients receiving either alendronate or calcitonin.
Patients receiving calcitonin experienced an increase in BMD of 1.18% in the lumbar
spine, 0.47% in the trochanter, and 0.58% in the femoral neck. However, more
substantial increases were noted in the alendronate group with BMD increases of 5.16%,
4.73%, and 2.78% in the spine, trochanter, and neck respectively.
Greenspan and colleagues13 examined the effects of a weekly alendronate dosing
on BMD in a 2-year double-blind study. Patients (n=1258) were postmenopausal women
between the ages of 42 and 95 and exhibited a lumbar spine or femoral neck BMD t score
of -2.5, which is characteristic of osteoporosis sufferers. Patients were randomized to
receive 70mg alendronate once a week (n=519), 35mg alendronate twice a week (n=369),
or 10mg alendronate every day (n=370). Results indicated that lumbar spine BMD
increased by 6.8%, 7.0%, and 7.4% in the group receiving alendronate once a week,
twice a week, and everyday respectively. Increases of 4.1%, 4.3%, and 4.3% in total hip
placebo; patients receiving 120mg/d exhibited an increase of 2.4% when compared to the
placebo group. The spinal BMD of patients being administered 60mg/d increased by
2.6% when compared to the placebo, while the spinal BMD of patients receiving
120mg/d increased by 2.7% when compared to the placebo group.
Prestwood et al10 demonstrated the effects of raloxifene and CEE on BMD when
taken separately in a phase II randomized, double-blind study. Over the course of 6
months, 51 Caucasian women who had been postmenopausal for at least 5 years prior to
the start of the study were examined. Eligible patients were between 55 and 85 years of
age and exhibited a baseline lumbar spine BMD score between 1 SD above and 3 SD
below peak bone mass. Patients received either 0.625 CEE (n=26) or 60mg raloxifene
(n=25) daily. The study showed a substantial increase in lumbar spine, femoral neck,
trochanter, and total body BMD. Theses increases can be seen in Figure 1.
Figure 1. BMD changes from baseline of patients receiving 60mg/d raloxifene (RLX) or 0.625mg/d CEE for 6 months. From: J Clin Endocrinol Metab. 2000;85:2197-2202.
Bone and colleagues11 researched the efficacy of alendronate, CEE, alendronate
and CEE, and a placebo in elevating BMD. A 2-year study including 425
postmenopausal women showed that alendronate when administered daily in amounts of
10mg increased lumbar spine BMD by 6.0%. The lumbar spine BMD decreased by 0.6%
in the placebo group. Downs et al12 performed a randomized study of 299 women ranging
in age from 45 to 84 who had been postmenopausal for at least 5 years and had been
diagnosed with osteoporosis. Researchers administered either 10mg/d of alendronate,
200mg IU/d calcitonin, or a placebo to patients in 24 centers across the United States.
BMD increases were observed in patients receiving either alendronate or calcitonin.
Patients receiving calcitonin experienced an increase in BMD of 1.18% in the lumbar
spine, 0.47% in the trochanter, and 0.58% in the femoral neck. However, more
substantial increases were noted in the alendronate group with BMD increases of 5.16%,
4.73%, and 2.78% in the spine, trochanter, and neck respectively.
Greenspan and colleagues13 examined the effects of a weekly alendronate dosing
on BMD in a 2-year double-blind study. Patients (n=1258) were postmenopausal women
between the ages of 42 and 95 and exhibited a lumbar spine or femoral neck BMD t score
of -2.5, which is characteristic of osteoporosis sufferers. Patients were randomized to
receive 70mg alendronate once a week (n=519), 35mg alendronate twice a week (n=369),
or 10mg alendronate every day (n=370). Results indicated that lumbar spine BMD
increased by 6.8%, 7.0%, and 7.4% in the group receiving alendronate once a week,
twice a week, and everyday respectively. Increases of 4.1%, 4.3%, and 4.3% in total hip

















 BMD were seen in the once-weekly, twice-weekly, and daily treatment groups
In a study14 of 36 patients receiving 30mg weekly risedronate, BMD increases of
1.9% and 2.1% were observed in the trochanter and hip respectively. Patients between
the ages of 46 and 86 also received daily supplements of 400IU/d of vitamin D and
1200mg/d of calcium. Similar results were noted in a 3-year randomized double-blind
study conducted by Harris and colleagues15 of 2458 ambulatory postmenopausal women.
Eligible subjects were younger than 85 and had sustained 2 or more radiographically
identified vertebral fractures (T4-L4, inclusive) or 1 vertebral fracture and low lumbar-
spine (L1-L4) BMD (defined as 0.83 g/cm2 [Hologic instrument] or 0.94 g/cm2 [Lunar
instrument]). Eligible patients were postmenopausal for at least 5 years prior to the start
of the study. Patients were randomized to receive 2.5mg/d risedronate, 5.0mg/d
risderonate, or a placebo. After the first year, the 2.5mg/d risedronate group was dropped
from the study due to an amendment to the protocol that was not further explained in the
study. Those patients receiving 5mg of risedronate a day exhibited an increase in lumbar
spine BMD of 5.4% compared to the 1.1% increase observed in placebo patients.
Femoral neck BMD increased by 1.6% in risedronate-receiving patients and decreased by
1.2% in placebo-receiving patients. Femoral trochanter BMD increased by 3.3% in the
risedronate group and decreased by 0.7% in the placebo group.
Decrease in Bone Turnover Markers
BMD were seen in the once-weekly, twice-weekly, and daily treatment groups
In a study14 of 36 patients receiving 30mg weekly risedronate, BMD increases of
1.9% and 2.1% were observed in the trochanter and hip respectively. Patients between
the ages of 46 and 86 also received daily supplements of 400IU/d of vitamin D and
1200mg/d of calcium. Similar results were noted in a 3-year randomized double-blind
study conducted by Harris and colleagues15 of 2458 ambulatory postmenopausal women.
Eligible subjects were younger than 85 and had sustained 2 or more radiographically
identified vertebral fractures (T4-L4, inclusive) or 1 vertebral fracture and low lumbar-
spine (L1-L4) BMD (defined as 0.83 g/cm2 [Hologic instrument] or 0.94 g/cm2 [Lunar
instrument]). Eligible patients were postmenopausal for at least 5 years prior to the start
of the study. Patients were randomized to receive 2.5mg/d risedronate, 5.0mg/d
risderonate, or a placebo. After the first year, the 2.5mg/d risedronate group was dropped
from the study due to an amendment to the protocol that was not further explained in the
study. Those patients receiving 5mg of risedronate a day exhibited an increase in lumbar
spine BMD of 5.4% compared to the 1.1% increase observed in placebo patients.
Femoral neck BMD increased by 1.6% in risedronate-receiving patients and decreased by
1.2% in placebo-receiving patients. Femoral trochanter BMD increased by 3.3% in the
risedronate group and decreased by 0.7% in the placebo group.
Decrease in Bone Turnover Markers 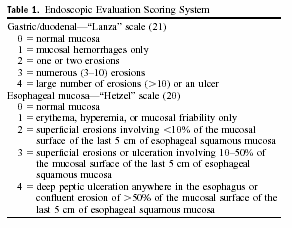
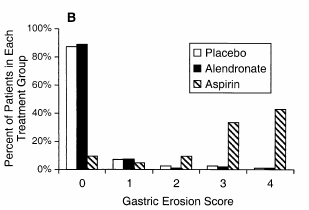
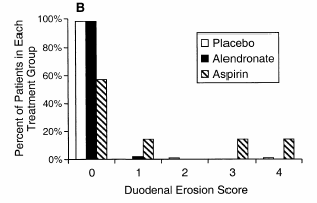 Table 1. Endoscopic scale used to evaluate patients’ conditions following treatment. From: Am J Gastroenterol. 2002; 97(1):58-64.
Results obtained from the alendronate and placebo group displayed similar mean gastric
erosion scores with the alendronate group exhibiting a mean score of 0.32 and the
placebo group illustrating a mean score of 0.35. Figure 2 and 3 respectively display the
gastric erosion and duodenal erosion scores of patients in each of the treatment groups.
Figure 2. Distribution of gastric erosion scores at the final endoscopy. From: Am J Gastroenterol. 2002; 97(1):58-64.
Figure 3. Distribution of duodenal erosion scores at the final endoscopy. From: Am J Gastroenterol. 2002; 97(1):58-64.
Lanza and colleagues22 concluded that a weekly dose of 70mg is well tolerated and would
increase patient compliance. The lack of gastric or duodenal adverse side effects was
attributed to the patients’ adherence to the dosing instructions of alendronate.
COMMENTS
Table 1. Endoscopic scale used to evaluate patients’ conditions following treatment. From: Am J Gastroenterol. 2002; 97(1):58-64.
Results obtained from the alendronate and placebo group displayed similar mean gastric
erosion scores with the alendronate group exhibiting a mean score of 0.32 and the
placebo group illustrating a mean score of 0.35. Figure 2 and 3 respectively display the
gastric erosion and duodenal erosion scores of patients in each of the treatment groups.
Figure 2. Distribution of gastric erosion scores at the final endoscopy. From: Am J Gastroenterol. 2002; 97(1):58-64.
Figure 3. Distribution of duodenal erosion scores at the final endoscopy. From: Am J Gastroenterol. 2002; 97(1):58-64.
Lanza and colleagues22 concluded that a weekly dose of 70mg is well tolerated and would
increase patient compliance. The lack of gastric or duodenal adverse side effects was
attributed to the patients’ adherence to the dosing instructions of alendronate.
COMMENTS