He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Institutogalenico.pt
Endovenous obliteration versus conventionalstripping operation in the treatment of primaryvaricose veins: A randomized controlled trial withcomparison of the costs
Tero Rautio, MD,a Arto Ohinmaa, PhD,b Jukka Pera¨la¨, MD, PhD,c Pasi Ohtonen, MSc,a Timo Heikkinen, MD, PhD,a Heikki Wiik, MD,a Pasi Karjalainen, MD,d Kari Haukipuro, MD, PhD,a and Tatu Juvonen, MD, PhD,a Oulu, Finland; and Edmonton, Canada Objective: The aim of this randomized study was to compare a new method of endovenous saphenous vein obliteration (Closure System, VNUS Medical Technologies, Inc, Sunnyvale, Calif) with the conventional stripping operation in terms of short-term recovery and costs. Methods: Twenty-eight selected patients for operative treatment of primary greater saphenous vein tributary varicose veins were randomly assigned to endovenous obliteration (n ؍ 15) or stripping operation (n ؍ 13). Postoperative pain was daily assessed during the 1st week and on the 14th postoperative day. The length of sick leave was determined. The RAND-36 health survey was used to assess the patient health-related quality of life. The patient conditions were controlled 7 to 8 weeks after surgery, and patients underwent examination with duplex ultrasonography. The comparison of costs included both direct medical costs and costs resulting from lost of productivity of the patients. Costs that were similar in the study groups were not considered in the analysis. Results: All operations were successful, and the complication rates were similar in the two groups. Postoperative average pain was significantly less severe in the endovenous obliteration group as compared with the stripping group (at rest: 0.7, standard deviation [SD] 0.5, versus 1.7, SD 1.3, P ؍ .017; on standing: 1.3, SD 0.7, versus 2.6, SD 1.9, P ؍ .026; on walking: 1.8, SD 0.8, versus 3.0, SD 1.8, P ؍ .036; with t test). The sick leaves were significantly shorter in the endovenous obliteration group (6.5 days, SD 3.3 days, versus 15.6 days, SD 6.0 days; 95% CI, 5.4 to 12.9; P < .001, with t test). Physical function was also restored faster in the endovenous obliteration group. The estimated annual investment costs of the closure operation were US $3360. The other direct medical costs of the Closure operation were about $850, and those of the conventional treatment were $360. With inclusion of the value of the lost working days, the Closure treatment was cost-saving for society, and when 40% of the patients are retired (or 60% of the productivity loss was included), the Closure procedure became cost-saving at a level of 43 operations per year. Conclusion: Endovenous obliteration may offer advantages over the conventional stripping operation in terms of reduced postoperative pain, shorter sick leaves, and faster return to normal activities, and it appears to be cost-saving for society, especially among employed patients. Because the procedure is also associated with shorter convalescence, this new method may potentially replace conventional varicose vein surgery. (J Vasc Surg 2002;35:958-65.)
In the Western countries, operations on varicose veins
the procedure is associated with significant surgical mor-
are among the most common surgical procedures. In Fin-
land, approximately 220 varicose vein operations per
Recurrence is common after primary greater saphenous
100,000 inhabitants are performed each year.1 The strip-
varicose vein surgery. Rates as high as 40% at 5 years have
ping operation is a relatively inexpensive day surgery pro-
been reported, and approximately 20% of varicose vein
cedure that needs no special instrumentation. Varicose vein
operations are done for recurrent veins.3,4 Furthermore,
surgery is regarded as a safe and minor procedure; indeed,
reoperations also result in marked losses of productivity. InFinland, the average sick leave time after a stripping oper-ation has been 4 weeks (Statistics of the Finnish National
From the Departments of Surgery,a Radiology,c and Anesthesiology,d Oulu
Pension Office 1997). Therefore, the economic conse-
University Hospital; and the Department of Public Health Sciences,University of Alberta.b
quences of varicose vein surgery and its numerous recur-
Supported by a grant from the University of Oulu, Finland.
rences for healthcare and whole society are high.
This issue has led to the development of mini-invasive
Additional material for this article may be found online at www.mosby.
techniques to replace the traditional procedure of stripping
Reprint requests: Tero Rautio, MD, Department of Surgery, Oulu Univer-
of the greater saphenous vein (GSV). Endovenous obliter-
sity Hospital, Kajaanintie 50, SF-90230, Finland (e-mail: tero.rautio@
ation (Closure System, VNUS Medical Technologies, Inc,
Sunnyvale, Calif) is a new method in which a catheter is
Copyright 2002 by The Society for Vascular Surgery and The American
inserted percutaneously to treat the GSV insufficiency.5,6
The operative costs of this new technique are higher be-
0741-5214/2002/$35.00 ϩ 0 24/1/123096 doi:10.1067/mva.2002.123096
cause of the purchasing price of the device and the dispos-
JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
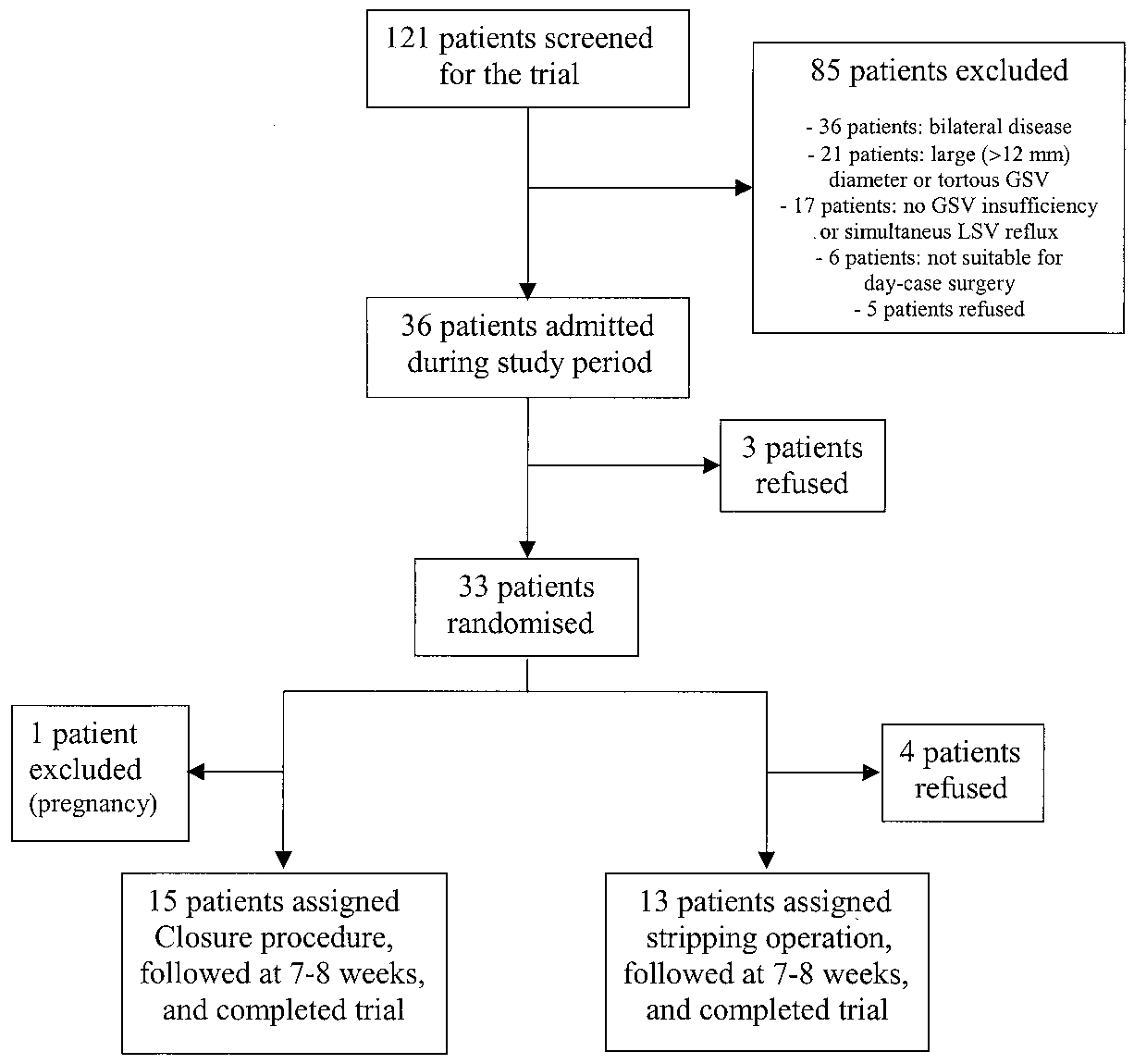
Rautio et al 959 Fig 1. Trial profile. GSV, Greater saphenous vein; LSV, lesser saphenous vein.
able catheters. On the other hand, the procedure is less
ultrasonography. Veins with a curve greater than 90 de-
invasive and may, therefore, result in shorter convalescence
grees were considered to be unsuitable for endovenous
and ability to resume work sooner, thus reducing the costs
treatment because of obvious problems of passage of the
of lost productivity. The purpose of this study was to
fairly rigid catheter in abrupt curves. The diameter of the
compare endovenous saphenous vein obliteration with
vein was measured with the patient in a semisupine posi-
conventional stripping operation in a randomized fashion
tion. The clinical severity of the varicose disease was graded
and to evaluate the outcome in terms of postoperative pain,
according to the clinical, etiologic, anatomic, and patho-
sick leave, health-related quality of life, and cost.
physiologic (CEAP) scoring system and its modifications,the venous clinical severity score, the venous segmental
PATIENTS AND METHODS
disease score, and the venous disability score.7,8
The study protocol was approved by the Ethical Com-
The trial profile is summarized in Fig 1. Originally, 36
mittee of the Medical Faculty of the University of Oulu,
patients with isolated GSV reflux were enrolled. Three of
and the study was performed according to the provisions of
the selected patients discontinued the study because of an
unsuitable schedule. The remaining 33 patients were ran-
Patient selection. For patient enrollment, 121 con-
domized with the sealed envelope method.
secutive patients scheduled for surgical treatment of pri-
After the randomization, however, another four pa-
mary varicose veins at the Department of Surgery, Oulu
tients withdrew because of disappointment with assign-
University Hospital, underwent examination with color
ment to the stripping group. Another patient withdrew
duplex ultrasonography. Screening was done between Jan-
after the randomization because of pregnancy.
uary and June 2000 (Appendix A, online only). A Valsalva’s
Procedures. All the procedures were performed with
maneuver–induced reversal of blood flow lasting for at least
standardized balanced general anesthesia. The endovenous
2 seconds was considered a sign of clinically significant
obliterations were performed by a surgeon (T.R.) in collab-
reflux. Patients suitable for day-case surgery with symptom-
oration with a radiologist (J.P.). The investigators had
atic, previously untreated, and uncomplicated GSV tribu-
performed more than 30 VNUS Closure procedures before
tary varicosis and isolated unilateral saphenophemoral junc-
the start of the study. All the stripping operations also were
tion (SFJ) and GSV trunk insufficiency were eligible for the
performed by the same experienced general surgeon (T.R.)
study. Patients with coagulopathy or multiple, tortuous,
with the same team and in the same operating room during
and large-diameter (Ͼ12 mm) GSV trunks were excluded.
November 2000. In addition, local phlebectomy with Oe-
The tortuosity and diameter of the vein were assessed with
sch hooks (Salzmann Medico, St Gallen, Switzerland) and,
960 Rautio et al
in case of teleangiectasis, microsclerotherapy (Glicerina,
leave was routinely prescribed for 5 days and continued for
Laboratorio Terapeutico MR srl, Florence, Italy) were per-
as much as 2 weeks if necessary. If disability lasted for more
than 2 weeks, the patient was scheduled for a control visit at
The endovenous obliteration procedure was performed
with the VNUS Closure system, for which the technical
The patients underwent reexamination after 7 to 8
details have been described previously.6,7 The catheter with
weeks with color duplex ultrasonography. The postopera-
sheathed electrodes was inserted percutaneously with ultra-
tive CEAP scores were recorded. The patients also were
sound scan guidance into the GSV at the ankle level
asked whether they were satisfied with the treatment and
through a vascular sheath of 5F or 8F. Subsequently, the
how long a sick leave was necessary in their own opinion.
catheter was passed up to the SFJ, and its correct position
The outcome measures were the duration of sick leave,
was controlled with intraoperative ultrasound scanning.
pain, health-related quality of life, and satisfaction with the
Subcutaneous saline solution was infiltrated between the
proximal GSV and the skin. The lower limb was elevated,
Calculation of costs. For a cost analysis, the costs
and an elastic compression wrap was applied from the toes
were divided into direct medical costs and indirect costs.
to the groin for exsanguination of the entire GSV. Supple-
The direct medical costs consisted of fixed and variable costs
mental manual compression was used at the groin region.
as seen in Table I. Indirect costs consisted of the value of lost
The electrodes of the catheter were unsheathed, and the
wall contact of the electrodes was tested with measurement
Costs that could be assumed to be the same in both
of the impedance of the catheter. Heparinized saline solu-
procedures (eg, administrative work, energy, overhead)
tion was administered through the central lumen to rinse
were excluded. Operating times (“skin-to-skin”) and oper-
the electrodes and to avoid thrombus formation. No ordi-
ating room and recovery room times were measured in
nary thrombosis prophylaxis was used. After the activation
minutes and valued on the basis of the average salary
of the treatment circuit, the wall temperature was allowed
brackets and figures drawn from the hospital accounting
to equilibrate at 85° C for 15 seconds. The catheter then
system. Anesthesia and recovery room costs were estimated
was slowly (ca 3 cm/min) withdrawn, with the temperature
to be US $72 in both methods. Two specialists were
within Ϯ3° C of the set temperature. The entire length of
involved in the VNUS operation compared with one in the
the femoral segment of the GSV thus was treated. To avoid
conventional alternative. The hourly salary of a specialist
damage to the saphenous nerve, the treatment was limited
was $32. Investment costs included only the cost of the
to the area above the medial condyle of the tibia. Immedi-
generator and were allocated to 5 years with a 5% social
ately after the treatment, the treated segment was evaluated
discount rate. The basic instrumentation was the same in
with color Doppler ultrasound scan to ensure proper oc-
both operations. The VNUS Closure specific costs further
clusion of the vein. This evaluation also allowed the option
included the price of the catheter and the rent of the
of retreatment of the unoccluded segment immediately.
ultrasound scan equipment. The other costs of day surgery
The length of the treated GSV segment and the pullout
were assumed to be the same. The postoperative costs
At the beginning of the stripping operation, the groin
included the additional follow-up visits and telephone con-
was dissected to fully expose the SFJ. The side branches of
sultations needed to lengthen sick leaves. The patient med-
the GSV at the SFJ were divided and ligated. After local
ical costs were assumed to be the same, with the exception
phlebectomy, the GSV was stripped from just below the
of the analgesics used during the first 2 weeks and the travel
knee to the groin with the conventional flexible and dispos-
costs as a result of the follow-up visits. The units and the
able Venostrip (Aesculap AG & CO, KG, Tuttlingen, Ger-
unit values of the cost factors and the sum totals are shown
many) with a 9-mm olive. The calf and groin incisions were
in Table I. The indirect costs were calculated as costs caused
sutured with 5/0 nonabsorbable interrupted sutures.
by lost productivity because of sick leave. The value of the
Postoperative care and follow-up examination.
lost workdays was assessed on the basis of the average wage
Postoperative compression of the treated leg was standard-
level in Finland in the year 20009 plus 50% nonwage costs
ized. Knee and groin length antiembolism stockings were
for social security and other worker-based costs. A 5-day
applied immediately after the treatment and kept for 7 days.
work week was used in the calculation of indirect costs.
No limitations were placed on mobilization, and the pa-
Statistical analysis. The serial measurements were
tients were encouraged to walk as soon as possible.
summarized with calculation of the average score over the
The patients recorded postoperative pain at rest, on
study period for each patient. The change from the baseline
standing, and on walking with a visual analogue scale
health-related quality of life scores to those recorded at 1
(range, 0 to 10) on a daily basis during the 1st week and on
week and 4 weeks after surgery was determined, and the
the 14th postoperative day. The short-term RAND-36
other intergroup comparisons were made with Student t
generic health-related quality of life questionnaire (validat-
test (TT) or with the Mann-Whitney U test as appropriate.
ed for Finland) was used to measure health status before the
The categoric values were analyzed with the 2 or Fisher
procedure and 1 and 4 weeks after surgery. The patients
exact test. Kendall rank correlation coefficient () and co-
also were asked to record the need and use of oral ibuprofen
efficient of determination (2) were calculated (Appendix
(the number of 600-mg tablets) or other analgesics. A sick
JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 961 Table I. Costs of VNUS Closure and conventional surgery in treatment of primary varicose veins (US dollars*)
Sensitivity analysis was done to estimate the effects of
Table II. Patient characteristics
the changes in the main background variables. The influ-ence of indirect costs was tested with 50% of the estimated
costs. The influence of the retired patients on the indirect
costs was tested with the assumption that 25% or 40% of thepatients were retired. The scenario with one specialist per-
forming the whole operation and no discounting of invest-
ment costs also was analyzed. Two-way sensitivity analysis
was performed, with the assumption that one specialist
performed the operation and that the indirect costs ac-
counted for 50%, 60%, or 75% of the estimated costs. The
influence of the possible higher investment costs in the
United States were tested with $18,000 as a cost for the
generator and $446 for the catheter (values from US ex-
Twenty-eight patients were allocated into the treat-
EOG, endovenous obliteration group; SOG, stripping operation group;
ment groups and completed the study. Fifteen patients
GSV, greater saphenous vein; VCSS, venous clinical severity score; VSDS,
were in the endovenous obliteration group, and 13 patients
venous segmental disease score; VSD, venous disability score.6
were in the stripping group (Fig 1).
The basic characteristics of the patients were similar in
both groups, with the exception of the higher mean age in
and operating room time (115 minutes, SD 18.3, versus 99
the stripping group (P ϭ .045, with TT; Table II). One
minutes, SD 12.9, P ϭ .01) were significantly longer in the
patient retired after randomization but was not withdrawn
endovenous obliteration group. These times are used in
the cost analysis presented in Table I. The differences in the
The procedures were performed on a day surgery basis.
recovery room times (obliteration: 227 minutes, SD 57.6;
As evidence of successful standardization of general anes-
versus stripping: 198 minutes, SD 40.7; P ϭ .16) were not
thesia, no significant differences were seen in the bispectral
index, sevoflurane minimum alveolar concentration, imme-
The mean follow-up time was 50 days in both groups.
diate recovery from anesthesia, or home readiness. Two
In all cases, endovenous obliteration was successfully per-
patients (one from each group) had to stay in the hospital
formed with no duplex scan– detectable flow in the treated
overnight because of social reasons.
GSV segments. Consequently, the postoperative venous
The mean operation time (75 minutes, standard devi-
segmental disease score fell from 1 to 0 in all patients of this
ation [SD] 16.6, versus 57 minutes, SD 11.0, P ϭ .003)
group. One patient in the stripping group had reflux in an
962 Rautio et al Table III. Postoperative complications after closure procedure and stripping operation for primary varicose veins
accessory branch of GSV, which resulted in a score of 1 aftersurgery. The average decrease of the venous clinical severityscore was 5.1 (SD, 1.5) in the endovenous obliterationgroup and 4.4 (SD, 1.1) in the stripping group (P ϭ .19,with TT). The postoperative venous disability score was 0in all but two patients (one from each group), who occa-sionally needed compression stockings while working.
Intraoperative complications consisted of a painful
groin hematoma (stripping group) and three small second-degree thermal skin injuries (endovenous obliterationgroup). The burns did not need specific treatment andhealed completely. These three patients, however, had ten-derness and induration over the course of the treated GSVsegment. In one of these cases, thermal burn scar wasnoticed at the time of follow-up visit and was considered asa late complication (Table III). Saphenous nerve paresthesis,defined as numbness or dysesthesia, which was limited tothe thigh, developed after two endovenous procedures andthree stripping operations. On the whole, minor postoper-ative complications were common in both groups, withseven in the endovenous obliteration group and seven inthe stripping operation group (Table III). None of thecomplications caused any need for treatment or resulted inincreased costs.
The average visual analogue scale pain scores at rest, on
standing, and on walking were significantly lower in theendovenous obliteration group than in the stripping group
Fig 2. Median pain scores with 25th and 75th percentiles at rest
(rest: 0.7, SD 0.5, versus 1.7, SD 1.3, P ϭ .017; standing:
and on standing and walking. (Daily P values were calculated with
1.3, SD 0.7, versus 2.6, SD 1.9, P ϭ .026; walking: 1.8, SD
Mann-Whitney U test). EOG, Endovenous obliteration group;
0.8, versus 3.0, SD 1.8, P ϭ .036; with TT). The differ-
SOG, stripping operation group; VAS, visual analogue scale.
ences were especially clear from the 5th to the 14th post-operative day (Fig 2). Patients in the endovenous oblitera-
The changes in the health-related quality of life param-
tion group also needed less analgesics than those in the
eters are shown in Table IV. Physical function was restored
stripping group (average daily number of 600-mg ibupro-
faster in the endovenous obliteration group. All patients
fen tablets, 0.4, SD 0.49, versus 1.3, SD 1.09, P ϭ .004,
were satisfied with the treatment, but one patient in the
endovenous obliteration group and four in the stripping
The sick leaves were significantly shorter in the en-
group were dissatisfied with the cosmetic outcome.
dovenous obliteration group (6.5, SD 3.3, versus 15.6, SD
The cost analysis results showed that the annual cost of
6.0; 95% CI, 5.4 to 12.9; P Ͻ .001, with TT). An even
the VNUS Closure generator was about $3400, which
more distinct difference was seen in the patients’ own
would have meant $120 per operation if all of our trial
assessment of the length of the required sick leave (6.1, SD
operations had been performed with the Closure procedure
4.4, versus 19.2, SD 10.0; 95% CI, 7.2 to 18.9; P ϭ .001,
(Table I). The operative costs of the endovenous oblitera-
with TT). A positive correlation between age and sick leave
tion were significantly higher, mainly because of the cost of
( ϭ 0.37; P ϭ .012) was observed (Appendix B, online
the catheter. However, the combined cost effect of the
additional specialist and the rent of the ultrasound scan
JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 963 Table IV. Quality of life indexes (RAND-36), at baseline and 1 week and 4 weeks postoperatively after surgery Median difference from baseline score (baseline-postoperative value)
Role functioning/emotional 100 (100-100) 100 (67-100)
*Comparison between endovenous obliteration and stripping operation groups (with Mann-Whitney U test). EOG, Endovenous obliteration group; SOG, stripping operation group. Fig 3. Sensitivity analysis of costs of VNUS Closure and conventional surgery in treatment of primary varicose veins in different numbers of patients per year (US dollars).
equipment was much smaller. The effects of the longer
retired, the Closure operation was cost saving (at least 20
operation times in the endovenous obliteration were
patients). The break-even point for 40% of retired patients
quite modest. Although all of the postoperative medical
(60% of indirect costs) was 43 patients. High investment
costs were somewhat higher in the conventional surgery
costs for the generator and the catheter would have raised
group, they did not have any major effect on the total
the Closure cost curves about $370. In the basic alterna-
variable costs of the alternatives. Although the variable
tives, the Closure operation would then have been cost
costs of the conventional operations were about half of
saving at the level of 40 patients per year.
the endovenous obliteration costs, the total societal costsof the conventional operation were at least $300 higher
DISCUSSION
than those of the Closure procedure (Fig 3). Thus, the
This study is the first randomized trial comparing en-
indirect costs had a significant impact on the total soci-
dovenous obliteration with traditional stripping operation
in the treatment of primary varicose veins. According to our
The sensitivity analysis results showed that the use of
findings, endovenous obliteration resulted in less postop-
one specialist in the operation did not change the cost
erative pain, shorter sick leaves, and faster recovery of
curves significantly (Fig 3). The effect of use of only half of
physical function than traditional surgery. Closure proce-
the indirect costs was great, especially in the conventional
dure has higher operating costs but involves potential eco-
group. If half of the indirect costs were included in the cost
nomic advantages for employed patients because of their
analysis, the endovenous obliteration became cost-saving
after about 150 operations per year, with one specialist for
The idea of use of endovenous electrosurgical devices
the operation. The influence of the retired patients on the
for venous wall collagen denaturation is not new. During
indirect costs was also great. If 25% of the patients were
the past few decades, sporadic reports concerning proce-
964 Rautio et al
dures to eliminate truncal or tributary varicosities with
have a significant influence on the results of the cost anal-
monopolar electrosurgical desiccation have been pub-
lished.10-14 The system used in this study (Closure System)
Because the differences in the postoperative pain and
was on the basis of an advanced method, including precise
other complications lasted for only a few weeks, cost com-
heating, feedback controlled with the venous wall temper-
parison and cost minimization analyses are appropriate
methods of economic evaluation.15 In this case, the
The procedures were equally efficient in elimination of
method is closer to cost comparison analysis because of the
reflux in the treated GSV segments. The postoperative
minor differences in the effectiveness of the treatments, at
changes in CEAP classification did not differ, either. The
least according to the short-term results.
overall complication rates were similar in the two groups,
Varicose vein recurrence, defined as the proportion of
although a difference was found in the distribution of the
patients seeking further treatment after apparently ade-
quate surgery, is seen in at least 20% to 30% of the cases and
The endovenous obliteration procedure duration was
tends to increase over time.16 This causes an extra financial
18 minutes longer than the conventional procedure. This
burden on general surgical units and induces costs for
trial was performed partly during the learning curve of
society. Endovenous obliteration omits high ligation and
endovenous obliteration because our surgical team per-
leaves accessory tributaries of the SFJ, which can be re-
formed only 30 procedures before the initiation of this
garded as a risk for recurrence. However, with Closure
study and the experiences from other centers with the
treatment without SFJ ligation, the normal venous drain-
procedure were also dated back only about 2 years. This
age of the lower abdominal and pudendal tissues is pre-
short experience time could have influenced the operating
served. This may reduce the stimulus to neovasculariza-
times and some of the short-term results (ie, complications).
tion.17 Because angiogenesis is regarded as an important
In this study, the minimally invasive nature of the
cause of recurrent reflux,18-21 endovenous obliteration mayactually reduce the risk of recurrent varicosities. Long-term
endovenous obliteration technique resulted in reduced
follow-up periods are, however, needed to better evaluate
postoperative pain and use of analgesics. Almost half of
whether the recurrence rate could be reduced with the
the patients in the stripping group had pain and tension in
the thigh 2 weeks after the operation, which seemed to be
In conclusion, our results indicated that endovenous
the main cause of prolonged sick leaves among these pa-
obliteration may offer an advantage over conventional
tients. In addition, the pain disturbed knee motion and
stripping operation in terms of reduced postoperative pain,
walking, thus delaying the recovery of normal physical
shorter sick leaves, and faster return to normal activities. We
function. However, the lack of blinding in this study may
also conclude that endovenous obliteration was more ex-
likely have had some influence on patients’ subjective eval-
pensive for the hospital. In this study, the total costs, which
uation of postoperative pain. The patients were slightly
also included the costs incurred by society because of sick
older in the stripping group, and a positive correlation
leaves, were no higher than the total costs of the conven-
between age and sick leave emerged. According to the
tional stripping operation. More information is needed on
coefficient of determination, however, age explained only
the long-term results and recurrence rates, and larger stud-
14% of the length of the sick leave. Thus, we believe that the
ies are needed to determine the precise role of this proce-
results were not distorted on the account of this random-
dure in the treatment of primary varicose veins. A thorough
assessment of varicose vein surgery would necessitate a
The patient’s subjective opinions about the appropriate
long-term cost-effectiveness or cost-benefit analysis of
duration of the sick leave were consistent with the sick
leaves actually prescribed. Furthermore, the changes in thehealth-related quality of life parameters, physical function-
We thank the staff of the Day Surgery and Interven-
ing, and bodily pain at 1 week after the procedures support
tional Radiology Units of the Oulu University Hospital for
the reliability of the finding concerning significantly shorter
sick leaves after endovenous obliteration (Appendixes Cand D, online only). REFERENCES
Our sample included employed patients, which in-
1. Laurikka J, Sisto T, Auvinen O, Tarkka M, Laara E, Hakama M.
creased the influence of the indirect costs on the cost
Varicose veins in a Finnish population aged 40-60. J Epidemiol Com-
analysis. The sensitivity analysis showed that even if 25% to
40% of the patients were retired, the Closure operation
2. Davies AH, Steffen C, Cosgrove C, Wilkins DC. Varicose vein surgery:
patient satisfaction. J R Coll Surg Edinb 1995;40:298-9.
could be economically cost-minimizing in the perspective
3. Royle JP. Recurrent varicose veins. World J Surg 1986;10:944-53.
of the society. The possible country-specific differences in
4. Negus D. Recurrent varicose veins: a national problem. Br J Surg
the investment costs and the cost of the catheter have
relatively small effects on the average cost of the Closure
5. Chandler JG, Pichot O, Sessa C, Schuller-Petrovic S, Kabnick LS,
procedure. In addition, because the two alternatives used
Bergan JJ. Treatment of primary venous insufficiency by endovenoussaphenous vein obliteration. Vasc Surg 2000;34:201-4.
about the same amount of other healthcare resources, the
6. Manfrini S, Gasbarro V, Danielsson G, Norgren L, Chandler JG,
differences in the values of the other cost factors do not
Lennox AF, et al. Endovenous management of saphenous vein reflux.
JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 965
Endovenous Reflux Management Study Group. J Vasc Surg 2000;32:
16. Darke SG. The morphology of recurrent varicose veins. Eur J Vasc Surg
7. Porter JM, Moneta GL. Reporting standards in venous disease: an
17. Chandler JG, Pichot O, Sessa C, Schuller-Petrovic S, Osse FJ, Bergan
update. International Consensus Committee on Chronic Venous Dis-
JJ. Defining the role of extended saphenofemoral junction ligation: a
prospective comparative study. J Vasc Surg 2000;32:941-53.
8. Rutherford RB, Padberg FT, Comerota AJ, Kistner RL, Meissner MH,
18. Glass GM. Neovascularization in recurrence of varices of the great
Moneta GL. Venous severity scoring: an adjunct to venous outcome
saphenous vein in the groin: phlebography. Angiology 1988;39(7 Pt
assessment. J Vasc Surg 2000;31:1307-12.
9. Statistical Yearbook of Finland. Helsinki: Painatuskeskus Oy; 2000.
19. Jones L, Braithwaite BD, Selwyn D, Cooke S, Earnshaw JJ. Neovascu-
10. Politowski M, Zelazny T. Complications and difficulties in electroco-
larisation is the principal cause of varicose vein recurrence: results of a
agulation of varices of the lower extremities. Surgery 1966;59:932-4.
randomised trial of stripping the long saphenous vein. Eur J Vasc
11. Watts GT. Endovenous diathermy destruction of internal saphenous. Br
20. Nyamekye I, Shephard NA, Davies B, Heather BP, Earnshaw JJ. Clin-
12. O’Reilly K. Endovenous diathermy sclerosis of varicose veins. Aust N Z
icopathological evidence that neovascularisation is a cause of recurrent
varicose veins. Eur J Vasc Endovasc Surg 1998;15:412-5.
13. Griffith CD, Dennis MJ, Blundell JW, Hopkinson BR. Bipolar dia-
21. Bradbury AW, Stonebridge PA, Callam MJ, Walker AJ, Allan PL, Beggs
thermy treatment of long saphenous vein varicosities. J R Coll Surg
I, et al. Recurrent varicose veins: assessment of the saphenofemoral
14. Gradman WS. Venoscopic obliteration of variceal tributaries using
monopolar electrocautery. Preliminary report. J Dermatol Surg Oncol
Submitted Aug 13, 2001; accepted Dec 3, 2001.
15. Drummond M, OЈBrien B, Stoddart G, Torranca G. Methods for the
economic evaluation of health care programmes. 2nd edition. Oxford:
Additional material for this article may be found onlineAuthors requested to declare conditions of research funding
When sponsors are directly involved in research studies of drugs and devices, the editors will ask authors to clarify theconditions under which the research project was supported by commercial firms, private foundations, or government. Specifically, in the methods section, the authors should describe the roles of the study sponsor(s) and theinvestigator(s) in (1) study design, (2) conduct of the study, (3) data collection, (4) data analysis, (5) datainterpretation, (6) writing of the report, and (7) the decision regarding where and when to submit the report forpublication. If the supporting source had no significant involvement in these aspects of the study, the authors shouldso state.
CUANTÍAS FACTURADAS POR PROVEEDORES 2013 [a 30 de JUNIO de 2013] A28037224 FOMENTO DE CONSTRUCCIONES Y CONTRATAS SAU71068167 EULEN SA ONDEMAND FACILITIES SL UTEA28002335 SDAD IBERICA DE CONSTRUCCIONES ELECTRICAB31954712 LIMPIEZAS PILAR MORENO S.L. G31111768 ASOCIACION BANDA DE MUSICA DE PAMPLONAA31118441 SERVICIOS DE LA COMARCA DE PAMPLONA S.A. F31876436 KAMIRA SOCIEDAD COOPERATIVA DE IN
Prescription Program Formulary — To be used by members who have a formulary drug plan. Anthem Blue Cross and Blue Shield prescription drug benefits include medications available on the Anthem Drug List/Formulary. Our prescription drug benefits can • If you have additional offer potential savings when your physician prescribes medications on the drug list/formulary. questi
 JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 959
JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 959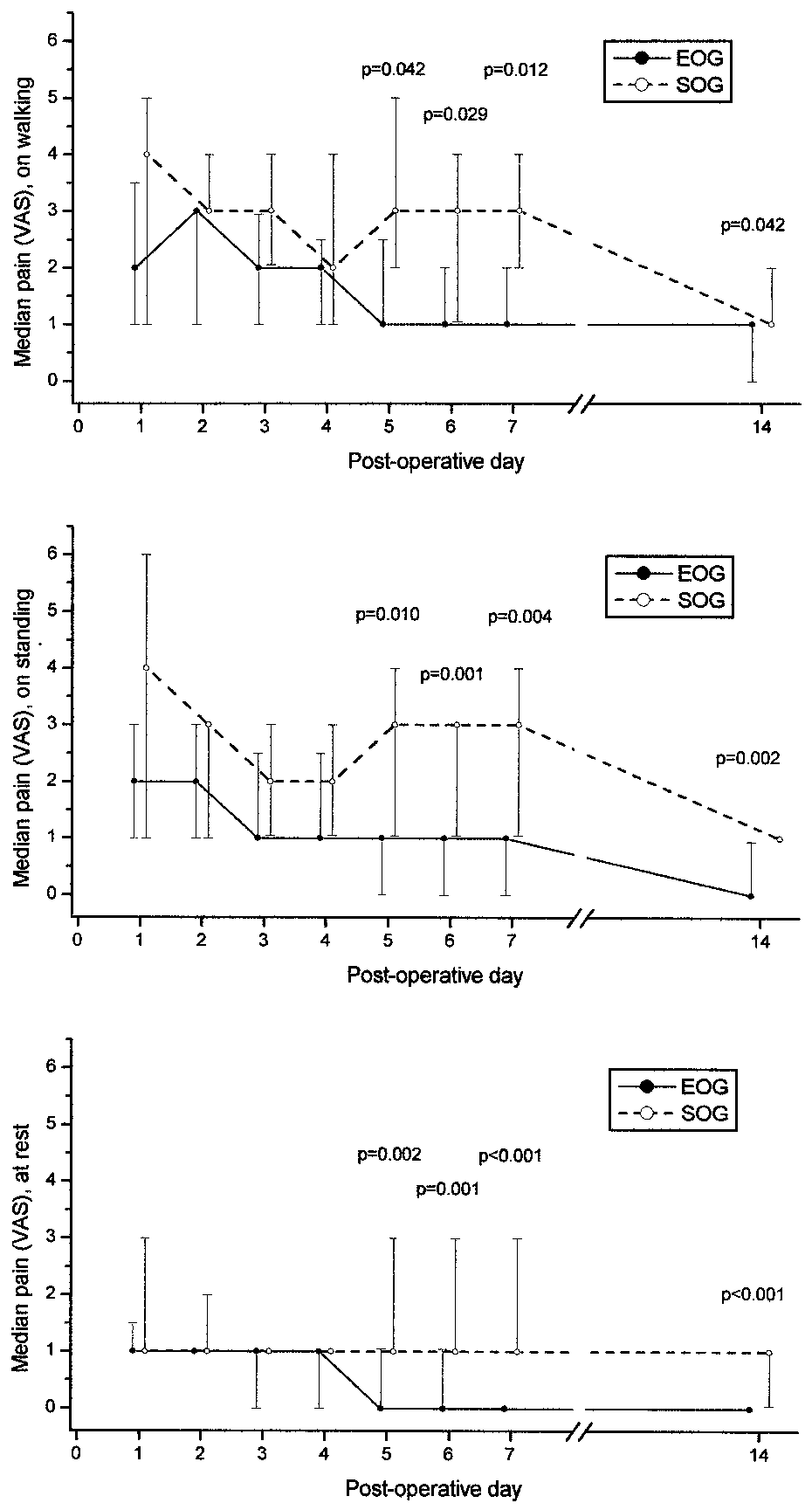 962 Rautio et al
962 Rautio et al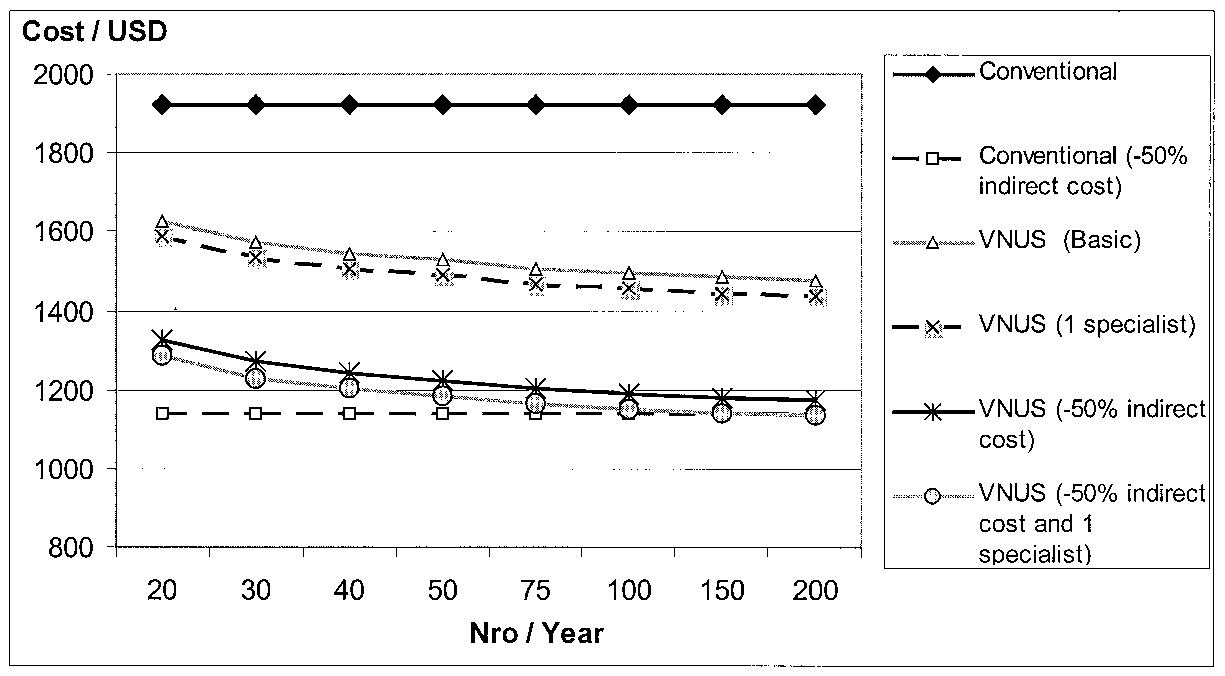 JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 963
JOURNAL OF VASCULAR SURGERYVolume 35, Number 5
Rautio et al 963