He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Doi:10.1016/j.ajo.2006.04.064
arrest in the G1-phase in a dose-dependent manner, while
body removal, and intraocular lens (IOL) implant. Post-
MMC inhibits DNA synthesis, which results in cell cycle
operatively, IOL was imaged with Pentacam Scheimpflug
arrest in the S CSA also inhibits angiogenesis in
imaging. RESULTS: Scheimpflug imaging allowed us to confirm the
Our cases indicate that adjunctive treatment with top-
presence and exact location of ILFB and its relation to
ical CSA (0.05%) and MMC (0.01%) prevents tumor
the intact posterior capsule as well as the postoperative
recurrence and provides excellent ocular surface healing in
IOL positioning. This helped in better planning of man-
patients who have tumor-positive margins following surgi-
agement of traumatic cataract with ILFB. CONCLUSIONS: Pentacam is a potential tool for accurate localization of foreign bodies lodged in the lens and pro- vides an objective basis for better patient counseling and surgical planning. (Am J Ophthalmol 2006;142:
1. Tunc M, Char DH, Crawford B, Miller T. Intraepithelial and
675– 676. 2006 by Elsevier Inc. All rights reserved.)
invasive squamous cell carcinoma of the conjunctiva: analysisof 60 cases. Br J Ophthalmol 1999;83:98 –103.
2. Dudney BW, Malecha MA. Limbal stem cell deficiency
METALLIC INTRALENTICULAR FOREIGN BODIES (ILFB)
following topical mitomycin C treatment of conjunctival-
after penetrating eye injuries are not common. We
corneal intraepithelial neoplasia. Am J Ophthalmol 2004;137:
describe a case of traumatic cataract with endophthalmitis
and retained metallic ILFB. Scheimpflug Imaging System
3. Benelli U, Ross JR, Nardi M, Klinworth GK. Corneal neovas-
(Pentacam 70700: Oculus, Wetzlar, Germany) helped in
cularization induced by xenografts or chemical cautery. Inhi-
localizing the ILFB, defining its relation with the posterior
bition by cyclosporin A. Invest Ophthalmol Vis Sci 1997;38:
capsule and reconstructing the projectile’s trajectory for
medico-legal importance. It captures a light slice through
4. Seki Y, Toba K, Fuse I, et al. In vitro effect of cyclosporin A,
the anterior chamber and crystalline lens to provide a quick,
mitomycin C, and prednisolone on cell kinetics in cultured
accurate, and objective documentation of the anterior
human umbilical vein endothelial cells. Thromb Res 2005;
segment that is convenient for the ophthalmologist. It’s
resolution is superior to roentgenograms, computed tomog-
5. Macarez R, Bossis S, Robinet A, Le Callonnec A, Charlin JF,
Colin J. Conjunctival epithelial neoplasias in organ transplant
patients receiving cyclosporine therapy. Cornea 1999;18:495–
A 35-year-old male presented with penetrating injury to
left eye (LE) with a projectile iron particle. Best-corrected
6. Tang-Liu DD, Acheampong A. Ocular pharmacokinetics and
visual acuity (BCVA) in LE was hand motion close to face.
safety of cyclosporine, a novel topical treatment for dry eye.
Slit-lamp biomicroscopy revealed corneal edema, 3-mm hy-
Clin Pharmacokinet 2005;44:247–261.
popyon, and fibrinous exudates in the pupillary area Left) suggestive of traumatic endophthalmitis, which wasmanaged with intravitreal vancomycin (1 mg/0.1 ml) and
Role of Scheimpflug Imaging
ceftazidime (2.25 mg/0.1 ml). The right eye was normal. in Traumatic Intralenticular
Within 48 hours, BCVA improved to count fingers threefeet away, corneal edema subsided, hypopyon reduced to
Foreign Body
0.5 mm, and fibrinous exudates retracted. Slit-lamp exam-
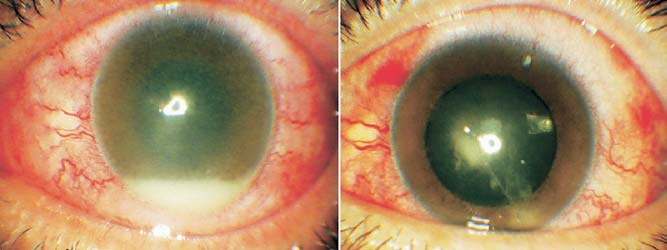
Satinder Pal Singh Grewal, MD, Rajeev Jain, MD, Rajeev Gupta, MD, and Dilraj Grewal, MBBS PURPOSE: The role of Pentacam Scheimpflug imaging in evaluation of penetrating eye injury and intralenticular foreign body (ILFB). DESIGN: Interventional case report. METHODS: A 35-year-old male presented to our clinical practice with penetrating eye injury and endophthalmitis. FIGURE 1. Intralenticular foreign body (ILFB) and endoph- Scheimpflug imaging helped localize the intralenticular thalmitis. (Left) Anterior segment image showing endophthalmitis foreign body (ILFB). It confirmed the posterior capsule on the day of presentation. Best-corrected visual acuity (BCVA) to be intact. He underwent phacoemulsification, foreign was hand motion close to face. (Right) Two days later, endoph- thalmitis has resolved and exudates are localized. The traumatic
Accepted for publication Apr 28, 2006. cataract is evident at the site of capsular tear. BCVA improved to
From the Grewal Eye Institute, Madhya Marg, Chandigarh, India. count fingers three feet. The metallic ILFB is visible in the
Inquiries to Satinder Pal Singh Grewal, MD, Grewal Eye Institute,
temporal clear part of the lens.
S.C.O. 166-169, Sector 9-c, Madhya Marg, Chandigarh, India 160009;e-mail: [email protected]
phacoemulsification (stop and chop), ILFB removal, andintraocular lens (IOLs) implantation (AMO AR 40e) werecarried out as a single procedure.
Four weeks post surgery, patient’s BCVA was 20/30 in
the left eye. Slit-lamp biomicroscopy showed normal pu-pillary reactions, a well-centered in-the-bag IOL Left). Indirect ophthalmoscopy revealed a clear media. FIGURE 2. Pentacam Scheimpflug image of the anterior segment.
Scheimpflug images revealed a well-centered IOL and an
(Left) Intralenticular foreign body (ILFB) and the corneal wound of entry are clearly visible (thin arrow). The trajectory projected
ILFB can be associated with cataract, intraocular
from these two revealed the foreign body as coming from the right
inflammation, endophthalmitis, or siderosis Poste-
side of the patient at an angle of 43.5° to the visual axis. ILFB
rior capsular rent may be coexistent in 25% of cases with
measured 750 and is located 1510 from the anterior capsule
ILFB and has a major implication on surgical planning. (short thick arrow). The posterior capsule is intact. (Right) The three-dimensional virtual reconstruction of the lens delineates the relative position of the ILFB (arrow).
there have been reports of ILFB lodged for a prolongedtime without
Pentacam helps ophthalmologists to accurately localize
and map the trajectory of foreign bodies lodged in anteriorsegment allowing better decisions for management.
1. Lee LR, Briner AM. Intralenticular metallic foreign body.
Aust N Z J Ophthalmol 1996;24:361–363.
2. Arora R, Sanga L, Kumar M, Taneja M. Intralenticular foreign
bodies: report of eight cases and review of management. Indian
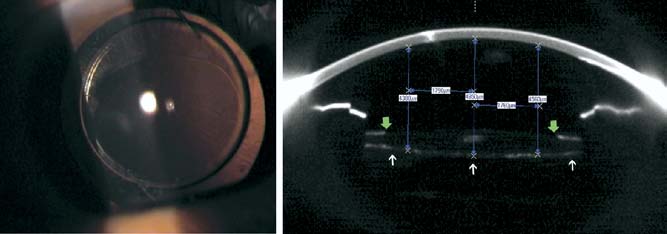
FIGURE 3. Postoperative slit-lamp and Scheimpflug images at four weeks. (Left) A retro-illumination slit-lamp image shows a
3. Kumar A, Kumar V, Dapling RB. Traumatic cataract and
well-centered intraocular lens (IOLs). Best-corrected visual
intralenticular foreign body. Clin Exp Ophthalmol 2005;33:
acuity (BCVA) is 20/30. (Right) The Scheimpflug image on Pentacam showing margins of anterior capsulorrhexis (green
4. Scala FED, Kamal A. Intralenticular foreign body: a D-Day
arrows), intact posterior capsule (white arrows), and a well-
reminder. Clin Exp Ophthalmol 2005;33:659 – 660. centered IOL implant with a minimum tilt of 160 (see blue line grid markings). Closure of Persistent Cyclodialysis Cleft Using the Haptics of the
ination revealed a metallic foreign body lodged in uppertemporal quadrant of the lens with localized traumatic
Intraocular Lens
cataract at the wound of entry Right). Media
Pierre G. Mardelli, MD
clarity was Grade III on indirect ophthalmoscopy. How-ever, the integrity of the posterior capsule could not be
PURPOSE: To evaluate a technique for ab-interno repair of cyclodialysis cleft in conjunction with placement of an
Scheimpflug imaging Left) revealed the cor-
intraocular lens (IOL).
neal wound of entry and intralenticular track of foreign
DESIGN: Interventional case reports.
body. The trajectory projected from these two revealed the
METHODS: SETTING: Clinical practice. PATIENTS: Two eyes
foreign body as coming from the right side of the patient at
of two patients, one phakic and one aphakic, present
an angle of 43.5° to the visual axis. A highly reflective
with hypotony secondary to traumatic cyclodialysis cleft.
ILFB (100% on lens densitometry scale), distinct from the
INTERVENTION: A single piece all-polymethyl methacry-
site of traumatic cataract, was best localized at 2 o’clock
late intraocular lens (PMMA IOL) 13.5 mm in diameter
(segment 197° Ϫ 17°). The ILFB was 750 in the maxi-
was placed in the ciliary sulcus with the haptics placed in
mum dimension. It was 1510 posterior to the anterior
the area of cyclodialysis cleft during cataract surgery and
capsule and 610 away from the intact posterior capsule. The three dimensional reconstruction of the patient’s
Accepted for publication May 10, 2006.
preoperative images showed the relative depth of foreign
From the Glaucoma Service, Eye and Ear Hospital, and Department of
body and its relation to the posterior capsule
Ophthalmology, Hotel Dieu de France, Saint Joseph University, Beirut,Lebanon.
Right). Scheimpflug images helped to plan phacoemulsifi-
Inquiries to Pierre G. Mardelli, MD, P. O. Box 113-5786, Beirut,
cation, removal of ILFB, and patient counseling. Unimanual
Alzheimer’s Imaging Consortium IC-P: Poster PresentationsBackground: Rosiglitazone, a peroxisome proliferator-activated receptorcopy. Because of their high iron content, plaques typically appear as hypo-[gamma] (PPAR[gamma]) agonist, has an anti-inflammatory effect in theintense spots on T2-weighted scans. One of the challenges in imagingbrain, decreasing interleukin-1[beta] concentration
BIOGRAPHICAL SKETCH EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, and include postdoctoral University of Agricultural Sciences, Bangalore, India University of Agricultural Sciences, Bangalore, India University of Minnesota, Saint Paul, MN Ph.D. Baylor College of Medicine, Houston, TX Post-doc A. Positions, professional service
 arrest in the G1-phase in a dose-dependent manner, while
body removal, and intraocular lens (IOL) implant. Post-
arrest in the G1-phase in a dose-dependent manner, while
body removal, and intraocular lens (IOL) implant. Post-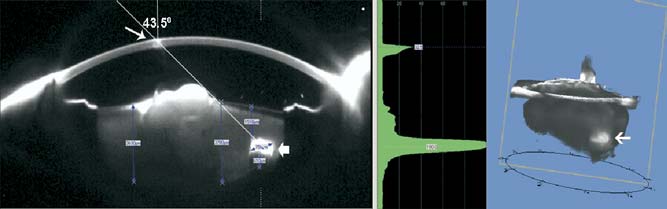
 phacoemulsification (stop and chop), ILFB removal, andintraocular lens (IOLs) implantation (AMO AR 40e) werecarried out as a single procedure.
phacoemulsification (stop and chop), ILFB removal, andintraocular lens (IOLs) implantation (AMO AR 40e) werecarried out as a single procedure.