Int J Colorectal DisDOI 10.1007/s00384-010-1066-7
Porcine dermal collagen matrix injection may enhance flaprepair surgery for complex anal fistula
Pierpaolo Sileri & Luana Franceschilli &Giovanna Del Vecchio Blanco & Vito M. Stolfi &Giulio P. Angelucci & Achille L. Gaspari
Accepted: 4 October 2010# Springer-Verlag 2010
impact on incontinence [, ]. On the other hand, surgical
Introduction The use of biomaterials to treat anal fistula has
treatments for high and complex fistulas may results in
drawn great interest. More recently, a porcine dermal matrix
variable degree of anal sphincter apparatus impairment.
injection has been proposed as infill biomaterial to treat
Various alternative surgical options have been proposed
such as flap repair, fibrin glue injection, seton drainage and
Methods We propose a novel approach consisting in non-
fistula track plug insertion with variable success rates
cutting seton positioning followed by flap repair associated
Currently, the transanal rectal advancement flap represents
with dermal matrix injection into the fistula tracts after
the most effective treatment for complex anal fistulas
allowing the closure of the internal opening with successful
Results We report our experience with this two-staged
rates, in some series, above 90%. However commonly,
procedure on 11 consecutive patients with recurrent high
recurrence rate is approximately 30%, a rate that leaves
trans-sphincteric fistulas with a minimum follow-up of
Over the last two decades, the use of biomaterials to treat
Conclusions In our experience, this two-stage approach
anal fistula has drawn great interest. Among these, fibrin
glue injection has been proposed to obliterate the fistulatract/s, but initial enthusiasms have been tempered by high
Keywords Permacol . Complex anal fistula . Flap repair
rates of recurrences [–, , ]. Several authors havetried a combination of fibrin glue and flap repair in order toenhance its success rates [, . Results have been
disappointing, showing worse outcomes after the combina-tion of the two compared to flap repair alone []. Reasons
The management of fistula-in-ano aims minimizing recur-
why fibrin glue addition is ineffective or even worse are
rences while maintaining continence. Low fistulas, where
unclear. A possible explanation can be that the closure of
the tract is submucosal, intersphincteric, or located in the
the fistula tract with the glue leads to a situation where
lower third of the external anal sphincter are usually treated
insufficient drainage from the primary and eventual
by fistulotomy with low recurrence rates and relatively little
secondary fistula tract occurs More recently, a porcinedermal matrix injection, named Permacol injection (Covi-dien plc, Dublin, Ireland) has been proposed as infillbiomaterial to treat fistulas [but data on its use on
P. Sileri (*) : L. Franceschilli : G. Del Vecchio Blanco :
anal fistula treatment is scant. We propose a novel approach
V. M. Stolfi : G. P. Angelucci : A. L. GaspariDepartment of Surgery (Dir. Achille L. Gaspari),
consisting in non-cutting seton positioning followed by flap
University of Rome Tor Vergata, Policlinico Tor Vergata,
repair associated with Permacol injection into the fistula
tracts after. We also report our experience with this two-
staged procedure on 11 consecutive patients with recurrent
00133 Rome, Italye-mail: [email protected]
Between July 2009 and April 2010, 11 consecutive patientsunderwent mucosal advancement flap repair and Permacolinjection for complex anal fistula in our institution. Inclusion criteria for this study were age between 18 and75 years and the presence of a complex anal fistula, definedas Crohn's, rectovaginal, and high trans-sphincteric fistulas. Patients' characteristics are resumed in Table
All patients underwent outpatient clinic evaluation and
preoperative MRI and/or endoscopic ultrasound. Fecalincontinence before and after surgery was evaluated usingthe Fecal Incontinence Severe Index (FISI) score. Patientswith a score >6 underwent anal manometry before surgery. All procedures consisted in two-stage approach.
Surgical technique, stage I On the day of the surgery, anenema was administered to the patient. All patientsunderwent surgery under general anesthesia in lithotomyposition and broad-spectrum antibiotics given at induction. The internal orifice was found using oxygen peroxideinjection through the external opening and gently probed. At this point a non-cutting seton (Silicone Surgical Vessel
Fig. 1 Flap preparation (mucosa, submucosa, and a small amount of
Loop, Dev-o-Loop, Mini-red, Covidien) was placed for a
internal sphincter fibers) after >6 weeks drainage seton insertion
period of at least 8 weeks aiming adequate drainage of the
which aimed draining the fistula tract thus abolishing collateral tractswhile transforming it in a more straight one
sepsis and followed up routinely as outpatient.
Surgical technique, stage II Surgery was performed in a
The flap base was performed large enough to avoid its
day surgery setting, under general anesthesia in the
ischemia and mobilization to avoid tension. The fistula tract
lithotomy position. Initial step was the identification and
was probed, curetted, and irrigated with saline. The internal
creation of an elliptical excision below the internal opening
opening underneath the mobilized flap was not closed
encompassing 20–30% of the circumference of the anus.
before suturing. The flap was sutured distally using full-
The rectal flap, fashioned with mucosa, submucosa, and a
thickness-interrupted vicryl 2-0 sutures (Fig. At this
small amount of internal sphincter fibers, was adequately
point, liquid dermal porcine matrix (Permacol Injection,
mobilized to overlap and cover the internal opening.
Covidien plc, Dublin, Ireland) was gently injected in the
Particular care on hemostasis was given to prevent
retrograde manner through the external orifice to fill the
entire tract. The entire procedure was performed under
Fig. 2 a and b The flap (mucosa,submucosa and a small amount ofmuscular fibers) was sutured usinginterrupted 00 absorbable sutures. Subsequently the fistula tract wasfilled with the preparation underdirect visual control. The externalorifice was then closed with a 00silk suture to prevent earlyextrusion. The infill preparationwas also injected all around thefistula tract nearby the externalorifice
direct vision of the flap in order to prevent anterograde
fluconazole (per os 200 mg/day). Mean follow-up after
extrusion and flap tension (Fig. In order to prevent
surgery was 9 months and we observed a single failure after
early extrusion of the matrix injection, at this point,
6 weeks secondary to partial displacement. This failure was
additional injection was performed next to the fistula tract
observed in a Crohn's disease patient who experienced a
at 360° through a 20-gauge needle and the external orifice
severe recurrence of intraluminal disease with frequent
was closed using a purse-string or figure of eight suture
bowel motions (>10/day). No difference in terms of
with silk 00. This suture was then removed at the first
preoperative and postoperative FISI scores was observed in
all but one patient who experienced transitory gas incontinence
After the discharge, patients were followed-up 1, 2,
4 weeks after surgery and then routinely every 4 months. Data was collected prospectively including demographics,previous treatments, details of surgery, and follow-up results.
Nowadays, flap repair remains the “gold standard” approachfor the treatment of high trans-sphincteric perianal or complex
fistulas. The flap repair, closing the internal anorectal opening,eliminates the source of persisting anal fistula where fecal
Overall, 11 patients who had complex anal fistula of
material is forced through. Healing rates are reported to range
cryptoglandular origin (five patients) and inflammatory
between 37% and 98% , , Lower recurrence rates
bowel disease (IBD) related (six patients) were treated.
have been observed after non-cutting seton insertion prior
Results are summarized in Table . The median age was
Over the last two decades the use of biomaterials to treat
One patient had previous rectovaginal fistula surgery
anal fistula has drawn great interest. Advantages of this
which failed and required fecal diversion. All first-stage
approach include simple and repeatable applications,
procedures were performed as planned day surgery cases.
preservation of sphincter integrity, minimal patient's dis-
Eight out of 11 second-stage procedures were carried in a day
comfort, and the ability for subsequent surgical options if
surgery setting, while three required overnight admission
needed. Among these, fibrin glue injection has been
because of age (one patient) and postoperative pain (two
proposed to obliterate the fistula tract/s, but initial enthu-
patients). No postoperative complications were observed as
siasms have been tempered by disappointing high rates of
part of a fungi infection substained by Candida albicans,
recurrences [–, Failures are attributable to the
which was successfully treated with a 7-days cycle of
displacement of the glue from the fistula tracts early after
surgery secondary to increased pressure from coughing or
that this combined approach offers several potential
straining [Other reasons suggested for the persistence
advantages compared to fibrin glue injection alone or
of fistula tracts have included chronic infection, residual
after flap repair. The earlier non-cutting seton insertion
granulation tissue or islands of epithelium being left behind
allows a good drainage of the sepsis, fistula cavities, and,
in the tract. As a matter of fact most of the authors point out
when present, the obliteration of all (either known or
the need of the tract curettage before sealant injection ].
unrecognized) secondary fistula tracts. At the second-stage
Several authors have tried a combination of fibrin glue
surgery, the injection would cover a single, possibly
and flap repair in order to enhance its success rates [,
. Results have been disappointing, showing worse
The flap repair (mucosal, submucosal, and some muscle
outcomes after the combination of the two compared to
fibers), covering the internal source of the fistula, would
flap repair alone ]. Reasons why fibrin glue addition is
prevent extrusion of the Permacol injection as already
ineffective or even worse are unclear. A possible explana-
shown by several studies using fibrin glue. In our opinion,
tion can be that the closure of the fistula tract with the glue
the reported failures using the combination of the two
leads to a situation where insufficient drainage from the
techniques can be explained with the need of correct fistula
primary and eventual secondary fistula tract occurs [].
anatomy identification and previous drainage of the sepsis
Furthermore, other authors have mentioned incomplete
obtained with the use of loose seton drainage as bridge to
filling of the fistula tract because of cavitary fistula tracts
flap repair surgery. The injected matrix offers a scaffold for
or the presence of side branches. Lindsey et al. reported the
scar formation and tissue regeneration. However some
efficacy of endorectal ultrasound to identify fistula anato-
limits are still evident. At the present time, this injectable
my, thus, the use of this approach preoperatively to improve
preparation is too liquid and this may lead to an immediate
results [A two-staged technique, using non-cutting
extrusion after injection. Despite that it has been success-
seton followed by a period of healing before glue injection
fully used for this purpose in outpatient setting as single
injection through the external orifice and around it [our
Recently, a porcine dermal matrix injection (Permacol
experience with its use in outpatient setting for anal fistula
Injection-Covidien plc, Dublin, Ireland) has been used as
(after previous seton placement) or sinus resulted unfavor-
infill biomaterial to treat fistulas []. Permacol is a
able and all patients (5 patients, data not published)
commercially available porcine dermal collagen developed
eventually required surgery. The sudden extrusion of the
as sheet or liquid injection. It is non-allergenic, non-
infill material might be responsible for this result. The early
antigenic, and entirely biocompatible. It has been used
extrusion is also observed after flap advancement surgery,
successfully in many different ways, including abdominal
thus in order to prevent extrusion we perform a purse-string
wall hernia repairs including incisional and parastomal
suture around the external orifice to avoid leaks during the
hernia as well as for pelvic floor surgery [. The
first three postoperative days and thereafter we remove the
injectable form is a 50% per by volume collagen particles
suture to prevent potential suppurations.
in saline and presently the most evident limit to fill in a
In conclusion, Permacol injection with advancement flap
fistula track is its extremely liquid consistency. It has been
repair seems to be safe and effective. A previous seton
used in cases of anal and urinary incontinence and for
insertion is mandatory to “clean” the fistula cavities and tracts
plastic surgery. At the present time, literature data experi-
and to “ameliorate” fistula anatomy. The current preparation
ence on its use to treat anal fistulas is scant. Himpson et al.,
does not allow the use as infill material in outpatient care even
in a experimental porcine model of fistula-in-ano, concluded
if fistula tract has been previously drained with seton.
that when the fistula track is completely removed and
Obviously a longer follow-up and large series are needed to
durable infill material used, it is possible to treat fistulas
successfully even in presence of infection or contamina-tion []. The same authors suggested that it is likely that
Acknowledgment Mrs. Brega Fiorella for the preparation of the
because of the cross-linked nature of Permacol, it provides
tissue repair regeneration with stability and facilitatescontrolled and ordered wound healing. However in theirexperience, the “too liquid” injectable preparation was
modified by centrifugation to produce a thicker paste toprevent extrusion from the tract. Initial clinical use is even
1. Davies M, Harris D, Lohana P, Chandra Sekaran TV, Morgan
less documented. In this study, we report our experience
AR, Beynon J, Carr ND (2008) The surgical management of
with a novel approach consisting in non-cutting seton
fistula-in-ano in a specialist colorectal unit. Int J Colorectal Dis23(9):833–838
positioning followed by flap repair associated with
2. Garcia-Aguilar J, Belmonte C, Wong WD, Goldberg SM,
Permacol injection into the fistula tracts after. We believe
Madoff RD (1996) Anal fistula surgery. Factors associated
with recurrence and incontinence. Dis Colon Rectum 39
11. Sentovich SM (2003) Fibrin glue for anal fistulas: long-term
results. Dis Colon Rectum 46(4):498–502
3. Quah HM, Tang CL, Eu KW, Chan SY, Samuel M (2006) Meta-
12. Zmora O, Mizrahi N, Rotholtz N, Pikarsky AJ, Weiss EG,
analysis of randomized clinical trials comparing drainage alone vs
Nogueras JJ, Wexner SD (2003) Fibrin glue sealing in the
primary sphincter-cutting procedures for anorectal abscess-fistula. Int
treatment of perineal fistulas. Dis Colon Rectum 46(5):584–589
J Colorectal Dis 21(6):602–609, Epub 2005 Nov 30. Review
13. Himpson RC, Cohen CR, Sibbons P, Phillips RK (2009) An
4. Taxonera C, Schwartz DA, García-Olmo D (2009) Emerging
experimentally successful new sphincter-conserving treatment for
treatments for complex perianal fistula in Crohn's disease. World J
anal fistula. Dis Colon Rectum 52(4):602–608
14. Milito G, Cadeddu F (2009) Conservative treatment for anal
5. Ellis CN, Clark S (2006) Fibrin glue as an adjunct to flap repair of
fistula: collagen matrix injection. J Am Coll Surg 209(4):542–543,
anal fistulas: a randomized, controlled study. Dis Colon Rectum
15. Ortiz H, Marzo M, de Miguel M, Ciga MA, Oteiza F, Armendariz
6. Singer M, Cintron J, Nelson R, Orsay C, Bastawrous A, Pearl R,
P (2008) Length of follow-up after fistulotomy and fistulectomy
Sone J, Abcarian H (2005) Treatment of fistulas-in-ano with fibrin
associated with endorectal advancement flap repair for fistula in
sealant in combination with intra-adhesive antibiotics and/or
surgical closure of the internal fistula opening. Dis Colon Rectum
16. Chung W, Kazemi P, Ko D, Sun C, Brown CJ, Raval M, Phang T
(2009) Anal fistula plug and fibrin glue versus conventional
7. van Koperen PJ, Wind J, Bemelman WA, Slors JF (2008) Fibrin
treatment in repair of complex anal fistulas. Am J Surg 197
glue and transanal rectal advancement flap for high transsphincteric
perianal fistulas; is there any advantage? Int J Colorectal Dis 23
17. Williams JG, MacLeod CA, Rothenberger DA, Goldberg SM
(1991) Seton treatment of high anal fistulae. Br J Surg 78
8. Ellis CN (2007) Bioprosthetic plugs for complex anal fistulas: an
early experience. J Surg Educ 64(1):36–40
18. Hammond TM, Grahn MF, Lunniss PJ (2004) Fibrin glue in the
9. Miller GV, Finan PJ (1998) Flap advancement and core
management of anal fistulae. Colorectal Dis 6(5):308–19, Review
fistulectomy for complex rectal fistula. Br J Surg 85(1):108–
19. Chung W, Ko D, Sun C, Raval MJ, Brown CJ, Phang PT (2010)
Outcomes of anal fistula surgery in patients with inflammatory
10. Buchanan GN, Bartram CI, Phillips RK, Gould SW, Halligan S,
bowel disease. Am J Surg 199(5):609–613
Rockall TA, Sibbons P, Cohen RG (2003) Efficacy of fibrin
20. Lindsey I, Humphreys MM, George BD, Mortensen NJ (2002)
sealant in the management of complex anal fistula: a prospective
The role of anal ultrasound in the management of anal fistulas.
trial. Dis Colon Rectum 46(9):1167–1174
ALBERTO FUJIMORI FUJIMORI-EX PRESIENTE DEL PERÚ REO CULPABLE DE GENOCIDIO, CORRUPCIÓN, DICTADURA. Los cargos por homicidio calificado, asesinato, bajo la circunstancia agravante de alevosía, lesiones graves y secuestro agravado CRONICA DEL JUICIO DEL AÑO EN EL PERU ESPECIAL DEL DIARIO LA PRIMERA La Primera , Lima, 08 de Abril del 2009 La rabia de la derecha César
CURRICULUM VITAE Professor dr. Henk J. Scholten SPINLAB, Center for Research and Education on Spatial Information GENERAL DESCRIPTION OF RELEVANT EXPERIENCE Professor dr. Henk Scholten is professor in Spatial Informatics at the Faculty of Business Economics at the Free University in Amsterdam and Scientific Director of the SPINlab, Center for Research and Education on Spatial Informa
 Int J Colorectal DisDOI 10.1007/s00384-010-1066-7
Porcine dermal collagen matrix injection may enhance flaprepair surgery for complex anal fistula
Pierpaolo Sileri & Luana Franceschilli &Giovanna Del Vecchio Blanco & Vito M. Stolfi &Giulio P. Angelucci & Achille L. Gaspari
Accepted: 4 October 2010# Springer-Verlag 2010
impact on incontinence [, ]. On the other hand, surgical
Introduction The use of biomaterials to treat anal fistula has
treatments for high and complex fistulas may results in
drawn great interest. More recently, a porcine dermal matrix
variable degree of anal sphincter apparatus impairment.
Int J Colorectal DisDOI 10.1007/s00384-010-1066-7
Porcine dermal collagen matrix injection may enhance flaprepair surgery for complex anal fistula
Pierpaolo Sileri & Luana Franceschilli &Giovanna Del Vecchio Blanco & Vito M. Stolfi &Giulio P. Angelucci & Achille L. Gaspari
Accepted: 4 October 2010# Springer-Verlag 2010
impact on incontinence [, ]. On the other hand, surgical
Introduction The use of biomaterials to treat anal fistula has
treatments for high and complex fistulas may results in
drawn great interest. More recently, a porcine dermal matrix
variable degree of anal sphincter apparatus impairment.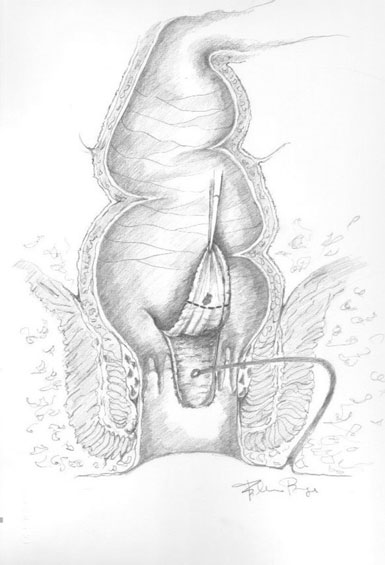 Between July 2009 and April 2010, 11 consecutive patientsunderwent mucosal advancement flap repair and Permacolinjection for complex anal fistula in our institution.
Between July 2009 and April 2010, 11 consecutive patientsunderwent mucosal advancement flap repair and Permacolinjection for complex anal fistula in our institution.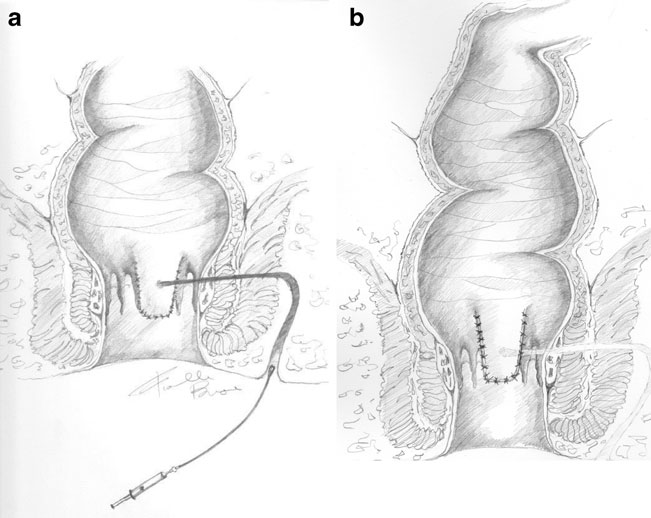 Fig. 2 a and b The flap (mucosa,submucosa and a small amount ofmuscular fibers) was sutured usinginterrupted 00 absorbable sutures.
Fig. 2 a and b The flap (mucosa,submucosa and a small amount ofmuscular fibers) was sutured usinginterrupted 00 absorbable sutures.