He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Phosphatidylcholine: a superior protectant against liver damage
Phosphatidylcholine: A Superior Protectant Against Liver Damage Parris M. Kidd, Ph.D.
Phosphatidylcholine (PC) is one of the most important support nutrients for the
liver. PC is a phospholipid, a large biological molecule that is a universal building blockfor cell membranes. A cell’s membranes are its essence: they regulate the vast majorityof the activities that make up life. Most liver metabolism occurs on cell membranes,which occupy about 33,000 square meters in the human. More than 2 decades ofclinical trials indicate that PC protects the liver against damage from alcoholism,pharmaceuticals, pollutant substances, viruses, and other toxic influences, most ofwhich operate by damaging cell membranes.
The human liver is confronted with tens of thousands of exogenous substances.
The metabolism of these xenobiotics can result in the liver’s detoxicative enzymesproducing reactive metabolites that attack the liver tissue. Dietary supplementationwith PC (a minimum 800 mg daily, with meals) significantly speeds recovery of theliver. PC has also been shown to be effective against alcohol’s liver toxicity in well-controlled studies on baboons.
PC has other qualities that enhance its usefulness as a dietary supplement. PC
is safe, and is a safer means for dietary choline repletion than choline itself. PC is fullycompatible with pharmaceuticals, and with other nutrients. PC is also highly bioavailable(about 90% of the administered amount is absorbed over 24 hours), and PC is anexcellent emulsifier that enhances the bioavailability of nutrients with which it is co-administered. PC’s diverse benefits and proven safety indicate that it is a premier livernutrient. (Alt Med Rev 1996;1(4):258-274)
Phosphatidylcholine (PC) is a phospholipid nutrient that is a major building block for
all known cells.1 PC is the most abundant constituent of cell membranes, the thin and delicateyet dynamic surfaces on which cells carry out most of their activities (Fig. 1). The “workhorse”parenchymal cells that make up the liver are especially reliant on their membranes,2 and it hasbeen estimated that the human liver as a whole encapsulates some 33,000 square meters of cellmembrane.3 The liver’s wide range of functions, as well as its capacity for ongoing renewal,hinge on its ability to make new cell membranes, which are on average 65% PC. Decades ofbasic and clinical research on this nutrient indicate that it is critical for optimal liver function.
Page 258 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
The Human Liver, the CELL INTERIOR Detoxification Paradox, and PC PHOSPHATE GLYCEROL
disarming and disposing of toxins, yet is
itself vulnerable to toxic attack. Such toxicattack is both endogenous (from toxins
FATTY ACID
generated in the liver), and exogenous (due
to toxins coming from the outside). Simi-
lar metabolic mechanisms are employedto deal with the toxins coming from either
CELL EXTERIOR
source, but due to the stressful influencesof modern life, toxic overload is a con-
Figure 1. Phosphatidylcholine, major constituent
of cell membrane systems. Left: Molecular plan
The healthy liver is the body’s largest
of PC. Middle: PC, membrane building block.
organ and is probably also its most meta-
Right: the basic membrane plan, with proteins
bolically versatile. The liver carries out
hundreds, if not thousands, of sophisti-cated enzymatic reactions along numerous
metabolic pathways. Enzymes residing within
body of potential toxins, the liver paradoxi-
the membranes of the parenchymal cells pro-
cally generates toxins that can damage the liver
duce biological molecules by synthesis from
tissue. This can happen because evolution has
smaller molecules, by the modification of pre-
existing metabolites or from newly-absorbed
activate the liver’s natural enzyme detoxifica-
nutrients. The parenchymal cells also process
tion pathways, but often the metabolites that
products into water-soluble compounds for
“bioactivation” are more toxic than the start-
subsequent excretion. With the myriad of func-
ing substrates. Whether their toxicity occurs
tions that it performs, the liver plays a pivotal
directly or following bioactivation, virtually
role in maintaining homeostasis, i.e., health
all of the agents that damage the liver do so by
in all its aspects. But these routine liver func-
way of attack on the membrane systems of the
tions do generate intrinsic, potentially toxic
survival and specialized functioning of all
well equipped with protective antioxidant
cells. In order to carry out its metabolic re-
enzymes and with water-soluble antioxidants
sponsibilities, the liver parenchymal cells are
such as glutathione, cysteine, and taurine to
densely packed with membranes. Given this
central role of membranes in the liver’s func-
tions, the demonstrated superiority of PC in
challenge posed to the liver’s defenses by food-
supporting the liver against damage is thor-
borne toxins and by the bioactivation products
oughly consistent with the known mechanisms
of xenobiotics, including lifestyle-related
of liver homeostasis, toxic liver damage, and
the liver’s recovery processes. Out of this
detoxification enzyme systems can be diverted
comes a dramatic conclusion: PC is the single
most important nutrient for the liver.
metabolites that attack their maker. Last but
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 259
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
Figure 2. Schematic of the liver parenchymal cell, showing the internal functional units or organelles. Those superscriptedM are made up of membranes or rely on membranes to function. Modified from Sherlock S, Dooley J. Diseases of the Liver and Biliary System. Oxford: Blackwell Scientific Publications; 1993.
not least, by being the first way-station for the
vestigated PC for the management of liver
blood draining the intestines (via the portal
damage coming from a variety of toxic insults.
circulation), the liver tissue is directly exposed
to preformed toxins that enter by the oral route.
Wallnoefer and Hanusch in Germany followed
650 subjects with various degrees of liver dam-
liver is evolutionarily equipped to cope with
age for at least 5 years.6 This trial relied on
the tens of thousands of toxins generated by
biopsy, conducted in conjunction with blood
modern circumstances: pharmaceuticals, pol-
analyses and clinical tests, to assess the scope
lutants, and other toxins associated with a self-
and character of liver damage.7 The subjects
abusive lifestyle. As the liver becomes over-
received PC for periods that ranged from 4
burdened with such toxins, its stores of pro-
weeks to several years. The distributions of
tective antioxidants are progressively de-
subjects, listed in groups according to approxi-
pleted.4 Parenchymal cells die, and cell death
mate degree of damage severity, was as fol-
spreads zonally. Left unchecked, necrotic and
lows: fatty degeneration, n=130; acute inflam-
inflammatory damage comes to threaten whole
mation, n=157; persistent inflammation (sub-
acute and chronic), n=41; chronic inflamma-tion, n=122; chronic aggressive inflammation,
Overall Clinical Benefits of PC for the
n=70; advanced fibrotic damage, n=130. All
subjects were begun on intravenous PC (950mg*) along with oral PC (450-700 mg*), un-
til blood parameters began to return to nor-
trials, conducted mostly in Europe, have in-
mal; they were then shifted to oral PC only.
Page 260 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
favor of PC (5 of the 7 were 95% significant),
benefited from receiving PC. Of those with
mild damage, more than half (51.1%) showed
SGOT—also became significant in favor of
excellent improvement, and many subjects ex-
PC. In suggesting that PC can benefit the vari-
perienced reversal of their fatty degeneration.
ous stages of liver damage, these findings are
In the acute inflammation group, lab measures
and biopsy indicated PC accelerated recovery
by about 10 days. In the group with persistentinflammation, PC returned the enzyme param-
Clinical Assessment of PC In
eters to normal after 30 days. In chronic ag-
Alcoholic Liver Damage
gressive inflammation , more than one-third
(35.3%) experienced benefit and among those
the single most common cause of toxic liver
with advanced fibrotic damage, 17.5% ben-
damage in Western societies. Alcohol dam-
efited. In this last group with liver damage of
ages the liver by various mechanisms.9 First,
the greatest severity, recovery was better when
it increases oxidative stress: the ethyl alcohol
PC was given intravenously as well as by the
molecule becomes metabolized by the liver
cell to acetaldehyde, which is a reactive oxi-
dant (“two-electron stealer”). Acetaldehyde
sistent inflammatory damage included in this
combines with antioxidants, often into a mo-
trial had failed to benefit from milk thistle ex-
lecular complex (an “adduct”), thereby drain-
tract (“silymarin”) or steroid drugs, but ben-
ing the liver cells of their antioxidant power.
efited from PC. The investigators commented
Acetaldehyde also reacts with enzymes and
that for the best chance of success, the man-
other proteins and with DNA, damaging these
agement of advanced liver damage should be
and sometimes causing mutations. Membrane
phospholipids and their associated fatty acids
months; and that in their clinical experience
PC proved to be the best single means for
highly reactive acetaldehyde, which can do as
much damage as many free radicals (techni-
studied 42 subjects with liver damage stem-
ming from varied causes and exhibiting all de-
has a dispersive/disruptive effect on the lipids
grees of severity.8 They divided the subjects
that make up the matrix of cell membranes.9
into 2 groups of 21 each, then provided con-
Alcohol can literally dissolve PC and other
ventional management (diet, B vitamins) to
one group. To the other group, they gave PC
(1350 mg), fortified with B1, B2, B6, B12,
and E. Blood samples and clinical assessments
were taken after 1 month, then at 2 months
(the end of the trial). The results were sub-
acetaldehyde pathways, alcohol also attacks
jected to a customized best-fit, least squares
the mitochondria, the liver cell organelles that
statistical analysis. After the first month, the
data on 7 of the 8 parameters were clearly in
*Footnote: The PC preparations used in clinical trials were soy lecithins enriched in PC, sometimes also with RDA-range levels of added B vitamins and vitamin E (herein termed fortified PC). In this text the actual PC intakes are stated,as calculated and rounded to the nearest 50 milligrams (mg). Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 261
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
the liver’s functional state cannot be improved,
exposure robs the cell of precious energy
however, the rate of collagen removal eventu-
ally falls behind the rate of collagen deposi-
more sophisticated functions. As the cell
tion, and progressive collagen accumulation
becomes more energetically compromised, its
(fibrosis, scarring) begins to obscure ever-en-
larging regions of the liver. Beyond this point,
the liver’s many functions become seriously
likely toxic basis for the early clinical stage of
compromised as it develops advanced, cir-
alcoholic liver damage termed “fatty liver.”9,10
The mitochondria are the organelles that nor-
mally burn fats (triglycerides) to make energy
against alcoholic liver damage have consis-
for the cell. When the mitochondrial mem-
tently produced favorable findings. Knuechel
branes become destroyed by alcohol, the pa-
reported in 1979 on a double blind trial con-
ducted in Germany on 40 male subjects who
metabolize fats. Pools of triglycerides then
had fatty deposits in the liver resulting from
become deposited within hepatocytes through-
alcohol intake, as verified by biopsy.11 A ma-
out the liver tissue. It is thought that as these
jority of these subjects also likely had “Stage
fatty deposits grow, they can come to occlude
2” inflammatory involvement, as indicated by
the important functions of the cell and cause
abnormally-elevated serum iron, elevated im-
and SGPT 3-5 times higher than normal.
sents a relatively mild degree of alcoholic dam-
age to the liver, which can often be reversed
through diligent personal commitment. How-
groups of 20 each. One group received a pla-
ever, if the individual continues to consume
cebo and the other, 1350 mg of fortified PC
alcohol the fat-laden parenchymal cells can
per day. Liver damage was monitored at days
begin to die off in large numbers. An inflam-
14, 28, and 56 after beginning the treatment,
matory situation then develops: in response to
substances exuded from dying liver cells, im-
AP, LDH, Chol, TG, and BR. In addition LAP,
mune cells migrate into the liver tissue from
immunoglobulins, platelets, reticulocytes, and
the circulation and attempt to “mop up” the
the blood fatty acid spectrum were measured,
debris. However, with the liver’s energetics
but only at the beginning and at the end of the
mised, the stage is set for the inflammatory
process to get out of hand and usher in a
PC intake were apparent at the first time
point—2 weeks after the start. At 4 weeks,
most of the indicators of liver damage were
alcohol toxicity and is not controlled, as with
clearly more improved for the PC group than
the continuation of alcohol consumption, cells
for the placebo group. By 8 weeks, the trial’s
in the liver called lipocytes are transformed
culmination, all the main parameters of liver
and begin to produce collagen, which is the
primary molecular basis for connective tissue
<0.05). The parameters LAP and IgA-IgG-
deposition and fibrosis. At first the liver may
IgM, measured only at the end of the trial, also
adapt, accelerating its removal of collagen to
keep pace with the rate of new deposition. If
Page 262 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
in the liver. These findings are consistent with
ducted at the end of the trial, by a qualified
those from Buchman and collaborators (1992),
investigator not informed of the randomiza-
who gave PC double-blind to 15 subjects with
tion code. Of the PC group of 20 subjects, 6
fatty liver of non-alcoholic origin as part of
were judged very good and 14 good. Of the
placebo group, none was very good, 7 were
change. The differences were statistically
which if left untreated can become life-threat-
highly significant in favor of the PC group.
ening. In 1990, Panoz and collaborators re-
No side effects from the PC were observed. In
ported on a double-blind trial conducted in
this 2-month trial, PC definitely benefited sub-
England.14 The researchers divided 46 subjects
jects with alcoholic liver damage. It did not
with liver inflammation from alcohol abuse
completely resolve the more severe inflamma-
(verified by biopsy) into two groups. The PC
tory indicators, which perhaps could have been
group were placed on a high intake—about 4.6
achieved had the trial gone for a longer pe-
grams daily—of fortified PC, in contrast to the
placebo group, and both groups were periodi-
cally assessed for 2 years. By the end of the
San Martin organized a double-blind trial.12
trial there had been deaths in both groups, but
They drew 20 subjects with alcohol-induced
a trend was seen toward increased survival in
fatty liver deposits from a population and com-
the PC group (p=0.086, short of the p<0.05
pared them with 20 matched control subjects.
required for statistical significance). The group
As in the Knuechel study just described, forti-
that seemed to benefit the most was the inter-
fied PC was given at 1350 mg per day. The
mediate stage of severity (Pugh’s B classifi-
trial went for 12 weeks, and blood samples
cation). Tolerance of the relatively high intake
were taken at the beginning and at the end of
this trial period. Initially the indicators SGGT,
SGOT, SGPT, AP, and bilirubin all were higher
clinical trials conducted on human subjects
in the PC group than in the controls, but by
with alcoholic liver damage are generally con-
the trial’s end they were significantly reduced
sistent with a large body of data from animal
and were lower than the controls. Alpha-2-
globulin was also significantly increased
(p<0.01). Clinical assessment at the trial’s end
liver “detoxification” seemingly is to make
determined that in the PC group 3 subjects
potentially problematic substances water-
were good, 14 were average, while 3 had not
soluble, suitable for later excretion into the bile
improved. In the placebo group, 0 subjects
or the urine. Therefore the healthy liver
were good, 9 were average, and 11 (more than
half) had experienced no benefit. The authors
concluded, “it is our view that the use of
charge on the molecule. It then attempts to
highly-unsaturated phosphatidylcholine for
therapy of alcohol-dependent steatoses [fatty
“activated” metabolite with glucuronic acid or
with glutathione or other antioxidants to render
it water-soluble.4 If the first phase enzyme
marized establish the benefits of PC as an oral
systems become induced, generating copious
nutritional supplement for the earliest clini-
amounts of exceedingly reactive activated
cally-characterized stage of liver damage from
molecules, then the resources for conjugation
alcohol abuse - the presence of fatty deposits
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 263
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
Figure 3. Inhibition of alcoholic liver damage in baboons fed an adequate diet with ethyl alcohol. Left: alcohol given daily along with PC to six baboons results in minimal fibrotic damage, stable for up to 8 years. Right: after PC is removed from the diet of three babbons, damage progresses to end-stage fibrosis (“cirrhosis”) in 1-2 years. From Lieber et al.15
can become insufficient. When this happens,
clinical benefits against liver damage from
activation can still proceed but conjugation
many causes. In the case of alcohol, the most
fails, and the liver tissue becomes a sitting duck
clinically relevant animal research to date has
been the “baboon model” of alcoholism de-
metabolites. Alcohol and many xenobiotics
veloped by Leiber and his colleagues at the
can actually induce, i.e., turn on, the Phase 1
systems, thereby racking up the potential for
Bronx Veterans Affairs Medical Center in New
York City, for more than 2 decades.10,15,16,48
metabolites. This can explain why combined
Their findings constitute compelling evidence
that dietary supplementation with PC is effec-
pollutants or other xenobiotics can be severely
tive against alcoholic liver damage. In early
threatening to the liver’s integrity.4,9,10 In this
experiments they fed alcohol to rats, and found
scenario any agent that turns on Phase 1 of the
that it impaired phospholipid synthesis in the
detoxification system, can cause the system
rat liver. This partially accounts for fats accu-
to concurrently convert excessive amounts of
mulating in the liver cells (“fatty liver”), since
a second (or third) agent to reactive, oxidant
PC and other phospholipids are needed to me-
tabolize triglycerides. Then, for an “experi-mental model” closer to the human state, they
The Baboon Model of Alcoholic Liver
turned to research on baboon primates (Fig. 3).
boons on a daily regimen of alcohol intake.
Over a period of years most of the baboons
the means by which PC exerts its impressive
developed features of alcoholic liver damage
Page 264 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
that closely resembled those seen in humans,
making this is a good “animal model” for hu-
man liver disease. The researchers also de-
were subsequently taken off PC while continu-
veloped sophisticated methods for quantitat-
ing to be fed alcohol. These baboons rapidly
ing the tissue changes seen in liver biopsy
progressed to extensive liver fibrosis (equiva-
samples, and refined biochemical analyses for
lent to advanced liver damage). From this
use on small amounts of biopsy material.
study and a follow-up study using a similar
design17, Lieber’s group were able to firmly
sign, they set up two main groups of baboons,
conclude that PC is an effective means for
one of which received alcohol along with PC,
halting (not merely slowing) the progression
the other receiving only alcohol.15 After run-
from early-stage alcoholic liver damage into
ning this primate trial for several years and
late-stage generalized fibrosis (cirrhosis). (Fig-
decoding their results, Lieber’s group found
ure 3) PC is unique among both nutrients and
that the baboons fed alcohol with PC devel-
drugs, as was pointed out in a supportive peer
oped fatty liver and mild fibrosis, but did not
editorial,18 in its ability to halt the clinical pro-
Figure 4. Summary of the mechanisms of liver damage by drugs. Note the lipid peroxidation events that result in cell membrane damage. From Hoyumpa and Schenker.19
progress to advanced liver damage for six
years or longer. In contrast, the majority of
Subsequent in vitro experiments by
baboons fed alcohol without PC progressed
Lieber’s group16 showed that the lipocytes, the
to advanced fibrosis (p < 0.005). While PC
did not block the development of fatty liver in
amounts of fats, under the influence of alco-
baboons that continued to receive alcohol, it
hol become transformed to collagen-produc-
dramatically slowed the progress to advanced
ing cells (called “transitional cells”). In the
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 265
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
intact, alcohol-treated liver these transitional
riety of toxic agents other than alcohol. The
cells intensify collagen production, but initially
trials reported in this category are sparse be-
the liver keeps up by breaking down collagen
cause of the difficulties in assembling victims
faster (via increased collagenase enzyme ac-
of toxic exposures. However, some clinical
tivity). As alcohol damage progresses, the
trials have been accomplished, and their find-
balance shifts: the liver’s collagenase activity
ings indicate PC is also unique in its protec-
drops and continued collagen production by
tion of the liver against toxins other than al-
the transitional cells results in progressive col-
lagen deposition and extensive fibrosis. This
eventually deprives the liver of most of its
function (the state of cirrhosis). It may well
(“xenobiotics”) entering the body. Blood car-
be that in the baboons fed PC along with alco-
rying newly-absorbed molecules proceeds di-
hol, excessive collagen production was par-
rectly to the liver from the intestines. Sub-
tially blocked by PC, and collagen breakdown
stances as diverse as drugs, whether legal or
was increased for a sustained period (also via
illegal; anesthetics; herbs, foods, and pollut-
ants can be rendered more toxic after reach-
supplementation with PC seemingly restored
ing the liver, due to bioactivation by the liver
normal collagen balance in the transitional
P450 and related enzyme pathways (see Fig.
cells, thereby blocking further fibrosis and pro-
4). Almost all of these substances are liver
tecting the baboons for several years and po-
toxins because of their conversion into reac-
tive oxidants, which deplete the antioxidants
and other Phase 2 conjugation resources. This
suggest that advanced liver damage in humans,
unfortunate lack of discriminative activity by
clinically expressed as cirrhosis, may prove
the liver underlies most of the notorious liver
amenable to dietary PC. As a result of this
toxicity of pharmaceuticals. Excessive intake
research breakthrough by the Lieber group, ex-
of substances from any xenobiotic category
citement developed in the U.S. research com-
can predispose the liver to damage in response
munity around the potential of PC to slow, to
to otherwise-reasonable intakes of substances
stabilize, and perhaps in some cases even to
from other categories. A classic example is
reverse, alcoholic liver damage. An editorial
alcohol intake potentiating the metabolism of
in the journal Alcoholism: Clinical and Experi-mental Research discussed PC as a possible“magic bullet” for this purpose.18 The Lieber
• Drug Xenobiotics.
baboon studies also established that choline
over the counter pharmaceuticals can become
does not have comparable benefits to PC for
activated to toxic metabolites in the liver.4,19
the liver. The small choline molecule is actu-
The most heavily consumed among these are
ally part of the headgroup of the large PC
the painkillers acetaminophen, aspirin (acetyl-
molecule, but when free choline was added to
salicylic acid), ibuprofen, carbamazepine, in-
the baboon diet it proved toxic to the alcohol-
domethacin, phenylbutazone; the antibiotic
tetracycline; the anti-arrhythmic drugsamiodarone, perhexiline, and hexestrol; the
Benefits of PC Against Other Liver
blood pressure drug alpha-methyldopa; theanticlotting medication sulfinpyrazone;
the barbiturate phenobarbital; the chemo-
therapy drug methotrexate; the gout drug al-
PC supports liver cells against attack by a va-
Page 266 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
lopurinol; the anti-tuberculosis drug isoniazid
(particularly in combination with rifampin);
against acute oral trichloroethylene poison-
the CNS stimulant amineptine; the tricyclic
ing.23 Also, non-halogenated organic solvents,
antidepressant tianeptine; the anti-epileptics
allyl alcohol, carbon disulfide, ethionine, and
phenytoin and valproic acid; and the benzodi-
thioacetamide all are markedly liver-toxic, by
azepine sedative chlordiazepoxide. Anesthet-
mechanisms similar to those illustrated in Fig.
ics that are potentially toxic to the liver in-
4. Numerous case histories have been pub-
clude halothane. Of the illicit drugs, cocaine
lished that document the benefits of PC in other
has been extensively studied for its toxicity to
foods, the deathcap mushroom (Amanita
double-blind trial for which they assembled
phalloides) carries toxins that are some of the
101 tuberculous subjects who earlier had suf-
most lethal agents known. Esslinger used PC,
fered liver damage from rifampin and 2 other
at first intravenously then also orally, to avert
anti-tuberculosis pharmaceuticals.20 The PC
death in victims of deathcap poisoning.24 In
group received 1350 mg of fortified PC daily,
Esslinger’s experience, PC worked against
deathcap mushroom toxicity after milk thistle
showed good clinical improvement, but in the
extract had failed to show benefit. He called
PC group SGOT and SGPT were significantly
PC “a valuable extension to therapy for this
lower when compared with the group that re-
ceived the placebo. Kuntz and collaboratorshad made a similar finding in 1979, by giving
• Natural plant toxins. In addition to the
peanuts is also one of the most toxic natural
antiepileptic drugs, especially phenytoin, pose
substances, and also becomes operative via
a high risk of liver damage. Hisanaga and
bioactivation. Constituents of herbs also can
collaborators (1980) in Japan followed 38 sub-
be liver-toxic by bioactivation, the most noto-
jects who had received phenytoin and other
rious of these being the pyrrolizidine alkaloids
antiepileptic drugs for an average of five
found in comfrey and at least 59 other plants.
years.22 A subgroup with the highest degreeof damage (assessed by SGGT enzyme eleva-
• Radiation exposure. Klemm and Pabst in
tion), after being given PC orally for 6 months,
1964 gave PC to 161 subjects who had previ-
ously undergone radiation treatment.25 Radia-tion scattered from the head-neck area tended
• Other, non-Pharmaceutical Xenobiotics.
to damage the liver, and PC afforded partial
but clinically-meaningful protection against
number at least sixty-five thousand. One of
the chemical classes most toxic to the liver isthe chlorinated and related halogenated hydro-
• Other toxic insults to the liver, such as from
carbons, of which carbon tetrachloride has
been extensively researched as an experimen-
hepatectomy (the surgical removal of liver
tal model. Included in this class is the dry
tissue), and a variety of other sources, have
cleaning solvent trichloroethylene, along with
many commonly used herbicides and pesti-cides. In 1965 Kuntz and Neumann-Mangoldt
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 267
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
studies conducted with laboratory animals.
sue had partially recovered from its earlierdamage; focal necrosis/cell death was lessened
Controlled Trials with PC in Viral
in the PC group, and these subjects showed
Liver Damage
ducted a sophisticated trial in Czechoslova-
liver, by precipitating widespread inflamma-
kia that compared PC against drugs for the
tory breakdown which is further complicated
management of viral-related liver inflamma-
by overactivation of the immune system (au-
tion. They recruited 80 subjects with pre-
toimmune complications). Once successfully
sumed acute LV infection (viruses hepatitis A
installed in the liver parenchyma, such viruses
and hepatitis B), and divided them into four
can become chronic and very hard to dislodge.
groups of 20 subjects each.29 The first 2
Liver viruses (here simply called LV) can
groups were drawn from subjects whose bi-
wreak havoc with the liver’s functions. Medi-
lirubin levels were low (below 250 micro-
cal weapons for eliminating LV from the liver,
moles per liter) and were judged “moderately
or for ameliorating their progressive damage,
serious.” Subjects in Group I were adminis-
have been limited. Controlled clinical trials
tered fortified PC (1350 mg) along with the
have unequivocally established PC as safe and
“standard treatment” that involved diet, rest,
reliable nutritional support for the liver against
vitamins, and glucose; Group II received the
standard treatment only. Groups III and IV
were judged “serious,” with bilirubin levels
gave 16 subjects with chronic, aggressive LV
above 250 micromoles per liter. Group III
a relatively high intake of PC (2,050 mg per
received fortified PC and 580 mg daily of the
immunosuppressive drug prednisone (a drug
of clinical parameters improved, including
measures of the liver’s detoxification pathways
overactivation from LV); Group IV received
that metabolize amino acids and phenols, and
prednisone plus the standard treatment.
the authors concluded that PC was having a
PC had a clearly favorable effect in this
“normalizing” effect on the liver as a whole.
trial. Concerning the resolution of viral dam-
From their large open study reported in 1973,
age, both Group I subjects (less severe) and
over the course of which some subjects re-
Group III (more severe) had their liver tests
ceived PC for up to 5 years, Wallnoefer and
return to normal markedly faster than the cor-
Hanusch noted a success rate for chronic, ag-
responding groups that did not receive PC.
Subjects who did not receive PC were more
likely to relapse (10% in the less severe, 25%
ducted a double-blind trial in Japan in 1978,
in the severe), while no relapses occurred in
using 124 subjects with various LV.27,28 They
the PC groups. Upset stomach, jaundice, and
gave PC (1350 mg per day) to a group of 58
liver swelling, as well as the lab tests, all re-
subjects and placebo to 66 subjects, for twelve
solved faster in the groups treated with PC.
weeks. The PC group experienced significant
There was a trend towards lower occurrence
of the hepatitis B surface antigen (HBsAg) in
compared with the placebo group; those with
the PC groups as treatment progressed.
higher enzyme values to begin with appeared
to benefit the most. A subsequent blinded bi-
College, London did a double-blind trial in
opsy assessment after 6 months confirmed that
1982 on 30 subjects with progressing liver
in the PC subjects, the liver parenchymal tis-
Page 268 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
damage from chronic LV (hepatitis B virus,
with LV (hepatitis B virus).32 All the subjects
negative for HBsAg), as verified by biopsy.30
were chronically infected—they all had been
They randomly divided the subjects into two
virus carriers for at least 6 months. Seven had
groups of 15 each, kept them on the standard
viral antigens (HBeAg) which indicated a rela-
immunosuppressive therapy (prednisolone or
tively high degree of active infection. The
azathioprine), then gave one group PC (2,300
other 17 subjects had no viral antigens and had
mg per day) and the other placebo, for 1 year.
antibodies to the virus (anti-HBeAg), indicat-
At the end of this period, the group given PC
ing that they were in a stage of relative viral
had no clinical changes, while the placebo
inactivity. All subjects received 900 mg of
(control) group had worsened. Biopsies re-
fortified PC per day. After 4 months, the less
vealed significant improvement of the liver
severely affected, antibody-positive subgroup
structure in the PC group, versus no improve-
showed statistically significant improvements
ment for the controls. More of the PC sub-
in SGOT, SGPT, albumins, gamma-globulins,
jects reported improved well-being than did
the controls (62% versus 43%). In 3 of the 15
group that began the study with active virus
subjects given PC the viral infection was
had statistically significant improvements in
judged to be inactive at the end of the trial,
immune measures, suggestive of clinical ben-
while no subjects were judged inactive from
efit from PC. The effects of PC in this small
the placebo group. Thus in this small con-
and not well controlled trial were judged en-
trolled trial, PC halted and partly reversed
couraging, and might have been more dramatic
chronic LV damage, improved overall well-
had the daily intake been as high as in other
being, and “turned off” the virus in as many as
trials (a minimum 1350 mg of fortified PC,
rather than the 900 mg that was given).
sembled 60 subjects who were positive for
Controlled Trials with PC Against
hepatitis B virus (assessed as presence of
Severe Liver Damage
HBsAg) and who had acute LV liver damage,
and divided them into two groups.31 Within
acterized by extensive fibrosis, which effec-
tively stifles whole zones of the liver. Some-
double-blind basis the subjects were started on
times aggressive inflammatory changes are
either fortified PC (1350 mg) or placebo cap-
also present. This stage can be reached as a
sules. Lab tests were conducted frequently,
consequence of persistent alcohol intake, per-
and immune evaluations and clinical exams
sistent viral infection, or the unchecked toxic
were done at 30, 90, and 180 days (6 months,
effects of any of the many other agents that
can damage the liver. Given the severity of
the structural and functional damage to the
PC was significantly more improved than the
liver at this stage, lesser benefits are to be ex-
placebo group, with 50% being negative for
pected from PC supplementation than at ear-
HBsAg versus 25% for the controls (p<0.05).
lier stages. Yet still PC proved beneficial.
PC improved the rate of clearance of virus
antigen from the blood. The immune param-
controlled trial conducted in Prague, Czecho-
eters were not significantly different, though
slovakia, studied 61 subjects with moderately
liver enzyme tests showed trends favoring PC.
severe to severe functional breakdown of the
liver.33 The degree of advanced liver damage
(extensive fibrosis, inflammation, elevated en-
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 269
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
zymes) was assessed by biopsy and by a wide
HBsAg viral antigen, versus only 3 of 25 for
range of blood biochemical tests. Thirty-four
the placebo group. Such “seroconversion”
(34) subjects were given fortified PC (900 mg
indicated marked clinical improvement for
per day), and 27 subjects served as controls.
these fortunate subjects. A number of cell-
The trial ran for 4 months, with each patient
structural, biochemical, immunologic, and
serving as their own control for statistical
hematologic parameters were significantly
improved in the PC group as compared with
the end of the trial showed that except for the
group continued well past the end of the trial.
bilirubin values, all the other biochemical in-
dicators were significantly improved (p<0.01).
such severely affected subjects obtained bet-
These included the albumin/globulin ratio, al-
ter results by maintaining the subjects on com-
bumin, bromsulfalein (BSP) clearance, SGPT,
bined intravenous PC and oral supplementa-
and SGOT. The number of subjects positive
tion until substantial improvement had begun.
for HBsAg in the blood moved from 8 of 34
to 3 of 34 in the PC group; that of the controls
though not controlled, are worthy of note.
Wallnoefer and Hanusch in their pioneering
apparent in the PC group was not statistically
study administered PC both intravenously and
orally to 130 subjects with advanced, fibrotic
HBsAg-positive subjects in both groups from
liver damage.7 Once the clinical indicators
the beginning of the trial. The investigators
began returning to normal, they switched to
commented that fortified PC was the only in-
purely oral administration at relatively low
tervention they were aware of that seemed to
intakes (450-700 mg), which was continued
bring down viral antigen levels, and they urged
for months to years as necessary. PC produced
further investigation of this possible benefit
benefits for 17.5% of these subjects, as con-
improved tissue structure on biopsy. Using a
ducted a randomized, double-blind, placebo-
similar strategy, they achieved benefit for 35.3
controlled trial.34 They recruited 50 subjects,
percent of their subjects with chronic viral in-
all positive for HBsAg (hepatitis B virus anti-
fection of a kind that was positive for viral
gen) who had extremely severe liver damage
antigen and has an aggressive tendency to
as verified by biopsy and immunologic test-
progress to severe liver damage. Kuntz re-
ing. The test group was administered 1350
ported in 1989 on 10 subjects to whom he gave
mg of fortified PC, and the control group re-
PC intravenously at 2,800 mg per day.3 Im-
ceived a placebo. Both groups were followed
provements were seen as early as the seventh
for 1 year, with periodic sampling for lab as-
day, and at the end of the 28-day trial period 3
sessments, then at the end of the 12 months
subjects showed “dramatic, life-saving” im-
provement, 2 had “increasingly rapid improve-
ment,” 2 had gradual improvement, 2 had no
had experienced considerably greater benefit,
change; and 1 of the 10 subjects had died.
as assessed both from the structural biopsy
findings and from the lab findings (p <0.001).
subjects who had advanced liver damage for
which pharmaceutical treatments had failed.35
good to moderately good, versus 6 of 25 be-
Orally administered fortified PC (1350 mg
ing moderately improved in the placebo group.
daily) produced clinical improvement after 6
Six of the 25 in the PC group also lost the
Page 270 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
months, with favorable effects on the usual
peroxidative membrane damage to the liver
cell membranes, and the damage spreads to
neighboring zones within the tissue.
clinical trials discussed above concur with
findings from others36-40 to paint a clear pic-
membrane-based structure and functions of the
ture of PC as an effective and safe nutrient for
liver’s parenchymal cells. When orally admin-
liver damage of all degrees of severity.
istered to experimental animals, in quantitiesusually equivalent to 1-3 grams per day for
PC Benefits the Liver Primarily
the human, PC had the following liver-pro-
Through Cell Membranes
• Leakage of “indicator” enzymes from
liver against toxic attack can be attributed to
• Lipid peroxidation from free radical/
its important role in cell membranes. The
stituents most vulnerable to toxic attack, and
the diverse array of hepatotoxic substances
• Cell death, fibrosis, and fatty infil-
operates through common pathways: free radi-
tration of the liver tissue were diminished
cal or other oxidative attack that depletes an-
tioxidants, leading to oxidative overload and
subsequent peroxidative damage to the cell’s
membranes.4 The ultimate consequence is thedeath of the cell.
from PC is consistent with its functions at the
are partially unsaturated, and by being packed
cell membrane. PC is required for the struc-
tightly next to each other in the membrane they
tural integrity of all the body’s cell membrane
are highly vulnerable to oxidative attack from
systems, and is essential to their functional-
free radicals and other highly reactive, oxidant
ity.41-45 PC is crucial both for the internal
toxins. Under excessive or sustained attack,
membranes to do their housekeeping and spe-
cialized functions, and for the cell’s “master
graded (“peroxidized”), mainly through their
switch”—its outer membrane. The outer mem-
brane interfaces with both the external envi-
peroxidize, membrane continuity is inter-
ronment and the internal environment of the
rupted. Holes begin to develop in the cell’s
cell; PC supports the membrane receptors that
outer membrane, resulting in loss of control
“hear” these molecular messages and carry
over internal conditions. Enzymes and other
them across the membranes in both directions.
larger bio-molecules begin to leak out, homeo-
This outer membrane is also the cells’ reser-
stasis fails, and the death of the cell becomes
voir for the eicosanoids and other phospho-
lipid derivatives that act as outgoing vocabu-
lary, speaking the language of that cell to oth-
model similar to chemical attack: viral inva-
sion of the parenchymal cells initiates release
of pro-inflammatory, oxidizing substances.
cades of research are that PC is an important
Immune cells arrive in the area and begin re-
protective nutrient for the liver, primarily
leasing more oxidants via their “respiratory
through being a building block for cell mem-
burst.” These activities initiate cascades of
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 271
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
branes. PC is essential for the liver’s baseline
liver damage have established that PC can
homeostatic housekeeping functions, for the
liver’s recovery following toxic damage, and
not least to support the sophisticated liver
from PC is far more likely if the subject’s al-
metabolism that determines the individual’s
cohol consumption is ceased. The small cho-
level of health and freedom from disease.
line molecule is actually part of the headgroup
of the large PC molecule, but when free cho-
of the administered amount is absorbed over
line was added to the baboon diet it proved
24 hours),46 and PC represents a far more
toxic to the alcohol-damaged liver. Phosphati-
pleasant means for dietary choline repletion
dylcholine is a highly bioavailable form of
than choline itself. Lastly, even as the PC mol-
choline; it is also the most biologically sig-
ecule is efficiently absorbed, it also is an ex-
nificant and (for damaged livers, at least) the
bioavailability of nutrients with which it is co-
administered. Antioxidant nutrients and es-
tant nutrient for the liver, both because it is
pecially the flavonoids are likely to be better
the primary cell membrane building block and
absorbed in combination with PC,47 as are B
because the liver is so functionally dependent
vitamins, minerals, and numerous other nutri-
on its estimated 33,000 square meters of mem-
brane surface. Whether the liver has beendamaged by alcohol, by other toxic chemicals,
Conclusion:
by pharmaceuticals, or by viruses, dietary
supplementation with PC significantly speeds
studies conducted on thousands of human sub-
recovery. The clinical studies demonstrate that
jects to date, PC’s confirmed clinical benefits
dietary PC in sufficient amounts revitalizes
whole zones of cells in the recovering liver.
hance its remarkable usefulness as a dietary
supplement. PC is well documented as safe
to take, and seems fully compatible with phar-
• Accelerated restoration of subjects’
maceutical regimens and with other nutrients.
The PC molecule enhances the bioavailabilityof nutrients with which it is co-administered,
In the trials cited in this review, PC was
is highly bioavailable and represents a far bet-
very well tolerated at oral intakes that ranged
ter means for dietary choline repletion than
up to 4.6 grams per day, and was found to be
more effective the earlier it was administered.
Subjects who are started on PC after their liver
truly a “magic bullet” for alcoholic liver
is already severely damaged are more likely
disease, but its benefits against various
to benefit from higher oral intakes of PC (up
severities of liver damage and its proven safety
to or exceeding 4.6 grams per day). The most
indicate that for the liver it is a nutrient of
severe cases are likely to thrive with the help
of intravenous PC, administered in combina-tion with a high oral dose. References
Alberts B, Bray D, Lewis L, et al. Molecular
with baboons as a primate model of alcoholic
Page 272 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
Biology of The Cell. New York:Garland
parenteral nutrition patients. Gastroenterology
Jones AL. Anatomy of the normal liver. In:
Panoz MZ, Polson R, Johnson R, et al.
Zakim D, Boyer TD, eds. Hepatology: A
Activity of polyunsaturated phosphatidylcho-
Textbook of Liver Disease. Philadelphia:WB
line in HBsAg negative (autoimmune) chronic
active hepatitis and in acute alcoholic hepatitis. In: Gundermann K, Schumacher R, eds. 50thAnniversary of Phospholipid Research (EPL)
polyenylphosphatidylcholine in severe liver
International Symposium. Bingen/Rhein: wbn-
insufficiency. Med Welt 1989;40:1327-1329.
Lieber CS ; DeCarli LM ; Mak KM ; Attenua-
xenobiotic chemicals, foods, and drugs to free
tion of alcohol-induced hepatic fibrosis by
radical oxidants. In: Levine S, Kidd PM.
polyunsaturated lecithin. HepatologyAntioxidant Adaptation—Its Role in FreeRadical Pathology. San Leandro,California:Biocurrents;1985: 221-281.
Li J, Kim C, Leo MA, et al. Polyunsaturatedlecithin prevents acetaldehyde-mediated
Fausto N. Hepatic regeneration. In: Zakim D,
hepatic collagen accumulation by stimulating
Boyer TD, eds. Hepatology: A Textbook of
collagenase activity in cultured lipocytes.
Lieber CS, Robins SJ, Li J, et al. Phosphati-
phospholipids in the treatment of hepatic
cirrhosis in the baboon. Gastroenterology
disease. Med Monatsschrift 1973;27:131-136.
function tests and the objective evaluation of
lecithin and alcoholic liver disease: a magic
the patient with liver disease. In: Zakim D,
Boyer TD, eds. Hepatology: A Textbook ofLiver Disease. Philadelphia:WBSaunders;1996:791-833.
Hoyumpa AM, Schenker S. Drugs and theliver. In: Maddrey WC, ed. Gastroenterology
Sorrentino F, Diene G, Corvaja E, et al. Use of
and Hepatology: The Comprehensive Visual
polyunsaturated phosphatidylcholine (EPL) in
Reference. Philadelphia: Current Medicine;
association with vitamin B complex in liver
therapy. La Clinica Terapeutica1982;102:163-183.
Marpaung B, Tarigan P, Zein LH, et al. Tuberkulostatische Kombinations—therapie
Lieber CS. alcohol and the liver:1994 update.
aus INH, RMP und EMB. TherapiewocheGastroenterology 1994;106:1085-1105.
Lieber CS. Alcohol-induced liver disease. In:
Maddrey WC, ed. Gastroenterology and
icity of rifampicin and the effect thereon of
Hepatology: The Comprehensive Visual
“essential” choline phospholipids. Med WeltReference. Philadelphia: Current Medicine;
Hisanaga M, Utsumi S, Miyamoto S, et al.
Knuechel F. Double blind study in patients
Abnormality of liver function in patients
with alcohol-toxic fatty liver. Med Welt
treated with antiepileptic drug and a trial of
polyene phosphatidylcholine treatment for
Schuller Perez A, San Martin F.G. Controlled
these patients. Folia Psychiatr Neurol
study using multiply-unsaturated phosphatidyl-
choline in comparison with placebo in the case
Kuntz E, Neumann-Mangold P. Acute peroral
of alcoholic liver steatosis. Med Welt
trichloroethylene poisoning. Med Welt
Buchman AL, Dubin M, Jenden D, et al.
Esslinger F. Death cap mushroom poisoning:
Lecithin increases plasma free choline anddecreases hepatic steatosis in long-term total
Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996 Page 273
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
report of clinical experience. Med Welt
acute, life-threatening liver failure conditions.
Frosch B, Wagener H. Therapy of hepatitis
den Einfluss therapeutischer Teilkoerper-
epidemica. Fortschritte Med 1963;81:725-7.
bestrahlungen auf die Leberfunktion und die
Kautsch E. Comparison of therapy in acute
Schutzwirkung essentieller Phospholipide.
hepatitis epidemica. Med KlinischeStrahlentherapie 1964;123:438-450. [In
Rottini E, Bazzanella F, Marri DG, et al.
Mueting D, Dohn P, Reikowski J. Effect of
Therapy of different types of liver insuffi-
high doses of essential phospholipids adminis-
ciency using “Essential” phospholipids. Med
tered intravenously and perorally on metabo-
lism of albumin and fats and on enzymatic
activity of chronically ill liver patients.
therapy of hepatitis infectiosa. Munch MedVerhandlungen der Deutsche Gesselchaft furInnere Medizin 1972;17:1389-1392.
27. Hirayama C, Okamura M, Tanikawa K, et al. The
transport. Can J Biochem 1980; 58, 1091-
clinical effect of polyene phosphatidylcholine
in chronic hepatitis in a double-blind test. Rinsho to kenkyu 1978;55:194-198.
Hirata F, Axelrod J. Phospholipid methylationand biological signal transmission. Science
28. Yano M, Koga M, Shirahama S, et al. Blind
assessment of liver biopsy findings in chronichepatitis: drug efficacy trial of polyene
phosphatidylcholine. Shindan to chiryo
composition and cellular function. J Lipid Res
29. Kosina F, Budka K, Kolouch Z, et al. Essential
Shinitzky M. Membrane fluidity and receptor
cholinephospholipids in the treatment of viral
function. In: Kates M, Manson LA, eds.
hepatitis. Cas Lek Ces 1981;120:957-960. Membrane Fluidity. New York:Plenum Press;1984.
30. Jenkins PJ, Portmann BP, Eddleston ALWF, et al.
Use of polyunsaturated phosphatidylcholine in
atherosclerosis—the importance of dietary
results of prospective double-blind controlled
fatty acid balance. Alternative Medicine
31. Visco G. Polyunsaturated phosphatidylcholine
Fox JM, et al. Pharmacokinetics of orally
ingested phosphatidylcholine. In: Barbeau A,
treatment of acute viral hepatitis B. La Clinica
et al, eds. Nutrition and the Brain, Volume 5. Terapeutica 1985;114:183-188.
32. Hantak I, Boca M, Miculecky M, et al. Essential
Buzzelli G, Moscarella S, Giusti A, et al. A
phospholipids in the treatment of chronic
pilot study on the liver protective effect of
infection with the hepatitis B virus. Vnitrni
1016) in chronic active hepatitis. Intl J ClinPharmacol Ther Toxicol 1993; 31:456-460.
33. Fassati P, Horesji J, Fassati M, et al. The effect of
choline phospholipids on HBsAg and selected
Lieber CS, Leo MA, Mak KM, et al. Choline
biochemistry tests in cirrhosis of the liver. Cas
fails to prevent liver fibrosis in ethanol-fed
baboons but causes toxicity. Hepatology1985; 5:561-572.
34. Ilic V, Begic-Janev A. Therapy for HBsAg-
positive chronically active hepatitis. Effect of“essential” phospholipids. Med Welt1991;85:523-525.
35. Kalab M, Cervinka J. Essential phospholipids in
the treatment of cirrhosis of the liver. Cas LekCes 1983;122:266-269. [In Slovak, withEnglish summary]
36. Docker O. Therapy of chronic liver diseases and
Page 274 Alternative Medicine Review ◆ Volume 1, Number 4 ◆ 1996
Copyright1996 Thorne Research, Inc. All Rights Reserved. No Reprint Without Written Permission
25 APRILE: sul palco di Piazza Napoleone il progetto musicale "Rezophonic" 25 APRILE: IL PROGETTO REZOPHONIC SUL PALCO DI PIAZZA GRANDE Torna l’atteso appuntamento musicale per l’anniversario della Liberazione. In scena artisti di Bluvertigo, Le Vibrazioni, Movida, Prozac + e tanti altri Lucca - Il progetto “Rezophonic” è un’innovativa proposta discografica e all
Co-Occurring Disorder-Related Quick Facts: NICOTINE Nicotine: Nicotine, a component of tobacco, is the primary reason that tobacco is addictive, although cigarette smoke contains many other dangerous chemicals, including tar, carbon monoxide, acetaldehyde, nitrosamines, and more.1 In 1988, the Surgeon General concluded that cigarettes and other forms of tobacco (i.e., cigars, pipes
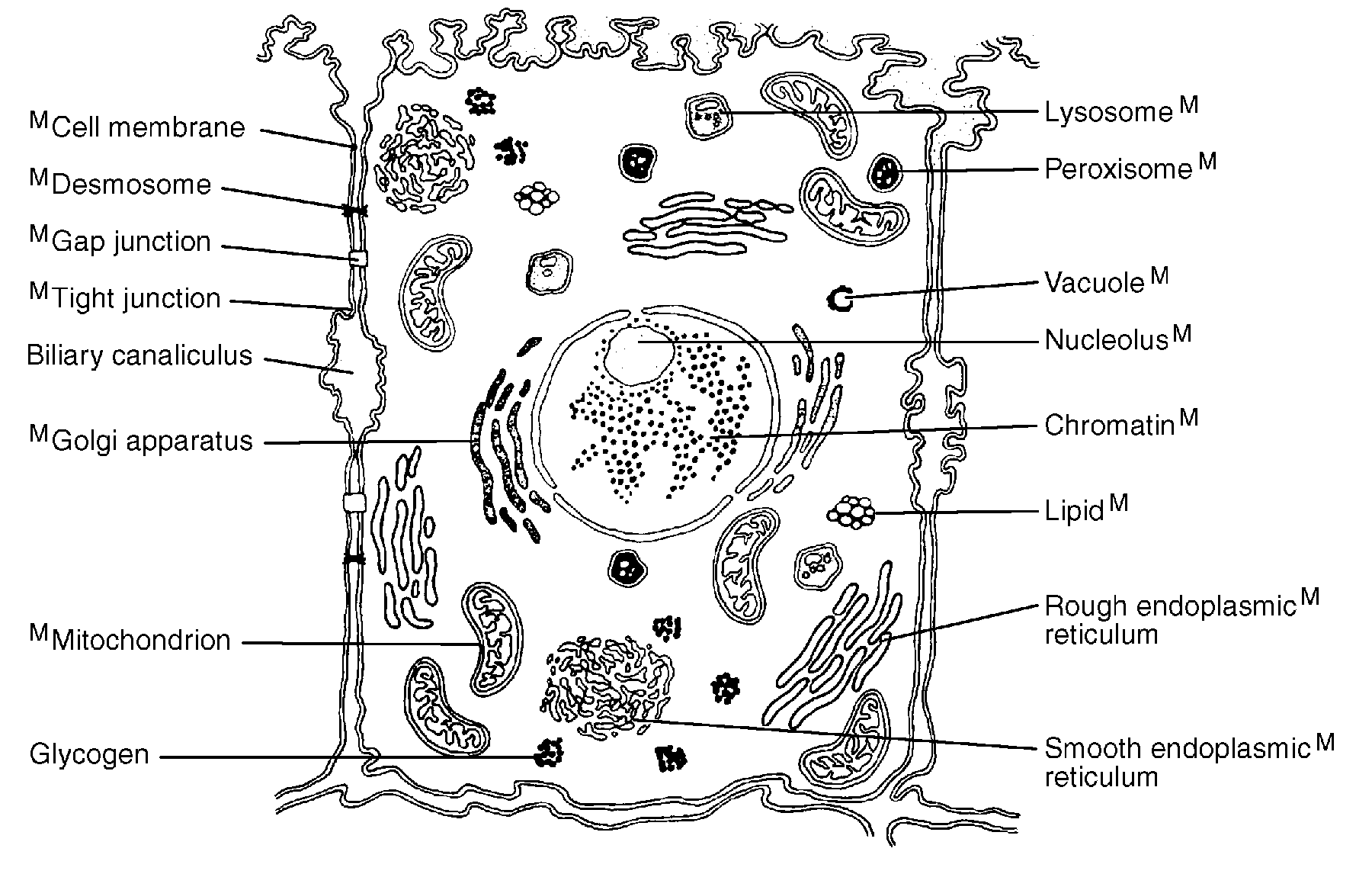 Figure 2. Schematic of the liver parenchymal cell, showing the internal functional
Figure 2. Schematic of the liver parenchymal cell, showing the internal functional