He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Sd-ladas.pblogs.gr
A Glass of Water Immediately Increases Gastric pH in HealthySubjects
George Karamanolis Æ Ioanna Theofanidou Æ Marina Yiasemidou ÆEvangelos Giannoulis Æ Konstantinos Triantafyllou Æ Spiros D. Ladas
Received: 18 February 2008 / Accepted: 10 April 2008 / Published online: 13 May 2008Ó Springer Science+Business Media, LLC 2008
Onset of action of antisecretory agents is of
pivotal importance for patients with gastroesophagealreflux disease (GERD) treated ‘‘on-demand.’’ Aim To study
Up to 20% of the general population has heartburn at least
the acute effect of acid-inhibiting drugs and water admin-
twice a week while 1–4% of the Western population
istration on gastric pH. Method A cross-over study was
consumes acid-suppressive drugs, most often for gastro-
performed in 12 H. pylori (-), healthy subjects (6 men;
esophageal reflux disease (GERD) [].
mean age: 26 years). A single oral dose of the following
The majority of symptomatic GERD patients have non-
agents was received with a wash-out period between each
erosive reflux disease (NERD) and require treatment with
study: a glass of water (200 ml), antacid, ranitidine, ome-
acid suppressive drugs for symptom relief However,
prazole, esomeprazole, and rabeprazole. Gastric pH was
GERD is a chronic disease, and relapse of symptoms
recorded for 6 h after drug intake. Results Water increased
occurs frequently. Studies have shown relapse rates in up to
gastric pH [4 in 10/12 subjects after 1 min. The time
70–80% in patients with NERD after they finish an initial
(median) needed to pH [4 was for: antacid 2 min, raniti-
course of therapy [Therefore, maintenance therapy is
dine 50 min, omeprazole 171 min, esomeprazole 151 min,
often required for ongoing symptom control.
and rabeprazole 175 min. Gastric pH [4 lasted for 3 min
Treatment to relieve symptoms as they occur may be the
after water and for 12 min after antacids; it remained [4
best way to manage NERD patients. In the on-demand
until the end of recording in: 4/12 subjects with ranitidine,
approach, symptoms are allowed to recur, and patients take
11/12 with rabeprazole, and all with omeprazole and
an acid-suppressing drug when symptoms arise Since
esomeprazole. Conclusion Water and antacid immediately
reflux symptoms are often transient, medication for on-
increased gastric pH, while PPIs showed a delayed but
demand therapy should have a rapid onset of action for
prolonged effect compared to ranitidine.
prompt symptom relief and act long enough to preventrecurrent symptoms. Many agents are currently available
for the treatment of heartburn, including antacids, H2-
receptor antagonists (H2RAs), and proton pump inhibitors(PPIs) []. PPIs have been established to be potent inhib-itors during chronic administration however, H2RAs
G. Karamanolis Á I. Theofanidou Á M. Yiasemidou Á
are reported to have a faster onset of antisecretory activity
Hepatogastroenteroly Unit, 2nd Department of Internal
We have observed that many patients with heartburn
Medicine-Propaedeutic, ‘‘Attikon’’ University General Hospital,
report immediate relief after drug administration. The
majority of patients take acid-suppressive drugs with tap
water, which usually has an alkaline pH. Thus, we
Hepatogastroenteroly Unit, First Department of Internal
hypothesized that the water could be the putative factor of
Medicine-Propaedeutic, ‘‘Laikon’’ General Hospital, Athens
the early post-administartion effect, whereas the active
University, Ag. Thoma 17, 11527 Athens, Greecee-mail: [email protected]
drug results in the later and prolonged action.
The aims of our prospective study on healthy subjects
location of LES was determined by stationary esophageal
were: (1) to compare the acute effects (onset and the
duration) on intragastric pH of antacids and acid-inhibiting
Values for intragastric pH were recorded on a Digitr-
drugs (H2RAs and PPIs) and (2) to investigate the effect of
apper Mk III (Synectics Medical, Stockholm, Sweden)
every 5 s. At the end of pH monitoring, the recorded datawere uploaded from the data logger to a computer and wereanalyzed using a commercially available software program
Subjects were 12 (6 men; mean age: 26 years, range 21–
Gastric juice was obtained from one healthy fasting vol-
30) healthy volunteers with no symptoms of gastrointesti-
unteer. In 20 ml of the sample of gastric juice (pH 1.3), we
nal or other disease. None of the subjects was receiving any
added different volumes (50, 100, and 200 ml) of tap
acid-suppresive medications or medication likely to inter-
water, distilled water, and two commercially available
act with acid secretion. Volunteers with a negative 13C-
bottled mineral waters (Table ). The pH of the used bot-
urea breath test for Helicobacter pylori infection were
tled water is into the range (from 6.0 to 7.9) of that
included in the study. All subjects were doctors or nurses of
characterizing nearly all the worldwide bottled mineral
our unit and medical students who volunteered to partici-
pate in the experiments. Written informed consent wasobtained from each volunteer, and the study was carried
Further Experiments with Water Administration
out in accordance with the Helsinki Declaration.
Further intragastric pH studies were performed in five
subjects. This ancillary study was performed to clarify theearly effect of water volume on the gastric pH. Each vol-
The study was an open-label, randomized, crossover trial.
unteer drank 50, 100, and 200 ml of water in a random
The volunteers were fasted overnight before treatment, and
order with a washout period of 60 min between each study.
study medications were randomly given in the morning. Asingle oral dose (swallowed with 15 ml of water) of each of
the following medications was received with a washoutperiod of at least 2 days between each study [
The effects of each medication and of water were com-
aluminium hydroxide plus magnesium oxide 400 mg,
pared for the time (in minutes) required for pH to increase
ranitidine 150 mg, omeprazole 20 mg, rabeprazole 20 mg,
to [4 after their ingestion. The time for which intragastric
and esomeprazole 40 mg. Moreover, administration of
pH remained above 4 during the 6-h monitoring period
200 ml (a glass) of water was studied in all subjects. All
after taking the study drug and water was also measured.
subjects underwent pH monitoring on 6 separate days, andthey were blinded for the administered drug.
Each study drug was administered 5 min after an
intragastric pH value of 1–3 was continuously recorded for
Results in the text and tables are expressed as median with
5 min. Gastric pH monitoring was continued for 6 h after
ranges. Statistical analysis of paired data was performed
intake of the medication. Smoking and ingestion of food orliquids were prohibited during the pH recording periods.
In vitro experiment: effect of different volumes of various
Gastric pH data were collected using an antimony pH
catheter with external reference (Synectics Medical Inc.),
which was inserted transnasally under local anesthesia
(xylocaine spray 2%). The catheter was calibrated before
insertion using standard buffer solutions of pH 1.0 and 7.0
at room temperature. It was positioned 10 cm below the
proximal border of the lower esophageal sphincter (LES),
and a pH value of 1–3 was recorded for 5 min. The
using non-parametric tests as appropriate. A P-value \0.05
time to pH [4 (median: 50 min) compared to omepra-
zole (median: 171 min, P \ 0.05), rabeprazole (median:175 min, P \ 0.05), and esomeprazole (median: 151 min,P \ 0.05). No significant difference was found among
omeprazole, rabeprazole, and esomeprazole.
Figure shows the median time taken for gastric pH to
Administration of water and of antacids provided a short
increase [4 for all study drugs. Water administration
duration of pH control (median: 3 and 12 min, respectively).
immediately increased gastric pH [4 in 10/12 subjects.
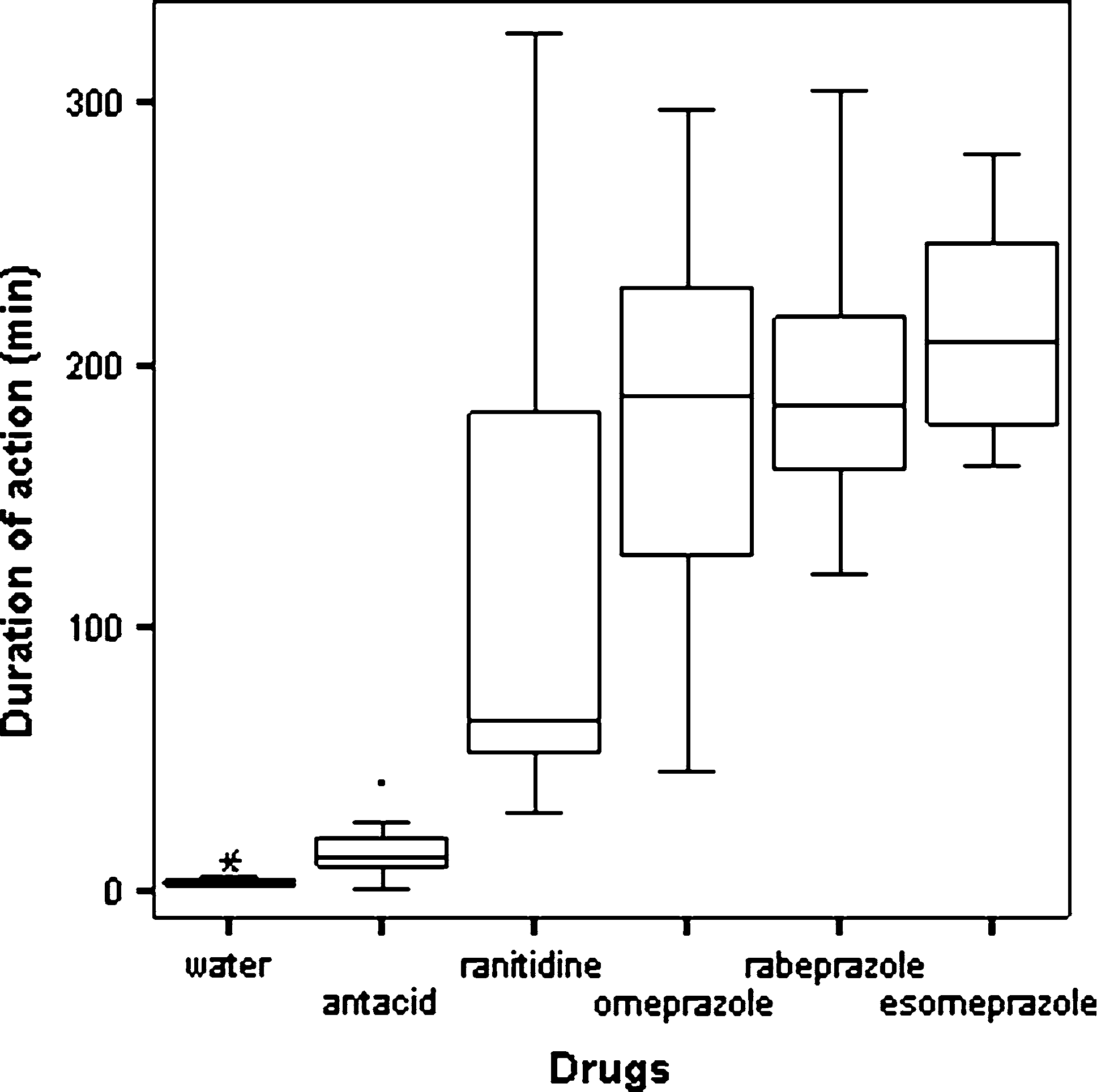
Figure shows median time that gastric pH remained[4. A
Antacids increased gastric pH [4 within 2 min (Fig.
sustained pH [4 was observed until the end of the 6-h study
The onset of antisecretory action of the remaining study
period in 4/12 subjects on ranitidine, in 11/12 subjects on
drugs occured in the majority of subjects within 2 h of drug
rabeprazole, and in all subjects on omeprazole and
administration. Ranitidine provided faster increase in
esomeprazole. The pH was maintained [4 for shorter peri-ods with ranitidine when compared with omeprazole,rabeprazole, and esomeprazole (median: 65 vs. 189, 185,209 min, respectively; P \ 0.05). No significant diffe-rence was found among omeprazole, rabeprazole, andesomeprazole.
Changes of fasting gastric juice pH after administration ofdifferent volumes of tap, distilled, and mineral bottledwater are shown in Table . We observed that byincreasing the volume of added water, intragastric pHincreased. This increase also depended on the initial pH ofthe type of added water (Table
Fig. 1 Time taken until pH rise [4 (median, 25th–75th percentileand 9th–95th percentile)
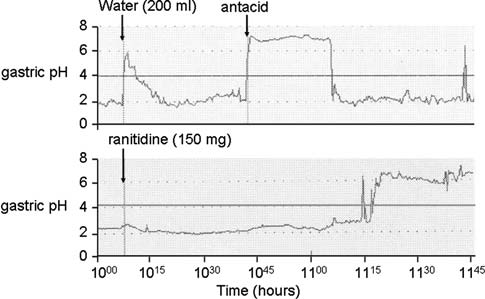
Fig. 2 Intragastric pH after administration of a glass of water and of
Fig. 3 Duration for which pH remained [4 (median, 25th–75th
Intragastric pH after Water Administration
that observed after antacids intake. A putative mechanismfor such a phenomenon is that the water as a substance with
Gastric pH remained below 4 after administration of 50 and
alkaline pH eliminates gastric acid similarly to the action
100 ml of water in all volunteers. In contrast, administra-
of antacids. Moreover, water could increase the total vol-
tion of 200 ml of water induced increase of pH [4 in all
ume of gastric fluid, decreasing the concentration of acid in
subjects after a median time of 1.5 min (range: 1–3). The
the gastric fluid. In other words, water administration
pH remained above 4 for a short period of time (median: 2,
seems to have a dilution effect on H+ ions. The latter is
supported by the in vitro experiments and our ancillarystudy. We showed that only the administration of a glass ofwater (200 ml) induced an increase of gastric pH above 4,
whereas the smaller water volumes usually used duringdrug consumption are inadequate to induce an effect on
Our study investigated the acute effect on intragastric pH
gastric pH. Although a dilution effect could be an impor-
of water and of the early phase following an oral single
tant factor for gastric pH increase, other factors might also
dose of antisecretory drugs. Water intake and antacids
be involved. Indeed, in our in vitro studies, we observed a
showed an immediately increase of gastric pH that lasted
large increase of pH (e.g., from 1.4 to 5.4) with the addition
for a few minutes. Ranitidine showed a faster onset of
of 200 ml of tap water to 20 ml of gastric juice sample.
action than did PPIs (omeprazole, rabeprazole, and
Thus, on the basis of dilution alone, one would predict that
esomeprazole). In contrast, maintenance of a gastric pH
the [H+] of the sample would decrease 11-fold, the dilution
above 4 was longer with all PPIs compared to ranititidine
factor, from 40 mM to 3.6 mM, or to pH 2.4. The finding
that water increased the pH to 5.4 suggests that the tap and
Although PPIs are the antisecretory drugs of choice for
mineral water used also had a high buffering capacity. This
GERD, they are not considered good candidates for treat-
buffering effect might be partly explained from the pres-
ment of very short episodes because of the rather long lag
ence of component elements, such as ions, acting as bases.
time needed to increase intragastric pH [4 ]. Indeed, our
Keeping in mind that antacids are provided as rescue
study showed that PPIs required longer time to increase
therapy in patients receiving on-demand PPI therapy [
gastric pH above 4 compared to ranitidine, and this finding
administration of a glass of water is likely to be clinically
is compatible with results reported by others [– –
meaningful. Water had a rapid onset of action comparable
However, our results are in contrast to studies showing that
to antacids and should be efficacious in relief of symp-
gastric pH failed to rise above 4 in the majority of subjects
tomatic heartburn episodes. Our study has a preliminary
after PPI treatment during a 6-h period [, We found
nature as it was performed in healthy subjects. Therefore,
that although PPIs required more time to start being effec-
further studies in patients with heartburn are needed to
tive, gastric pH above 4 was achieved in all subjects within
confirm the effect of water on gastric acidity and to support
a period of approximately 3 h after drug administration. Our
a potential role of water as rescue therapy for episodic
results support the findings of a previous study showing that
reflux symptoms during non-continuous treatment for
the onset of antisecretory action for PPIs occured within 2 h
In conclusion, we showed that in healthy subjects,
We also found that high intragastric pH with PPIs was
similarly to antacids, a glass of water (200 ml) increases
maintained for a longer period of time than with ranitidine.
gastric pH immediately. Although heartburn is usually
Gastric pH remained above 4 at the end of the study in all
associated with acidic esophageal pH and not with intra-
subjects with omeprazole and esomeprazole and in all
gastric drop in pH \4, we could hypothesize that an
except one with rabeprazole, while only four subjects with
increase of intragastic pH [4 is likely to contribute to the
ranitidine sustained a pH [4. This finding was unexpected
improvement of heartburn. Thus, patients who with ‘‘on-
because previous studies have shown that during the early
demand’’ therapy for episodic heartburn should swallow
postadministration period, H2RAs had a greater long-
the pill with at least a glass of water, as this may imme-
standing effect on gastric pH compared to PPIs , –
All studies were carried out in healthy, H. pylori (-)subjects; thus, we can speculate that differences either indoses and formulations of the drugs or in fasting status of
the subjects could explain this discrepancy.
1. Kennedy T, Jones R (2000) The prevalence of gastro-oesophageal
An important finding of our study was the fact that in the
reflux symptoms in a UK population and the consultation
majority of our subjects, administration of a glass of water
behaviour of patients with these symptoms. Aliment Pharmacol
resulted in a rapid increase of gastric pH, comparable to
2. Jacobson BC, Ferris TG, Shea TL et al (2003) Who is using
more suitable for on-demand use? J Gastroenterol 40:453–458.
chronic acid suppression therapy and why? Am J Gastroenterol
12. Khoury RM, Katz PO, Castell DO (1999) Post-pradial ranitidine
3. Fass R, Fennerty MB, Vakil N (2001) Nonerosive reflux
is superior to post-prandial omeprazole in control of gastric
disease-current concepts and dilemmas. Am J Gastroenterol 96:
acidity in healthy subjects. Aliment Pharmacol Ther 1211–1214.
4. Carlson R, Dent J et al (1998) Gastro-esophageal reflux disease
13. Robinson M (2001) New generation proton pump inhibitors:
(GORD) in primary care- an international study of different
overcoming the limitations of early-generation agents. Eur J
treatment strategies with omeprazole. Eur J Gastroenterol Hepa-
Gastroenterol Hepatol 13(Suppl 1):S43–S47
14. Hedenstrom H, Alm C, Kraft M, Grahnen A (1997) Intragastric pH
5. Tytgat GNJ, Blum AL, Verlinden M (1995) Prognostic factors for
after oral administration of single doses of ranitidine effervescent
relapse and maintenance treatment with cisapride in gastro-
tablets, omeprazole capsules and famotidine fast-dissolving tablets
esophageal reflux disease. Aliment Pharmacol Ther 9:271–280
to fasting healthy volunteers. Aliment Pharmacol Ther 11:1137–
6. Goh KL (2006) ‘‘On-demand’’ therapy for gastroesophageal
reflux disease: are current proton pump inhibitors good candi-
15. Chassany O, Bergmann JF, Simoneau G et al (1996) The com-
dates? J Gastroentrol Hepatol 21(Suppl 5):S115–S118. doi:
parative effects of single intravenous doses of cimetidine,
ranitidine, famotidine, and omeprazole on intragastric pH. Curr
7. Hatlebakk JG, Berstad A (1996) Pharmacokinetic optimization in
the treatment of gastro-oesophageal reflux disease. Clin Phar-
16. Abe Y, Inamori M, Togawa J et al (2004) The comperative
effects of single intravenous doses of omeprazole and famoti-
8. Bell NJ, Burget D, Howden CW et al (1992) Appropriate acid
dine on intragastric pH. J Gastroenterol 39:21–25.
suppression for management of gastro-oesophageal reflux dis-
17. Pantoflickova D, Dorta G, Ravic M et al (2003) Acid inhibition
9. Hurlimann S, Abbuhl B, Inauen W et al (1994) Comparison of
on the first day of dosing: comparison of four proton pump
acid inhibition by either oral high-dose ranitidine or omeprazole.
10. Arnestad JS, Klevemand PM, Waldum HL (1997) In single doses
18. Zacny J, Zamakhshary M, Skertis I, Veldhuyzen van Zanten S
ranitidine effervescent is more effective than lansoprazole in
(2005) Systematic review: the efficacy of intermittent and
decreasing gastric acidity. Aliment Pharmacol Ther 11:355–358.
on-demand therapy with histamine H2-receptor antagonists or
proton pump inhibitors for gastro-oesophageal reflux disease
11. Inamori M, Towaga JI, Iwasaki T et al (2005) Early effects of
patients. Aliment Pharmacol Ther 21:1299–1312. doi:
lafutidine or rabeprazole on intragastric acididty: which drug is
O segmento Citigold passa a se chamar de suporte a clientes, implantamos um Citigold Private Client. A mudança, no núcleo de atendimento diferenciado entanto, não se restringe à marca; ela no CitiPhone Banking e inauguramos também consolida o atendimento espe-cializado e a plataforma diferenciada sempre com uma equipe altamente es-de produtos aos quais os clientes têm pecializada. Nosso
J Musculoskel Neuron Interact 2003; 3(1):71-76 Original Article Bone mineral density in hypoparathyroid women on LT4 suppressive therapy. Effect of calcium and 1,25(OH)2 vitamin D3 treatment F. Hawkins1, F. Escobar-Jiménez2, E. Jfidar1, M.M. Campos2, M.B. L fi pez Alvarez1, G. Mart›nez D›az-Guerra1 1Service of Endocrinology, University Hospital 12 de Octubre, Madrid2Servi
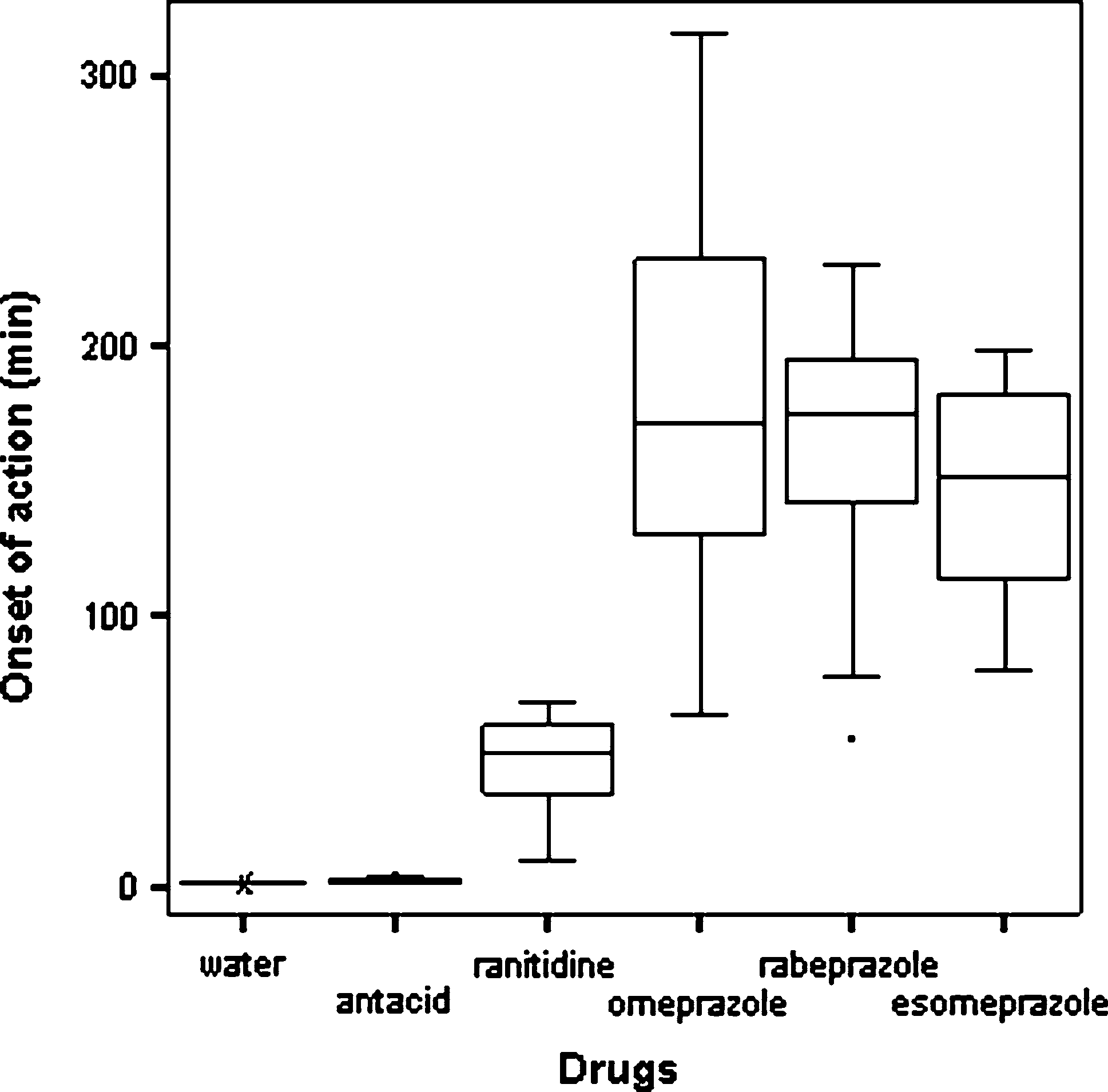
 using non-parametric tests as appropriate. A P-value \0.05
time to pH [4 (median: 50 min) compared to omepra-
zole (median: 171 min, P \ 0.05), rabeprazole (median:175 min, P \ 0.05), and esomeprazole (median: 151 min,P \ 0.05). No significant difference was found among
omeprazole, rabeprazole, and esomeprazole.
using non-parametric tests as appropriate. A P-value \0.05
time to pH [4 (median: 50 min) compared to omepra-
zole (median: 171 min, P \ 0.05), rabeprazole (median:175 min, P \ 0.05), and esomeprazole (median: 151 min,P \ 0.05). No significant difference was found among
omeprazole, rabeprazole, and esomeprazole.