He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Jhh$$$012p
Journal of Human Hypertension (2001) 15, 475–480 2001 Nature Publishing Group All rights reserved 0950-9240/01 $15.00 www.nature.com/jhh ORIGINAL ARTICLE A forced titration study of antihypertensive efficacy of candesartan cilexetil in comparison to losartan: CLAIM Study II
DG Vidt1, WB White2, E Ridley3, M Rahman4, S Harris5, J Vendetti5, EL Michelson5,R Wang5, and CLAIM Study investigators61Cleveland Clinic Foundation, Cleveland, OH, USA; 2Section of Hypertension and Clinical Pharmacology,University of Connecticut Health Center, Farmington, CT, USA; 3Medical College of VirginiaCommonwealth University, Richmond, VA, USA; 4Case Western Reserve University, Cleveland, OH, USA;5AstraZeneca LP, Chesterbrook, PA, USAAn 8-week, multicentre (72 sites in the US), double- mm Hg, and 48-h BP by 5.9/7.0 mm Hg by losartan. The blind, randomised, parallel group, forced titration study responder and control rates were numerically higher in compared the antihypertensive efficacy of candesartan the candesartan cilexetil group, but the differences did cilexetil and losartan. A total of 611 patients with essen- not reach statistical significance; the responder rates tial hypertension (diastolic blood pressure 95 to 114 were 58.8% for the candesartan cilexetil group and mm Hg) were randomised initially to candesartan cilexe- 52.1% for the losartan group and control rates were til 16 mg once daily or losartan 50 mg once daily. After 49.0% for the candesartan cilexetil group and 44.6% for 2 weeks of randomised treatment, the doses of candes- the losartan group. Overall, both treatment regimens artan cilexetil and losartan were doubled to 32 mg and were well tolerated. A total of 15 of the 611 (2.5%) 100 mg once daily and continued respectively for 6 patients withdrew from the study due to an adverse weeks. At week 8, candesartan cilexetil lowered the event, including nine (2.9%) in the candesartan cilexetil blood pressure (BP) at 24 h (trough), 6 h (peak) and 48 h group and six (2.0%) in the losartan group. In con- post dose to a significantly greater extent (P Ͻ 0.05) clusion, this forced titration study confirms that candes- than losartan: candesartan cilexetil lowered trough BP artan cilexetil is more effective in lowering BP than los- by 13.4/10.5 mm Hg, peak BP by 15.5/12.9 mm Hg and artan when compared at once daily maximum doses. 48-h BP by 10.5/9.9 mm Hg compared to a reduction of
Journal of Human Hypertension (2001) 15, 475–480 trough BP by 10.1/9.1 mm Hg, peak BP by 12.0/9.5 Keywords: candesartan cilexetil; losartan; CLAIM Study II Introduction
behaved like surmountable or partially surmount-able antagonists with a relatively short duration of
The two angiotensin II type 1 receptor blockers
action. Vanderheyden et al2 found that the dis-
(ARBs), candesartan and losartan, exhibit different
152 min for candesartan, 5 min for losartan and
angiotensin II receptor. Morsing et al1 demonstrated
that candesartan acted as an insurmountable antag-
Three previous randomised, controlled trials have
onist with a marked and long-lasting blockade of the
demonstrated greater antihypertensive effects of
vascular contractile effects of angiotensin II whereas
candesartan cilexetil over losartan. These studies
losartan and its active metabolite, EXP 3174,
either evaluated the starting doses of both drugs orused a response titration design for comparison oftheir maximum doses.3–5 A fourth study by Bakris
Correspondence: Dr Donald Vidt, Cleveland Clinic Foundation,
et al6 (CLAIM Study I) and the present study
Department of Hypertension and Nephrology, A-51, 9500 Euclid
(CLAIM Study II), are two identically designed, con-
Avenue, Cleveland, OH 44195, USA. E-mail: vidtdȰccf.org Sup-
currently conducted, double-blind, randomised for-
ported by a grant from AstraZeneca LP, Wayne, PA, USA6See Appendix
ced titration studies to provide direct comparison of
Received 24 October 2000; revised 18 December 2000; accepted
the blood pressure (BP) lowering effects at once
daily maximum doses. CLAIM Study I showed that
Candesartan cilexetil vs losartan
candesartan cilexetil lowered all the primary and
in the diastolic BP readings were required to be no
secondary BP parameters by a significantly greater
more than 5 mm Hg with additional readings perfor-
amount (P Ͻ 0.05) than losartan in 654 hypertensive
med if necessary until such consistency was obtain-
patients.6 The present report summarises the find-
ings of CLAIM Study II on 611 patients with sys-
At each visit, trough sitting diastolic (D) and sys-
tolic (S) BP (24 ± 3 h after dose), heart rate, concomi-tant medications and adverse events were recorded. An adverse event is defined as any unfavourable
Patients and methods
changes in symptoms, signs or laboratory data tem-
Patients
porally associated with the use of study medicationwhether or not considered related to the use of study
A total of 611 men or women (without child bearing
medication. In addition, peak BP (6 ± 2.5 h after
potential) between 18 and 80 years of age, with
dose) was measured at week 3 or 4 of the placebo
essential hypertension (diastolic BP (DBP) 95–114
run-in period and also at week 8 of the double-blind
mm Hg) were enrolled into the study. Major
period. The definition of a peak effect at 6 h after
exclusion criteria included systolic BP у180 mm Hg
dose was chosen as previous studies indicated that
or diastolic BP у115 mm Hg, known hypersensitiv-
the peak effect of losartan occurred approximately
ity reaction to ARBs, secondary hypertension, sever-
6 h and that of candesartan cilexetil occurred after
ely impaired liver function, significant renal impair-
4 to 8 h.8,9 The trough-to-peak ratio was determined
ment, haemodynamically significant valvular heart
from dividing the trough DBP effect by the peak DBP
disease, angina pectoris requiring more than short-
effect. Laboratory tests including blood counts, renal
acting nitrates, recent history of myocardial infarc-
and liver function tests were performed by a central
tion, coronary revascularisation procedures, stroke
laboratory (SmithKline Beecham Clinical Labor-
or transient ischaemic attack. Current use of an anti-
atories) at week 3 of the placebo run-in period and
hypertensive agent was cause for exclusion unless
also at week 8 of the double-blind period. Any
it could be discontinued safely by the first week of
abnormal laboratory values from week 8 were re-
evaluated at the 2-week follow-up visit. Study design Statistical methods
This was an 8-week, multicentre (72 sites in US),
The primary efficacy parameter was mean change
double-blind, randomised, parallel group, forced
from baseline to week 8 in trough DBP. Based on
titration study. After a 4- or 5-week single-blind, pla-
this sample size and the 1:1 randomisation scheme,
cebo run-in period, enrolled patients were random-
the study had at least 90% power to detect a true
ised centrally with a computer generated randomis-
difference in mean change from baseline in trough
ation list in a 1:1 ratio to candesartan cilexetil 16 mg
sitting diastolic BP of 2.0 mm Hg between the two
tablet once daily or losartan 50 mg once daily. After
treatment groups. This estimate assumes a standard
2 weeks of randomised treatment, the doses of can-
deviation of 7.5 mm Hg and is based on a two-tailed
desartan cilexetil and losartan were doubled and
test with ␣ = 0.05. Secondary efficacy variables
continued for 6 weeks. The patients were asked to
included change from baseline to week 8 in trough
take the study medication in the morning with no
SBP and peak SBP/DBP, proportion of responders
specific instruction regarding food. In general, food
(patients with either a DBP of Ͻ90 mm Hg or a
does not affect the absorption of candesartan and
decrease from baseline in DBP of у10 mm Hg at
has only minor effects on the AUC of losartan and
week 8) and controlled patients (DBP of Ͻ90 mm Hg
its metabolite.7 Visits were scheduled at weeks 1, 2,
at week 8), and the change from baseline BP at 48 h
4 and 8 of the 8-week double-blind treatment period.
post last dose of study medication. An analysis of
Patients were also seen 48 h following their last dose
covariance for a randomised block design was used
of study medication and 2 weeks after they discon-
to assess the primary and secondary variables, with
tinued therapy with the study medication for fol-
baseline as the covariate and the study site as the
low-up visits. Post-study treatment for hypertension
block. All data analyses are presented using the
was not instituted until after the 48-h assessment
least-squares means (LSM) and 95% confidence
intervals (CI). Efficacy analyses for trough sitting
For each patient, visits were scheduled at the
DBP, SBP were performed using an intent-to-treat
same time in the morning. Patients were instructed
approach with the last observation carried forward.
to refrain from taking the study medication on the
Efficacy analyses with peak sitting and 48 h post last
morning of clinic visits until after BP was measured.
dose BP were performed with actual values as these
All BP determinations were performed in the sitting
readings were taken at baseline and once again at
position using a mercury sphygmomanometer from
their respective and points—either at week 8 or 48 h
the right arm after the patient had sat quietly for at
after the week 8 visits. The statistical difference in
least 5 min. BP was measured 3 times at 2-min inter-
the responder and control rates between the treat-
vals and the mean value computed. The differences
ment groups at week 8 were determined using Fish-
Candesartan cilexetil vs losartan DG Vidt et al Table 1 Patient characteristics at baseline Candesartan cilexetil (n = 307)
aExpressed as mean (s.d.). bExpressed as number (%). Table 2 Least squares mean changes from baseline to week 8 in blood pressure
LSM, least squares mean. aIntent-to-treat, last-observation-carried forward population (candesartan cilexetil: n = 306; losartan: n = 303). bPatients with data available: peak sitting BP (candesartan cilexetil: n = 274; losartan: n = 266); 48-h, post-dosing BP (candesartan cilexe-til: n = 246; losartan: n = 247).
er’s exact test. Both descriptive and inferential stat-istics between treatment groups were calculated forthe primary and secondary BP parameters. Patientcharacteristics at baseline, trough-to-peak ratios,adverse events and laboratory data were compareddescriptively between the two treatment groups. Laboratory data were evaluated according to prede-fined limits of change and mean change from base-line.
Of the 611 patients, 307 patients were randomisedto candesartan cilexetil and 304 patients to losartan. A total of 535 patients (88%) completed the study:
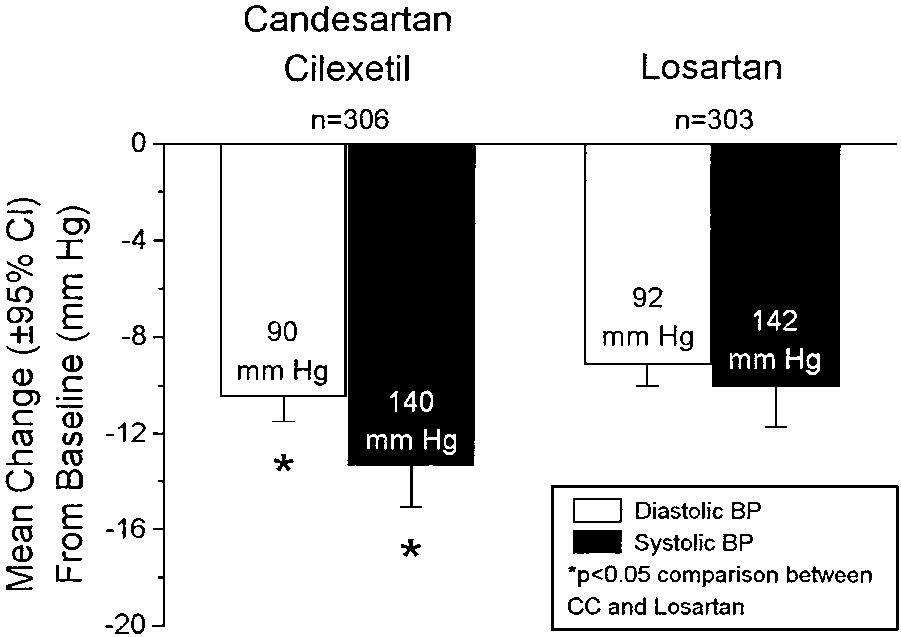
Figure 1 Effects of candesartan cilexetil and losartan on trough
87% for candesartan cilexetil and 88% for losartan.
blood pressure (BP). Labels within bars are means of intent-to-
The study population was 58.6% male, 19.8% black
treat, last value carried forward, readings of the trough sitting BP
with a mean age of 55 years and a baseline BP of
readings (24 ± 3 h after dosing) at week 8. CI, confidence intervals;
152.9/100.3 mm Hg. Patient characteristics at base-
line were similar in the two treatment groups(Table 1).
Table 2 lists the comparison between the candes-
significant. Figure 1 shows the mean trough BP at
artan cilexetil and losartan treatment groups in low-
week 8 in each group with candesartan cilexetil low-
ering the trough, peak and 48-h post last dose dias-
ering trough SBP/DBP by 13.4/10.5 mm Hg com-
pared to 10.1/9.1 mm Hg by losartan (P Ͻ 0.05). Candesartan cilexetil vs losartan
common adverse events for the candesartan cilexetilgroup were headache (7.2%), respiratory infection(3.9%), and sinusitis (3.9%), whereas those for thelosartan group were respiratory infection (7.9%),headache (5.9%), and rhinitis (3.6%). A total of 15of the 611 (2.5%) patients withdrew from the studydue to an adverse event, including nine (2.9%) inthe candesartan cilexetil group and six (2.0%) in thelosartan group. Only four of the 611 (0.7%) patientsreported adverse events that were considered seri-ous due to hospitalisation during the double-blindtreatment period; two were in the candesartan cilex-etil group and two were in the losartan group. Therewere no deaths during this trial. Minor changes from
Figure 2 Effects of candesartan cilexetil and losartan on peak
baseline in laboratory values were observed in
blood pressure (BP). Labels within bars are means of the peak
isolated individuals. There were no clinically mean-
sitting BP readings (6 ± 2.5 h after dosing) at week 8. CI, confi-
ingful changes in mean laboratory values in either
dence intervals; CC, candesartan cilexetil.
treatment group and no laboratory evidence ofdeterioration in renal, hepatic, or metabolic func-
Figure 2 shows the mean peak BP at week 8 in each
group with candesartan cilexetil reducing peakSBP/DBP by 15.5/12.9 mm Hg compared to 12.0/9.5
Discussion
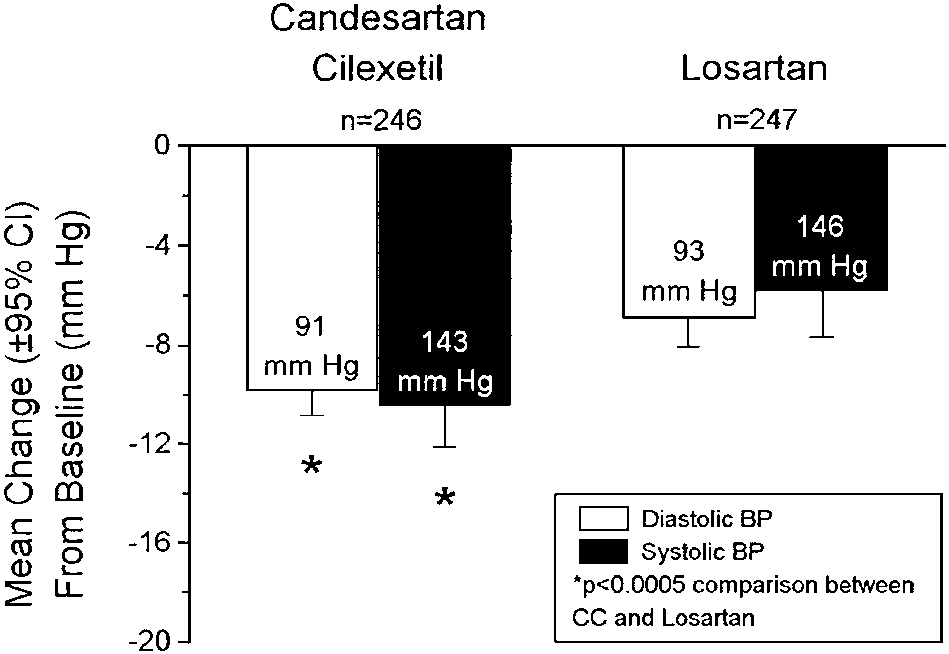
mm Hg by losartan (P Ͻ 0.005). Figure 3 shows themean 48-h BP at week 8 in each group with candes-
The present study was designed to provide an effec-
artan cilexetil lowering the 48-h post last dose
tive comparison of the BP lowering effects of these
SBP/DBP by 10.5/9.9 mm Hg vs 5.9/7.0 mm Hg by
two ARBs. Candesartan is a once-daily drug
losartan (P Ͻ 0.0005). At the week 8 visit, the
although losartan is occasionally used twice daily as
trough-to-peak ratios were 0.86 for candesartan
its package insert states that peak effects are uni-
cilexetil and 0.92 for losartan. Candesartan cilexetil
formly but moderately larger than trough effects.
also produced a numerically higher responder rate
Thus, the study measured not only trough SBP/DBP
(58.8% for candesartan cilexetil and 52.1% for
but also peak and 48 h post dose BP. Although the
losartan) and control rate (49.0 for candesartan
trough-to-peak ratio did not give any details of the
cilexetil and 44.6% for losartan) but the differences
actual BP effects during the 24-h period, a high
did not reach statistical significance.
trough/peak ratio confirms a substantial persistence
Overall, the incidence and intensity of adverse
of the peak BP lowering effects of the drug before
events were similar in the two treatment groups. A
the next dosing. With the value exceeding 80% for
total of 276 of 611 (45.2%) patients reported adverse
each drug, both drugs were effective as once daily
event: 45.6% in the candesartan cilexetil group and
antihypertensive agents. The 48-h post dose BP was
44.7% in the losartan group. Most adverse events
measured to evaluated whether the insurmountable
were mild in intensity and resolved with continued
AT1 receptor binding characteristics of candesartan
treatment including dose escalation. The three most
translated clinically into more sustained BP lower-ing effects. Although only about 80% of patientsshowed up for the 48-h post dose BP measurement,the drop outs were comparable from each group andthe reading was available in a fairly large number ofpatients (a total of 493 patients). The findings of theimpressive extended therapeutic BP lowering effectsof candesartan cilexetil compared to losartan suggestthat the different receptor binding properties of thetwo ARBs resulted in tangible clinical benefits incase of a missed dose. Candesartan had an AT1 bind-ing affinity in rabbit aorta 80 times greater than thatof losartan and 10 times greater than that of EXP3174.10 In summary, the superior blockade of cande-sartan on the AT1 receptor of angiotensin II than los-artan probably accounted for the greater antihyper-tensive efficacy of the drug with the results of thestudy
Figure 3 Effects of candesartan cilexetil and losartan on blood
trough, peak and 48 h post dose BP to a greater
pressure (BP) 48 h after the last dose of study medications. Labelswithin bars are means of the 48 h BP readings at week 8. CI, con-
extent than losartan (P Ͻ 0.05).
fidence intervals; CC, candesartan cilexetil.
The findings of this study are similar to those of
Candesartan cilexetil vs losartan DG Vidt et al
CLAIM Study I, the other identically-designed, com-
the meta-analysis. Thus, the conclusions of this
parative study of candesartan cilexetil (n = 332) and
meta-analysis are probably applicable to the earlier
losartan (n = 322).6 CLAIM Study I showed that at
ARBs but not to candesartan cilexetil.
week 8, candesartan cilexetil 32 mg once daily wasmore effective in lowering all the measured BP para-
Conclusion
meters than losartan 100 mg once daily (P Ͻ 0.05):candesartan
This randomised, controlled, forced titration study
13.3/10.9 mm Hg, peak BP by 15.2/11.6 mm Hg and
demonstrated consistently that candesartan cilexetil
48-h post dose BP by 11.2/10.2 mm Hg compared to
32 mg once daily, lowered trough, peak and 48 h
a reduction of trough BP by 9.8/8.7 mm Hg, peak BP
post dose BP more effectively than losartan 100 mg
by 12.6/10.1 mm Hg, and 48-h post dose BP by
once daily in a diverse population with systemic
5.3/6.0 mm Hg by losartan. In addition, CLAIM
hypertension in the US. Both drugs were well toler-
Study I showed that candesartan cilexetil produced
higher responder and control rates (62% and 56%)than losartan (54% and 47%); the differences beingstatistically
Acknowledgements
independent studies showing the greater efficacy of
We gratefully acknowledge the diligent efforts of the
clinical study coordinators at the 72 investigative
occurring by chance is minimal as the one-sided P-
sites. We also recognise the contributions of Chan-
neary McDowell, BS, Jeanine Parsons, BS, Melissa
0.025 × 0.025 = 0.000625, and the corresponding
Grozinski, BS, Anne Kezer, BS, Conrad Tou, PhD,
two-sided P value is 0.00125.11 Overall, including
Terry Flanagan MPH, James Gaddy, PhD, Oliver
the present study, there have been five sizable, dou-
Yeh, BA and Debbie Brangman, MBA, for invaluable
ble-blind, randomised, controlled studies providing
assistance in the conduct of the study and manu-
direct comparison between candesartan cilexetil
and losartan.3–6 The Andersson and Neldam study3showed that candesartan cilexetil 16 mg once dailylowered SBP/DBP more effectively than losartan
References
50 mg once daily by 4.6/3.7 mm Hg with the differ-
1 Morsing P et al. Mechanistic differences of various
ence in DBP statistically significant. In the CANDLE
AT1-receptor blockers in isolated vessels of different
(Candesartan Versus Losartan Efficacy Comparison
origin. Hypertension 1999; 33: 1406–1413.
Study), candesartan cilexetil 16 mg dose-titrated if
2 Vanderheyden PML, Fierens FLP, De Backer JP, Vau-
needed to 32 mg once daily reduced SBP/DBP more
quelin G. Reversible and syntopic interaction between
than losartan 50 mg dose titrated if needed to
angiotensin receptor antagonists on Chinese hasmster
100 mg once daily by 1.9/2.1 mm Hg, with the differ-
ovary cells expressing human angiotensin II type I
ence in DBP statistically significant.4 In a forced
receptors. Biochem Pharmacol 2000; 59: 927–935.
3 Andersson OK, Neldam S. The antihypertensive effect
titration study, candesartan cilexetil 16 mg once
and tolerability of candesartan cilexetil, a new gener-
daily lowered 24-h ambulatory SBP/DBP more than
ation angiotensin II antagonist, in comparison with
losartan 100 mg by 4.1/1.8 mm Hg, with the differ-
losartan. Blood Pressure 1998; 7: 53–59.
ence in SBP statistically significant.5 These three
4 Gradman AH et al, for the Candesartan Versus Losar-
studies, however, did not test the recommended
tan Efficacy Comparison (CANDLE) Study Group.
once daily maximum doses of the two drugs by a
Comparative effects of candesartan cilexetil and losar-
forced titration design. Thus, with the strikingly
tan in patients with systemic hypertension. Heart Dis-
consistent demonstration of greater peak, trough and
ease 1999; 1: 52–57.
48-h post dose BP lowering of candesartan cilexetil,
5 Lacourciere Y, Asmar R, for the Candesartan/Losartan
these two CLAIM studies establish convincingly the
study investigators. A comparison of the efficacy andduration of action of candesartan cilexetil and losartan
greater antihypertensive efficacy of candesartan
as assessed by clinic and ambulatory blood pressure
cilexetil over losartan when compared at once daily
after a missed dose, in truly hypertensive patients: a
placebo-controlled, forced titration study. Am J Hyper-
These head-to-head comparisons are important to
tens 1999; 12: 1181–1187.
differentiate the antihypertensive efficacy of ARBs.
6 Bakris G et al. Antihypertensive efficacy of candesar-
A recent meta-analysis of 43 published, randomised,
tan in comparison to losartan: The CLAIM study. J Clin
controlled trials concluded comparable antihyper-
Hypertens, 2001; 3: 16–21.
tensive efficacy of losartan, valsartan, irbesartan and
7 Physician’s Desk Reference. 54th edn. Medical Eco-
candesartan cilexetil and a near flat dose response
nomics: Montvale (NJ), 2000. (a) Atacand (candesartan
of these ARBs.12 The meta-analysis consists essen-
cilexetil), pp 592–594; (b) Cozzar (losartan), pp 1769–1772.
tially of data on the two earlier ARBs, losartan and
8 Munafo A et al. Drug concentration response relation-
valsartan (81% of the ARB monotherapy starting
ships in normal volunteers after oral administration of
losartan, an angiotensin II receptor antagonist. Clin
titration data). It is also noteworthy that only 8–
Pharmacol Ther 1992; 51: 513–515.
16 mg candesartan cilexetil doses were evaluated in
9 Delacretaz E, Nussberger J, Biollaz J, Weber B, Brunner
Candesartan cilexetil vs losartan
HR. Characterization of the angiotensin II receptor
Research Inc, Tuscon, AZ; Theodore E. Lefton, MD,
antagonist TCV-116 in healthy volunteers. Hyperten-
ICSL-Clinical Studies, Melbourne, FL; Alan Levin,
sion 1995; 25: 14 –21.
MD, Glenville, NY; Hari Malik, MD, Cedarwood
10 Burnier M, Brunner HR. Angiotensin II receptor antag-
Medical Center, St. Joseph, MI; Abe Marcadis, MD,
onists. Lancet 2000; 355: 637–645.
ICSL-Clinical Studies, Boynton Beach, FL; R Eric
11 Fisher LD, Moye LA. Carvedilol and the Food and
Drug Administration approval process: an introduc-
McAllister, MD, MEDStudies Inc, Ukiah, CA; James
tion. Controlled Clin Trials 1999; 20: 1–15.
McMechan, DO, Jefferson Country Medical Clinic
12 Conlin PR et al. Angiotensin II antagonists for hyper-
PA, Oskaloosa, KS; John Mihalik, MD, Northern Cal-
tension: are there differences in efficacy? Am J Hyper-
ifornia Medical Associates, Cloverdale, CA; David
tens 2000; 13: 418– 426.
Miller, MD, Bucks County Clinical Research,Moorisville, PA; Michael Miller, MD, University of
Appendix
MD School of Medicine, Baltimore, MD; RafaelMontoro, MD, Clinical Therapeutics Corp, Coral
CLAIM Study 230 Investigators:
Gables, FL; Jane Mossberg, MD, Research Studies,
Frank G Baratta, MD, Ft Lauderdale, FL; Scott
Blesser, DO, Midwest Regional Research Inc., Bell-
Research of Northern Virginia, Falls Church, VA;
brook, OH; Paul J Bresnan, MD, Watson Clinic LLP,
Lakeland, FL; Joan Brigham, MD, ICSL-Clinical
Research, Greer, SC; Larry Neuman, MD, New York,
Studies, Charlotte, NC; David Calhoun, MD, Univer-
NY; Margarita C Nunez, MD, ICSL-Clinical Studies,
sity of Alabama at Birmingham, Birmingham, AL;
St. Petersburg, FL; Thomas O’Barr, MD, Health
Julian A Colton, MD, Health Advance Institute, St.
Advance Institute, Marietta, GA; Mark Okusa, MD,
Petersburg, FL; Martin Conway, MD, Lovelace
University of Virginia Medical Center, Charlottes-
Scientific Research, Albuquerque, NM; Pamela
ville, VA; Vasilios Papademetriou, MD, VAMC-
Craven, MD, Health Advance Institute, Oklahoma
Hypertension Research Clinic, Washington, DC;
City, OK; William Cushman, MD, VAMC-Memphis,
Kavita Persaud, MD, St. Joseph Senior Health Ser-
Memphis, TN; Stephen D’Amico, MD, GRAE, Inc,
vices, Fort Wayne, PA; Frank Pettyjohn, MD, Uni-
Franklin, TN; Vincent DeQuattro, MD, Los Angeles,
versity of South Alabama, Mobile, AL; James L Pool,
CA; Lance D Dworkin, MD, Rhode Island Hospital,
MD, Baylor College of Medicine Methodist Hospital,
Providence, RI; David J. Frid, MD, OSU Center for
Houston, TX; Anthony Puopolo, MD, Milford
Wellness and Prevention, Columbus, OH; Debra
Emergency Associates, Inc, Milford, MA; Promod
Ann Friesen, MD, Exempla Internal Medicine,
Raval, MD, Oak Park, MI; Albert J Razzetti, MD, Uni-
Wheat Ridge, CO; W Thomas Garland, MD, Lawr-
versity Clinical Research-DeLand, DeLand, FL;
ence Clinical Research, Lawrenceville, NJ; Larry I
Steven Rosansky, MD, Three Rivers Medical-Carol-
Gilderman, DO, University Clinical Research Inc,
ina Research Assoc, Columbia, SC; Herman Rose,
Pembroke Pines, FL; Edward Gillie, MD, Medical
MD, Fort Worth, TX; Eli Roth, MD, Sterling Research
Studies, Florida, Fort Myers, FL; Ivan Goldsmith,
Group Ltd, Cincinnati, OH; Henry Rothschild, MD,
MD, West Trop Medical Centre, Las Vegas, NV; Ron-
Louisiana State University Medical Center, New
ald C Gove, MD, Jersey Research Foundation Inc,
Orleans, LA; John Rubino, MD, Raleigh Medical
Linwood, NJ; Maria Gutierrez, MD, ICSL-Clinical
Group, Raleigh, NC; Susan Savage, MD, ICSL-Clini-
Studies, Fort Lauderdale, FL; Kathy Harvey, DO,
cal Studies, Denver, CO; Kevin T Scully, MD, Lex-
Internal Medicine, Logan, WV; Bradley Heppner,
ington Cardiology Consultants, Lexington, KY; Stan
MD, ICSL-Clinical Studies, Pittsburgh, PA; John A
Slabic, MD, Slabic & Slabic Internal Medicine, Erie,
Holmes, MD, Heart of America Research Institute,
PA; William B Smith, MD, New Orleans Center for
Mission, KS; E Walter Hood, DO, ICSL-Clinical
Clinical Research, New Orleans, LA; John A Stou-
Studies, Atlanta, GA; David B Jack, MD, Physicians
kides, MD, ICSL-Clinical Studies, East Providence,
Research Options, Sandy, UT; Edwin Jacobson, MD,
RI; Malcolm Taylor, MD, Jackson Cardiology Associ-
Los Angeles, CA; Ashok Jain, MD, Dearborn, MI; Roy
ates, PA, Jackson, MS; Thomas Tse, MD, Bellville,
Kaplan, MD, East Bay Clinical Trial, Concord, CA;
IL; Margaret Wagner, MD, Idaho Falls, IN; Mervyn
Edward M Kerwin, MD, Clinical Research Institute
Weerasinghe, MD, Rochester Clinical Research,
of Southern Oregon, LLC, Medford, OR; Robert
Rochester, NY; Susan Wehle, MD, ICSL-Clinical
Kloner, MD, Los Angeles Cardiology Assoc, Los
Studies, Brandon, FL; Gerald D Wolfley, MD, Hill
Angeles, CA; Robert Leff, MD, Hill Top Argus
Chiesadomestica.net Pillola abortiva per mascherare l'orrore dell'aborto 18 novembre 2007 "Meglio l’ospedale di quell’inferno” Ombre e dolore sulla kill pill (e gli effetti collaterali si moltiplicano) - di Assuntina Morresi, Eugenia Roccella Roma. La RU486, la pillola abortiva, sembra avere un merito: aver convertito alcuni medici obiettori. Su Repubblica di ieri, il dottor Salvatore
(E-News Letter) Drug Information & Pharmacovigilance Centre, Tamil Nadu Pharmacy Council, Tele fax: 91 - 044 - 2473 0061, e -mail: Web site: http://tnpc.ac.in Contact: 91 44 -24338421 Antidepressants as Treatment Immediately after Stroke? IN SIGHT Research suggests a new strategy for the treatment of stroke. Research in rodents • Antidepressants as Treatment
 Candesartan cilexetil vs losartan
Candesartan cilexetil vs losartan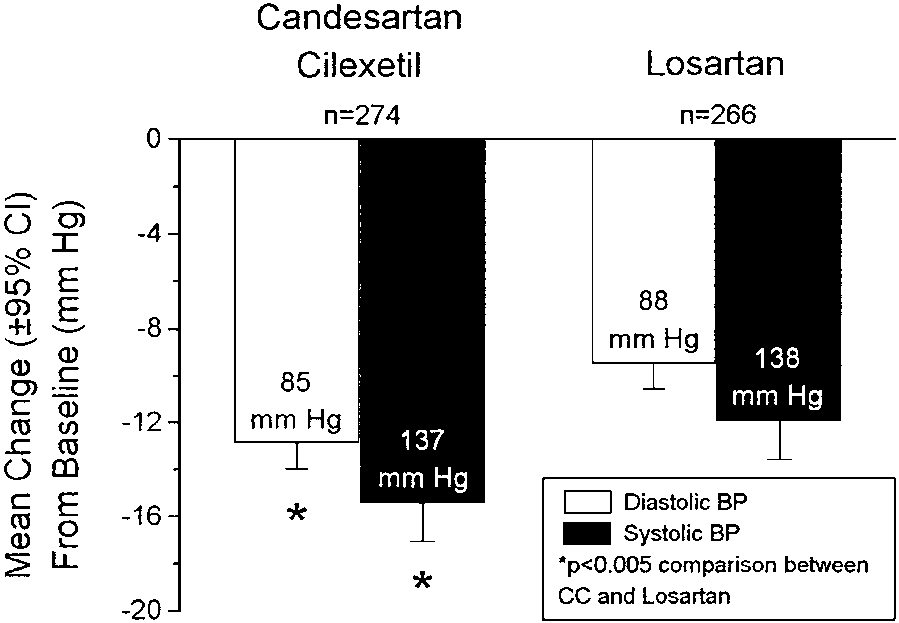
 Candesartan cilexetil vs losartan
Candesartan cilexetil vs losartan