He encontrado que alguna farmacia puede tener existencias limitadas de ciertos medicamentos, mientras que otras pueden tener casi cualquier formato que se le ocurra y el habitual de dosis habitualidad apareció. En resumen, siempre se contiene el almacén de corroborar. Al mismo tiempo que el producto que más que gustaba ha resultado no estaba disponible en stock otro distinto por las Buenas costumbres también debe buscarse jefe no asн parezca. Por eso es importante disponer de un Plan B para actuar cuandod ello no ocurra.
Ventaja de tomar un genérico en lugar de Asix
Un genérico es más barato que el nombre de marca
Uno de los mayores incentivos para someterse al Dónde comprar Lasix genérico en lugar de pagar la marca es que usted puede obtener un ahorrando importantes Lasix genérico. Por lo tanto, un Lasix genérico es en general mucho más barato que el homólogo de marca, así que una denominación genérica se hace posible para las personas que usan este medicamento con frecuencia. Un ejemplo: La compra de lurosemida en lugar de Lasix es una considerable ahorro para el presupuesto mensual de medicamentos.
Nephrostomy-tube
GUIDELINE FOR CARE OF A PATIENT WITH A NEPHROSTOMY TUBE
Supporting Policy/ Working in New Ways (WINW) Package Implementation date
Guideline for Care of A Patient with A Nephrostomy Tube (March 2010)
Nursing Practice Guidelines Group, Ward Sisters/Charge Nurses, Practice Development Matrons (PDMs), Clinical Leads, Matrons, Medical Gas Committee.
Further Guidance/Information Urology CNS, Stoma CNS Distribution:
Ward Sisters/Charge Nurses, PDMs, Clinical
Leads, Matrons, Nursing Practice Guidelines Group (includes University of Nottingham representative), Clinical Quality, Risk and Safety Manager, Trust Intranet.
This guideline has been registered with the Trust. However, clinical guidelines are guidelines only. The interpretation and application of clinical guidelines will remain the responsibility of the individual clinician. If in doubt contact a senior colleague or expert. Caution is advised when using the guidelines after the review date.
CARE OF A PATIENT WITH A NEPHROSTOMY TUBE
E. OBTAINING A URINE SAMPLE FROM A NEPHROSTOMY
CARE OF A PATIENT WITH A NEPHROSTOMY TUBE
Best Practice MRSA Screening
All patients must be screened for MRSA prior to insertion or change of a nephrostomy tube.
All patients must have a urine sample taken prior to insertion or change of tube and prior to discharge. Please see Section H
A INTRODUCTION What is a Nephrostomy Tube?
A nephrostomy tube is inserted into the pelvis of the kidney under x-ray control in order to bypass a blockage below. The blockage is usually caused by a stone or tumour in the ureter or bladder causing urine to back up in the kidney. Without this procedure kidney damage can quickly occur. The tube comes out onto the lower back and is kept in place by a locking device within the tube. Although it is unlikely that the tube will fall out, care should still be taken when handling it to avoid displacement. The tubes are designed to stay in place for 3 - 6 months. If the obstruction has not resolved in this time, it will be replaced under x-ray control. These tubes can be temporary (mostly) or permanent (usually for palliative reasons or long term management when all else has failed). B HOW TO CHANGE A POUCH - ASEPTIC TECHNIQUE A one piece urostomy pouch (with a tap at the bottom) is worn to offer some protection against knocking the nephrostomy tube accidentally. Equipment Clean pouch Sterile saline/water Dressing pack Sterile gloves x 3 Apron It is recommended that the pouch be changed three times a week, as the flange will not last more than 2 to 3 days. Leaking urine damages the surrounding skin, which needs to be kept intact in order to allow the flange to stick securely. Any damage to the skin causes discomfort and pain to the patient. PRINCIPLE RATIONALE PRINCIPLE RATIONALE
To minimize risk of cross infection and to comply with infection control policy.
and to comply with infection control policy.(NUH ANTT Policy, 2011
away old pouch using non-alcohol stripping. (Dougherty and Lister, adhesive remover if appropriate,
other hand to prevent skin damage or pulling the tube.
To minimize of cross infection and to comply with infection control policy.
(NUH Hand Hygiene Policy, 2011) (DH, 2007)
The flange and pouch will only stick to clean, dry skin.
To minimize cross infection and to comply with infection control policy.
(NUH Hand Hygiene Policy, 2011) (DH, 2007)
flange and curl, if possible, into top as non-return mechanism stops the section of pouch. The hole in the
Best Practice Use of Leg Bags and Night Bags Some tubes will not curl but will migrate through the gaps past the non- return valve. The use of a leg bag is suggested if this is the case to prevent the above. Night bags should be used for drainage of the system when bed bound or immobile. If the collecting system is detached, then a new leg/night bag should be connected. PRINCIPLE RATIONALE
12. Once in place, use the palm of the The heat of the hand and the patient’s
C GENERAL ADVICE Empty pouch when one third full (if not connected to a leg or night bag), to prevent tension on the appliance. When connecting the pouch to the night/leg bag do not empty the pouch first, allow urine to flow into the night/leg bag as this prevents a vacuum being formed and urine flows easily between the two. Encourage 2-2.5 litres of oral fluid daily to reduce the risk of urinary infections by keeping the kidneys well flushed. The majority of these should be water based, however tea, coffee and fruit juices are acceptable. Patients with a nephrostomy are often able to go home to be nursed in their own environment. Before discharge takes place, it is essential that the following issues are considered:
Has the patient been referred to the Stoma Care Team - ext 56736 or bleep
Has enough equipment been supplied by the hospital until stock can be
Is the patient/carer familiar with equipment to be used and how it works?
Has a district nurse been organized to visit three times weekly?
If a carer is to look after the patients nephrostomy needs, have they been
D HOW TO FLUSH A NEPHROSTOMY TUBE – ASEPTIC TECHNIQUE The tube needs to be checked continuously for drainage of clear urine. If it is suspected that the tube is blocked try flushing it before contacting medical staff. If the patient develops pain over the nephrostomy site, this should be investigated as this may be a symptom of a blocked tube. Equipment Clean pouch Sterile water 10 ml (for flushing) Sterile saline/water (for cleaning) 5-10 ml sterile syringe Sterile gloves x 3 Dressing pack Alcohol wipe Apron PRINCIPLE RATIONALE
To minimize cross infection and to comply with infection control policy.
away old pouch using non-alcohol stripping. (Dougherty and Lister, adhesive remover if appropriate,
other hand to prevent skin damage or pulling the tube.
PRINCIPLE RATIONALE
To minimize cross infection and to comply with infection control policy.
To minimize cross infection and to comply with infection control policy.
or Chlorhexidine and alcohol wipe and allow to dry.
To check obvious reasons for non-drainage of tube initially.
Ensure luerlock cap has been removed (used to block off the tube when required).
risk of deposits/stones). Disconnect syringe from tube and allow urine to run back into receptacle. Pulling back on syringe slowly may help dislodge a blockage but excess force can cause bleeding. Flushing again with 5 ml of water can be carried out if necessary.
PRINCIPLE RATIONALE
To minimize risk of cross infection and to comply with infection control policy.
Encourage patient to drink a glass of water if appropriate.
Best Practice Always check the tube is draining before you leave the patient. A blocked Nephrostomy tube can cause lower back pain, hydronephrosis (inflammation of the kidney), sepsis and eventually kidney failure. FLEXIMA 8 fr NB The locking device refers to the locking mechanism holding the tube in place in the kidney. It is not a valve to control the flow of urine. Do not touch it when flushing the tube. E OBTAINING A URINE SAMPLE FROM A NEPHROSTOMY TUBE – ASEPTIC TECHNIQUE If a urine infection is suspected Equipment Clean pouch Sterile universal pot Alcohol wipe Sterile saline/water Dressing pack Sterile gloves x 3 Apron PRINCIPLE RATIONALE
To minimize cross infection and to comply with infection control policy.
away old pouch using non-alcohol stripping. (Dougherty and Lister, adhesive remover if appropriate,
other hand to prevent skin damage or pulling the tube.
To minimize cross infection and to comply with infection control policy.
To minimize cross infection and to comply with infection control policy.
PRINCIPLE RATIONALE
or alcohol and Chlorhexidine wipe and allow to dry.
tube, allow urine to drip into the sterile, universal pot.
Best Practice Symptoms of an infection include blood stained urine, offensive smelling urine, flu-like symptoms, lower back pain, rigors and a temperature. Treat according to culture and sensitivity result.
F TROUBLESHOOTING Problem Cause
If red/sore skin is identical to the shape of the flange, contact Stoma Care Team for alternative equipment. Apply skin protective wipe, e.g. Cavilon.
nodular type appearance around the site of the tube. It may bleed and/or cause discomfort.)
G POLICY FOR MRSA SCREENING Please adhere to the Nottingham University Hospitals policy (2010) for Meticillin Resistant Staphylococcus Aureus (MRSA). The latest information on screening and decolonization can be found on the NUH Infection Prevention and Control intranet site. MRSA is a bacterium that is resistant to several antibiotics, notably Flucloxacillin, that would be commonly be used to treat staphylococcus aureus infections. MRSA infections cause significant morbidity and mortality and the mortality for MRSA bacteraemia is greater than that from Meticillin Sensitive Staphylococcus Aureus bacteraemia (MSSA). Patients with MRSA surgical site infections have been shown to have a prolonged hospital stay and higher mortality. MRSA is readily transmitted between patients. Inpatients who are colonized or infected with MRSA must have appropriate infection control special precautions taken to prevent spread to other patients. The Department of Health have required that all NHS Hospitals must have in place MRSA screening for all elective patients by April 2009 and for all emergency patients by April 2011 (DoH, 2007). All staff who have contact with MRSA positive patients have a responsibility to ensure that they adhere to the necessary wound and skin precautions as advised by the Infection Prevention and Control Team (IPCT). Screening swabs should be taken from patients whether elective or an emergency who are about to undergo insertion of a nephrostomy tube. This includes replacement of an existing nephrostomy tube. Screening should ideally occur 2-4 weeks prior to the procedure taking place, with the goal of decolonization occurring pre-admission also. In the event that this has not occurred pre-admission, screening must take place upon arrival to the ward.
Screening involves:- Screening patients with no existing nephrostomy tube present:
Screening patients with existing nephrostomy tube in situ who are scheduled for replacement tube: The patient requires a FULL MRSA screen including:
Sample of urine from existing nephrostomy tube (see page 10 referring to
If screening has taken place by GP prior to admission, communications about screening results need to take place from healthcare profession to healthcare professional, and not just from the patient. If the urine sample is positive for MRSA, the new nephrostomy tube is likely to become infected. Antibiotic therapy to protect the new nephrostomy must be considered and discussed with the Microbiology Team. Best Practice The procedure should not be carried out until the correct screening has taken place.
If patient is an existing MRSA carrier, then all other routine swabs should be taken as per policy prior to this procedure, and alternatives considered to usual first line Ciprofloxacillin antibiotic treatment.
Post insertion of tube, if the patient is to remain in hospital, samples of urine from the nephrostomy tube and site should be taken immediately prior to discharge. MRSA status and confirmation of screening should be identified and reported to the appropriate District Nursing Teams to aide communication. Decolonization Treatment
If Nose and/or perineum swabs are positive on screening then a 5 day
decolonization treatment with nasal Bactroban (three times per day) and Chlorhexidine body wash (once daily including the washing of hair twice in the 5 days) is indicated.
If the nephrostomy site is found to be positive for MRSA then a daily
application of Bactroban to the nephrostomy site is recommended to coincide with the 5 day general skin decolonization treatment with nasal Bactroban and Chlorhexidine body wash. This decolonization treatment must also be instigated when the nose and perineum are negative and only the nephrostomy site is found to be positive
Long term use of Bactroban/Chlorhexidine or other alternative skin decolonization treatments such as Naseptin or Stellisept is not recommended and can cause problems with resistance.
H REFERENCES Department of Health (2007) Saving Lives: reducing infection, delivering clean safe care (revised edition), London, Crown Copyright. Dougherty, L. Lister, S. (2008) The Royal Marsden Hospital Manual of Nursing Procedures 7th P.365-370 Ed. Wiley Blackwell, Oxford. Nottingham University Hospitals NHS Trust (2008) Hand Hygiene Policy. Nottingham University Hospitals NHS Trust (2008) Glove Selection Guidelines. Nottingham University Hospitals NHS Trust (2010) Meticillin Resistant Staphylococcus Aureus (MRSA) Policy. Nottingham University Hospitals NHS Trust (2011) Aseptic Non-Touch Technique (ANTT) Policy.
Resolution 2011-2 RESOLUCIÓN SOBRE SEGURIDAD EN ALTA MAR CONSIDERANDO que la seguridad de los buques y tripulaciones, el orden de la navegación marítima y la protección ambiental son, y por mucho tiempo han sido, intereses comunes de las naciones alrededor del mundo; CONSIDERANDO que la Comisión y los Gobiernos Contratantes apoyan el derecho a las formas legítimas y pacífic
SUSPENSION TRAUMA Suspension trauma, or orthostatic intolerance, is a natural human reaction to being upright and immobile, where a complex combination of blood pooling in the legs and cardiorespiratory restriction leads to unconsciousness. It can be caused by suspension in a harness (deliberate or accidental), when trapped in a confined space, when secured to a vertical stretcher or litter -
 GUIDELINE FOR CARE OF A PATIENT WITH A NEPHROSTOMY TUBE
GUIDELINE FOR CARE OF A PATIENT WITH A NEPHROSTOMY TUBE  CARE OF A PATIENT WITH A
CARE OF A PATIENT WITH A  CARE OF A PATIENT WITH A
CARE OF A PATIENT WITH A 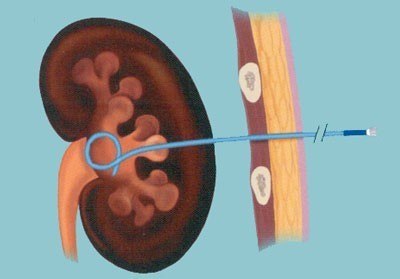 B HOW TO CHANGE A POUCH - ASEPTIC TECHNIQUE
B HOW TO CHANGE A POUCH - ASEPTIC TECHNIQUE 
 FLEXIMA 8 fr
FLEXIMA 8 fr