He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Effect on pregnancy rates of the delay in the administration of levonorgestrel for emergency contraception: a combined analysis of four who trials
Effect on pregnancy rates of the delay in the administration of
levonorgestrel for emergency contraception: a combined analysis of four
Gilda Piaggioa,⁎, Nathalie Kappb, Helena von Hertzenc
aStatistika Consultoria, São Paulo, Brazil
bWorld Health Organization, 1211 Geneva, Switzerland
cConcept Foundation, 1211 Geneva, Switzerland
Received 29 October 2010; revised 6 November 2010; accepted 16 November 2010
Background: Levonorgestrel is an effective method for emergency contraception (EC) and is used worldwide. Consistent with itsmechanism of action in delaying ovulation, the earlier it is administered within 72 h of an unprotected act of intercourse, the more effective itis. There is uncertainty, however, about its effectiveness after 72 h. This analysis explores the effect of 24-h intervals of delay inlevonorgestrel administration on pregnancy rates when used until 120 h of an unprotected act of intercourse. Study Design: Data were analyzed from 6794 women participating in four World Health Organization randomized trials and receiving1.5 mg of levonorgestrel for EC in a single dose or split into two doses 12 h apart, within 48, 72 or 120 h of an act of unprotected intercourse. The pregnancy rates among women in successive days after an unprotected act of intercourse and odds ratios of pregnancy were calculatedusing logistic regression with the first day as the reference. Results: For the four trials combined, odds ratios for pregnancy in the second, third and fourth day with respect to the first day were notsignificantly different from 1 at the 5% level of significance. On the fifth day, the odds ratio of pregnancy compared to the first day wasalmost 6. Conclusions: Levonorgestrel for EC should be administered as soon as possible after unprotected intercourse. Delaying levonorgestreladministration until the fifth day after unprotected intercourse increases the risk of pregnancy over five times compared with administrationwithin 24 h. It is uncertain whether levonorgestrel administration on the fifth day still offers some protection against unwanted pregnancy. 2011 Elsevier Inc. All rights reserved.
Keywords: Emergency contraception; Levonorgestrel; Effectiveness in successive days; Combined analysis; Meta-analysis
these regimens are administered within 72 h of anunprotected act of intercourse, the more effective they are
Levonorgestrel has been shown to be more effective than
. Although there had been some evidence of decreasing
the Yuzpe regimen for emergency contraception (EC) and to
effectiveness of levonorgestrel (LNG) beyond 72 h , the
have a better side-effect profile . Its effectiveness has been
extent and time pattern of this decrease between 72 and 120 h
assessed when administered within 120 h of an unprotected
remained unclear. Combination of results from two World
act of intercourse It has been shown that the earlier
Health Organization (WHO) trials provided someevidence of effectiveness until the fourth day following anunprotected act of sexual intercourse By combining data
☆ GP had a contract to conduct the analysis and write the manuscript
from four WHO trials , including one recently
funded by the UNDP/UNFPA/WHO/World Bank Special Programme of
published we sought to accrue a larger number of
Research, Development and Research Training in Human Reproduction,
women in each of the successive days after an unprotected
act of intercourse to increase the power for the estimation of
⁎ Corresponding author. 1764 vie de l'Etraz, 01220 Divonne-les-Bains,
the relationship between delay in administration and
0010-7824/$ – see front matter 2011 Elsevier Inc. All rights reserved.
G. Piaggio et al. / Contraception xx (2011) xxx–xxx
logistic regression model. This technique was also used toadjust for baseline variables for the two oldest trials
The present article combines data from 6794 women
since the day of delay was not randomized and might be
participating in four WHO randomized trials and receiving
1.5 mg of LNG for EC in a single dose or split into two doses12 h apart, within 48 h 72 h or 120 h of an act ofunprotected intercourse. All four studies were randomized
controlled trials, randomization being applied to different ECregimens. The description of studies is shown in .
The number of women recruited and allocated to a LNG
The proportions of women becoming pregnant (from now
arm in the four trials was 7219. The number in the efficacy
on denoted as pregnancy rates) among those recruited and
populations in LNG arms in the four trials was 6921, and the
receiving LNG in successive days after an unprotected act of
number of women with data on time interval between
intercourse were calculated for each trial and for all the trials
intercourse and treatment and analyzed for delay was 6794
combined. When there were two LNG regimens included in
(see for these data by trial). There was a significant
the trial , the two regimens were combined based on
effect of delay on the proportion of women who became
their similarity regarding efficacy and safety outcomes. The
pregnant (pb.0001). The pregnancy rate varied between
odds ratios (OR) of pregnancy for each of the successive
0.7% (14/2065) and 1.6% (17/1059) during the first 4 days
days of delay after an unprotected act of intercourse, for the
(96 h) after unprotected intercourse and increased to 5.2%
four trials combined, were calculated using logistic regres-
(12/230) on the fifth day (). The ORs for pregnancy
sion and the first day as reference. This analysis was repeated
on the second, third and fourth day with respect to the first
using RevMan with a fixed model and the inverse
day were not significantly different from 1 at the 5% level.
variance method, but results are not presented since they
They were, respectively, 0.68 (95% CI 0.36 to 1.28), 1.74
were very similar to the ones obtained using logistic
(95% CI 0.94 to 3.19) and 0.87 (95% CI 0.26 to 2.89). On the
regression. The I2 statistic was calculated to assess
fifth day (96–120 h), the OR of pregnancy compared to the
heterogeneity, and the homogeneity of the effect of delay
first day was almost 6 (OR=5.81, 95% CI 2.87 to 11.76)
across trials was tested by the interaction delay by trial in a
) and the percentage of women who became pregnant
Table 1Characteristics of WHO EC trials using LNG
Randomized controlled trial of LNG vs.
Low-dose mifepristone and two regimens 1. 10 mg single-dose mifepristone
2695 in the LNG regimens analyzedfor delay (97.8%)
Two-dose LNG: 1512Total LNG: 30222794 in the LNG regimen analyzedfor delay (92.5%)
Design: Prospective multicenter randomized controlled trials (random assignment of interventions to subjects within centers). Participants: Healthy women with regular menses, not using hormonal contraception, requesting EC within 48, 72 or 120 h (depending on the trial) of anunprotected act of intercourse. Main outcome: Pregnancy.
G. Piaggio et al. / Contraception xx (2011) xxx–xxx
Table 2Number of pregnancies, number of women and pregnancy rates (%) by 24-h intervals of delay between an unprotected act of intercourse and administration ofLNG, and ORs of pregnancy for intervals after 24 h with respect to the first 24 h, with 95% CIs, for four WHO studies and for the combined data
was 5.2 (95% CI 2.7% to 8.9%), below the 6% to 8%
There was some indication of a different pattern in the
expected without treatment but not significantly different
effect of delay in two of the trials where the
pregnancy rates showed an increasing trend within 72 h.
Combining data from the two trials that included women
However, the heterogeneity of the effect of delay across
until 120 h of delay in administration after an unprotected act
trials was not significant at 5% (p=.0637), I2=47.6%,
of intercourse did not change the results substantially.
The ORs were, respectively, 0.41 (95% CI 0.18 to 0.95),1.25 (95% CI 0.63 to 2.49), 0.72 (95% CI 0.22 to 2.39) and4.83 (95% CI 2.39 to 9.73) for pregnancy in the second,
third, fourth and fifth day with respect to the first day.
The number of women requesting EC after 72 h of an act
of unprotected intercourse is usually small. By combininglarge trials using very similar protocols, the analysispresented in this article intended to accrue a sufficientnumber of women with this characteristic to reliably assessthe effectiveness of levonorgestrel for EC in successive dayswithin 120 h after an act of unprotected intercourse. Among6794 women analyzed, 616 (9.1%) had treatment between72 and 120 h after intercourse.
The results of the combined analysis show no evidence of
an increase in pregnancy rates with the delay in administra-tion of 1.5 mg of LNG, administered in a single dose or splitinto two doses 12 h apart, until the fourth day inclusive afteran act of unprotected intercourse. Levonorgestrel is providedwithout prescription in many countries and is not associatedwith a delay in menses, unlike antiprogestins such asmifepristone The mechanism of action of LNG has beenstudied and the drug is reported to have no effect onimplantation, while mifepristone can prevent it . In
Fig. 1. Odds ratios of pregnancy for intervals of delay between an
cultures where conservative religious views prevail and can
unprotected act of intercourse and administration of levonorgestrel after24 h with respect to the first 24 h, with 95% CIs, for combined data of
influence health policies and public opinion, LNG is more
accessible and acceptable to women than mifepristone or
G. Piaggio et al. / Contraception xx (2011) xxx–xxx
other progestogen-receptor modulators. Similar levels of
the trials included in this report showed a linear
effectiveness of LNG through the fourth day (up to 96 h) are
increasing trend of pregnancy rates within 48 h or within
72 h . Given that the test for homogeneity might be
However, an important increase in pregnancy rates, with a
underpowered, we do not exclude the possibility of a decrease
possible decrease in effectiveness of LNG, is apparent if
in effectiveness in the second, third and fourth day with
administered after the fourth day of an act of unprotected
respect to the first day in certain settings or under particular
intercourse. It is uncertain whether it still provides some
conditions, possibly present in the settings of those two trials,
degree of protection against unintended pregnancy if
and that we could not identify. A decrease in effectiveness of
administered on the fifth day, albeit diminished from earlier
LNG with delay in administration would be consistent with its
administration. We hope this report will have addressed the
mechanism of action of preventing ovulation.
concerns raised about the lack of data on the effectiveness of
A third limitation is that the number of women receiving
LNG when administered between 72 and 120 h of an
treatment between 72 and 120 h of an unprotected act of
intercourse is only 616, from just two trials Although
The Cochrane review about interventions for EC
this number gave enough power to draw conclusions on the
reports no difference in pregnancy rates between women
fifth day, more research would be desirable to confirm this
with a delay within 72 h and those with a delay of 72 h or
finding, probably using surveillance epidemiological studies.
more, but the comparison reported by the authors includes
In conclusion, combining four studies with similar
LNG and mifepristone combined from one trial and the
protocols, it was shown that there was no evidence of an
delay of 72 h or more includes both the fourth and fifth day,
increase in the risk of pregnancy when LNG 0.75 mg,
which in our findings demonstrates a different efficacy. The
repeated 12 h later or in a single dose of 1.5 mg, was
results presented in this report, instead, are for LNG only and
administered for EC on the second, third and fourth day after
include a sufficient number of women to make separate
unprotected intercourse, compared to administration on the
comparisons of efficacy between the first and fourth day and
first day. However, under certain conditions an increasing
trend in pregnancy rates might exist within 72 h of
It is worth noting that the comparison between the first
administration; therefore it is advisable to administer LNG
and fifth day, although based on only 230 women, results in
as soon as possible after unprotected intercourse. Delaying
the 95% confidence interval for the OR not including 1,
LNG administration until the fifth day after unprotected
implying that receiving LNG on the fifth day was
intercourse increases the risk of pregnancy over five times
significantly less effective at the 5% level of significance
compared with administration within 24 h. It is uncertain
whether LNG administration on the fifth day still offers some
Two of the trials in this review admitted women
protection against unwanted pregnancy.
within 120 h of unprotected coitus. The aims of these trialswas to compare different regimens, not to estimate absolute
efficacy. Conclusions about whether LNG is effective — or
[1] Task Force on Post-ovulatory Methods of Fertility Regulation.
not — compared to placebo or effective on particular days
Randomised controlled trial of levonorgestrel versus the Yuzpe
following unprotected intercourse should be made with
regimen of combined oral contraceptives for emergency contraception.
caution, since a comparison to placebo was not included in
those trials (it would not be ethical to do so) and the number
[2] von Hertzen H, Piaggio G, Ding J, et al, for the WHO Research Group
of women with more than 72 h of delay was only 11–12% of
on Post-ovulatory Methods of Fertility Regulation. Low dosemifepristone and two regimens of levonorgestrel for emergency
contraception: a WHO multicentre trial. Lancet 2002;360:1803–10.
This analysis has limitations: the comparison of preg-
[3] Olukayode AD, Godfrey E, Piaggio G, von Hertzen H, on behalf of the
nancy rates in the different categories of delay does not have
Nigerian Network for Reproductive Health Research and Training. A
the advantages of a randomized comparison and might be
randomized, double-blind, noninferiority study to compare two
subject to bias due to different characteristics of women at
regimens of levonorgestrel for emergency contraception in Nigeria. Contraception 2010;82:373–8.
trial entry in the different categories of delay. In particular,
[4] Piaggio G, von Hertzen H, Grimes DA, Van Look PFA, on behalf of
the expected pregnancies according to the day of the cycle on
the Task Force on Post-ovulatory Methods of Fertility Regulation.
which unprotected intercourse occurred might have been
Timing of emergency contraception with levonorgestrel or the Yuzpe
different across the categories of delay. However, adjustment
for baseline characteristics in the two oldest trials produced
[5] Piaggio G, von Hertzen H. Effect of delay in the administration of
levonorgestrel for emergency contraception. Paper presented at the
similar results (not presented), indicating that if bias was
XVII FIGO World Congress of Gynecology and Obstetrics, 2–7
present, it was not a factor strongly affecting efficacy rates.
November 2003, Santiago, Chile; 2003.
A second limitation is the difference between trials in the
[6] Ho PC, Kwan MSW. A prospective randomized comparison of
efficacy trend. Heterogeneity across trials in the effect of
levonorgestrel with the Yuzpe regimen in post-coital contraception.
delay on pregnancy rates did not reach significance at the 5%
[7] Review Manager (RevMan) [Computer program]. Version 5.0.
level and the I2 statistic indicated only ‘moderate heteroge-
Copenhagen: The Nordic Cochrane Centre, The Cochrane Collabora-
neity’; therefore, we combined the results. However, two of
G. Piaggio et al. / Contraception xx (2011) xxx–xxx
[8] Wilcox AJ, Weinberger CR, Baird DD. Timing of sexual intercourse in
[11] Meng CX, Andersson KL, Bentin-Ley U, Gemzell-Danielsson K,
relation to ovulation: effects on the probability of conception, survival
Lalitkumar PG. Effect of levonorgestrel and mifepristone on
of the pregnancy, and sex of the baby. N Engl J Med 1995;333:
endometrial receptivity markers in a three-dimensional human
endometrial cell culture model. Fertil Steril 2009;91:256–64.
[9] WHO Task Force on Post-ovulatory Methods. Comparison of three
[12] Glasier AF, Cameron ST, Fine PM, et al. Ulipristal acetate versus
single doses of mifepristone as emergency contraception: a randomised
levonorgestrel for emergency contraception: a randomised noninfe-
riority trial and meta-analysis. Lancet 2010;375:555–62.
[10] Lalitkumar PG, Lalitkumar S, Meng CX, et al. Mifepristone, but not
[13] Cheng L, Gülmezoglu AM, Piaggio G, Ezcurra E, Van Look PFA.
levonorgestrel, inhibits human blastocyst attachment to an in vitro
Interventions for emergency contraception (Review). The Cochrane
endometrial three-dimensional cell culture model. Hum Reprod 2007;
Management of Acute Pain After An Emergency Department Visit: Acetaminophen (Tylenol) 1,0000 mg every 6 hours as needed Acetaminophen (Tylenol) 1,0000 mg every 6 hours AND Ibuprofen (Advil) 600 mg every 6 hours as needed for breakthrough pain Acetaminophen (Tylenol) 1,000 mg every 6 hours AND Ibuprofen (Advil) 600 mg every 6 hours AND Narcotics as needed for breakth
 Effect on pregnancy rates of the delay in the administration of
levonorgestrel for emergency contraception: a combined analysis of four
Gilda Piaggioa,⁎, Nathalie Kappb, Helena von Hertzenc
aStatistika Consultoria, São Paulo, Brazil
bWorld Health Organization, 1211 Geneva, Switzerland
cConcept Foundation, 1211 Geneva, Switzerland
Received 29 October 2010; revised 6 November 2010; accepted 16 November 2010
Background: Levonorgestrel is an effective method for emergency contraception (EC) and is used worldwide. Consistent with itsmechanism of action in delaying ovulation, the earlier it is administered within 72 h of an unprotected act of intercourse, the more effective itis. There is uncertainty, however, about its effectiveness after 72 h. This analysis explores the effect of 24-h intervals of delay inlevonorgestrel administration on pregnancy rates when used until 120 h of an unprotected act of intercourse.
Effect on pregnancy rates of the delay in the administration of
levonorgestrel for emergency contraception: a combined analysis of four
Gilda Piaggioa,⁎, Nathalie Kappb, Helena von Hertzenc
aStatistika Consultoria, São Paulo, Brazil
bWorld Health Organization, 1211 Geneva, Switzerland
cConcept Foundation, 1211 Geneva, Switzerland
Received 29 October 2010; revised 6 November 2010; accepted 16 November 2010
Background: Levonorgestrel is an effective method for emergency contraception (EC) and is used worldwide. Consistent with itsmechanism of action in delaying ovulation, the earlier it is administered within 72 h of an unprotected act of intercourse, the more effective itis. There is uncertainty, however, about its effectiveness after 72 h. This analysis explores the effect of 24-h intervals of delay inlevonorgestrel administration on pregnancy rates when used until 120 h of an unprotected act of intercourse.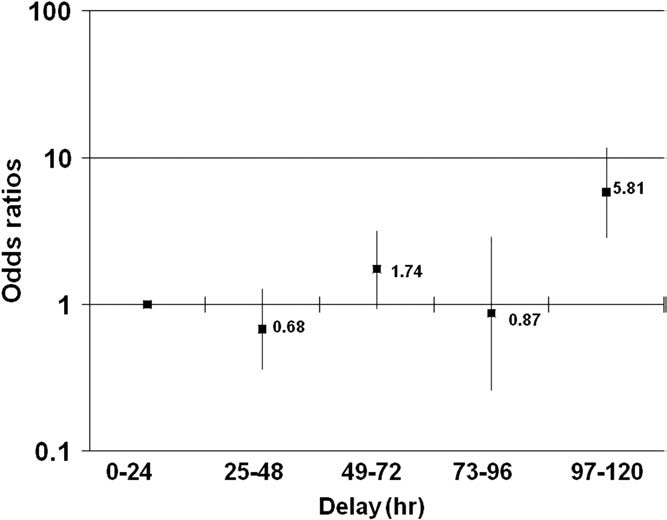 G. Piaggio et al. / Contraception xx (2011) xxx–xxx
Table 2Number of pregnancies, number of women and pregnancy rates (%) by 24-h intervals of delay between an unprotected act of intercourse and administration ofLNG, and ORs of pregnancy for intervals after 24 h with respect to the first 24 h, with 95% CIs, for four WHO studies and for the combined data
was 5.2 (95% CI 2.7% to 8.9%), below the 6% to 8%
There was some indication of a different pattern in the
expected without treatment but not significantly different
effect of delay in two of the trials where the
pregnancy rates showed an increasing trend within 72 h.
G. Piaggio et al. / Contraception xx (2011) xxx–xxx
Table 2Number of pregnancies, number of women and pregnancy rates (%) by 24-h intervals of delay between an unprotected act of intercourse and administration ofLNG, and ORs of pregnancy for intervals after 24 h with respect to the first 24 h, with 95% CIs, for four WHO studies and for the combined data
was 5.2 (95% CI 2.7% to 8.9%), below the 6% to 8%
There was some indication of a different pattern in the
expected without treatment but not significantly different
effect of delay in two of the trials where the
pregnancy rates showed an increasing trend within 72 h.